[level-membership-for-basic-science-category]
Chapter 7 Toxicology
 Descriptive toxicology focuses on toxicity testing with the intent of defining the degree of risk associated with substances.
Descriptive toxicology focuses on toxicity testing with the intent of defining the degree of risk associated with substances.




General Principles






General Mechanisms of Toxicity








Target Organs
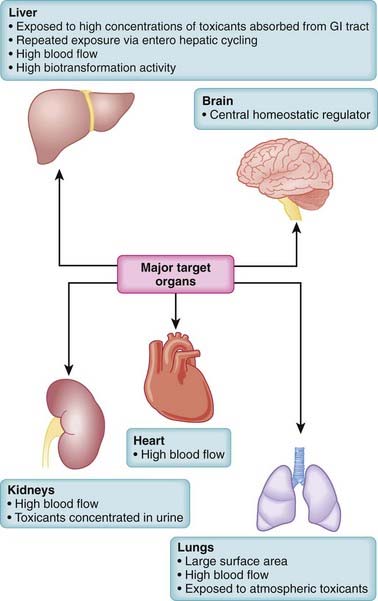
Toxicity may be systemic, affecting the whole body, or it may be largely confined to select target organs, the so-called toxic effect organs. Some organs, such as the liver, brain, lungs, heart, and kidney, play a central role in poisonings (Figure 7-1). When toxicity is site specific, the word toxic is preceded by an indication of the specific target organ. Thus, hepatotoxicity refers to effects on the liver, nephrotoxicity refers to effects on the kidney, ototoxicity refers to effects on the auditory system, and so on. A number of factors interact to determine the susceptibility of organs to toxic effects. These include the organ’s anatomic location, blood flow, metabolic processes and activity, affinity for the toxicant, and capacity for self-repair. Major toxic effect organs include the following:
 Liver. The liver is exposed to a high concentration of toxic substances. Orally absorbed toxicants are presented first to the liver via the portal circulation. The liver also receives a large proportion of systemic blood flow. Enterohepatic cycling extends exposure to toxicants excreted through the bile. The high metabolic activity of the liver also results in the generation of reactive intermediates that may have toxic actions.
Liver. The liver is exposed to a high concentration of toxic substances. Orally absorbed toxicants are presented first to the liver via the portal circulation. The liver also receives a large proportion of systemic blood flow. Enterohepatic cycling extends exposure to toxicants excreted through the bile. The high metabolic activity of the liver also results in the generation of reactive intermediates that may have toxic actions.



Risk Assessment
Because virtually all substances are potentially toxic, key questions in toxicology are how much risk is associated with a particular substance and under what conditions does this risk become apparent? In addition, the level of acceptable risk will vary. In some circumstances, very toxic substances (e.g., anticancer drugs) are used therapeutically despite their known toxic effects because the benefits of such treatments outweigh the risks. Accordingly, risk assessment is a primary consideration in the management of toxic events (Figure 7-2).
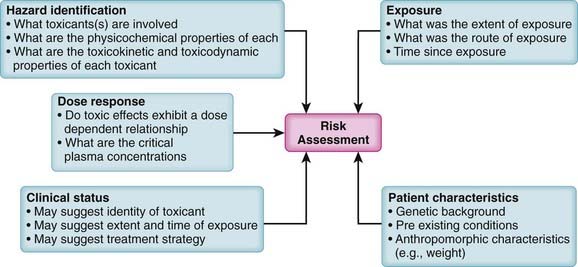
Key factors contributing to risk assessment include the following:
 Hazard identification. What substances are involved and what are the adverse effects of each substance? Knowledge of the physicochemical properties, toxicokinetics, and toxicodynamics of the suspected toxicant(s) is invaluable in designing treatment strategies.
Hazard identification. What substances are involved and what are the adverse effects of each substance? Knowledge of the physicochemical properties, toxicokinetics, and toxicodynamics of the suspected toxicant(s) is invaluable in designing treatment strategies.
 Exposure assessment. Exposure assessment is a key process in determining the urgency and strategy for treatment of toxic events. Exposure assessment includes estimation of the following:
Exposure assessment. Exposure assessment is a key process in determining the urgency and strategy for treatment of toxic events. Exposure assessment includes estimation of the following:

 Time since exposure. An estimate of the time since the exposure will be helpful in estimating the following:
Time since exposure. An estimate of the time since the exposure will be helpful in estimating the following:


General Strategies for Management of Toxic Events
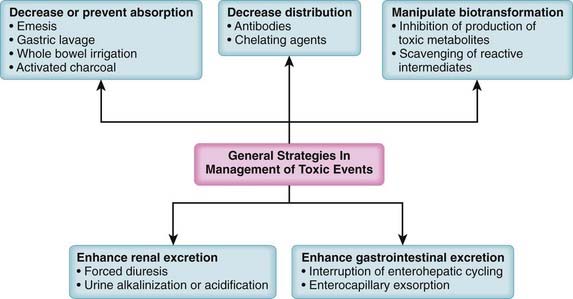
 Antibodies that neutralize toxicants or prevent their distribution to target organs (e.g., antivenin for snake bites)
Antibodies that neutralize toxicants or prevent their distribution to target organs (e.g., antivenin for snake bites)






In addition to specific treatments, a number of generalized treatment strategies can be used in poisonings (Figure 7-3). These are toxicokinetic treatment strategies targeted at reducing or preventing the absorption of the toxicant, at reducing the distribution of the toxicant, at manipulating biotransformation to reduce formation of the toxicant, or at hastening excretion of the toxicant. These approaches rely heavily on the concepts of pharmacokinetics presented earlier, which will not be repeated here. These generalized approaches are very useful in situations in which there are no specific antidotes or the causative toxicant(s) and/or modes of action are not sufficiently well defined to allow application of a specific antidote.
Reduction or Prevention of Absorption

















Gastric Lavage










Activated Charcoal
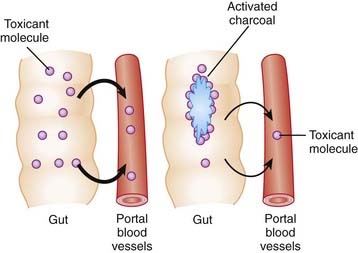
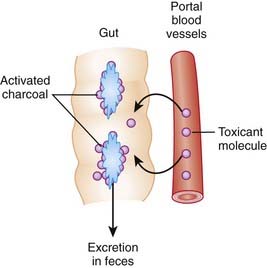
Activation of charcoal by oxidization increases its adsorptive surface area. The large surface area of charcoal is capable of adsorbing many toxicants, thus sequestering them in the gut. Because only free molecules are able to diffuse across membranes, reduction of the concentration of free toxicant in the gut by charcoal greatly reduces absorption into the bloodstream (Figure 7-4). This treatment is administered as a slurry of the activated charcoal powder.































Manipulation of Distribution
 General mechanisms of action
General mechanisms of action
 Antibodies
Antibodies






 Edetate calcium disodium (calcium disodium salt of ethylenediaminetetraacetic acid; EDTA)
Edetate calcium disodium (calcium disodium salt of ethylenediaminetetraacetic acid; EDTA)
 Dimercaprol (British antilewisite)
Dimercaprol (British antilewisite)











 Deferoxamine
Deferoxamine
















Enhancement of Toxin Excretion
Renal Excretion
Forced Diuresis




Urine Alkalinization
 As discussed in the pharmacokinetics chapter, many substances are reabsorbed from the renal tubules into the bloodstream, limiting the extent of their urinary excretion.
As discussed in the pharmacokinetics chapter, many substances are reabsorbed from the renal tubules into the bloodstream, limiting the extent of their urinary excretion.


















Gastrointestinal Excretion
Interruption of Enterohepatic Cycling
 Activated charcoal, particularly MDAC, may increase toxicant elimination in part by interrupting enterohepatic cycling.
Activated charcoal, particularly MDAC, may increase toxicant elimination in part by interrupting enterohepatic cycling.


Enterocapillary Exsorption (Gastrointestinal Dialysis)

 The very low concentration of free toxicant in the gut lumen means that free toxicant concentrations in the plasma are higher than those in the gut. This blood-to-gut concentration gradient favors diffusion of toxicant from the blood into the gut lumen where the toxicant binds to the charcoal. The charcoal-bound toxicant is eventually excreted in the feces (Figure 7-5). As this cycle repeats itself, the blood is cleared of toxicant.
The very low concentration of free toxicant in the gut lumen means that free toxicant concentrations in the plasma are higher than those in the gut. This blood-to-gut concentration gradient favors diffusion of toxicant from the blood into the gut lumen where the toxicant binds to the charcoal. The charcoal-bound toxicant is eventually excreted in the feces (Figure 7-5). As this cycle repeats itself, the blood is cleared of toxicant.




Pharmacologic Treatment of Specific Intoxications
Analgesics
Intoxication with analgesics represents the most common form of toxicity requiring hospitalization.
Acetaminophen
 Acetaminophen poisoning causes hepatotoxicity and is one of the more common lethal poisonings in industrialized countries.
Acetaminophen poisoning causes hepatotoxicity and is one of the more common lethal poisonings in industrialized countries.
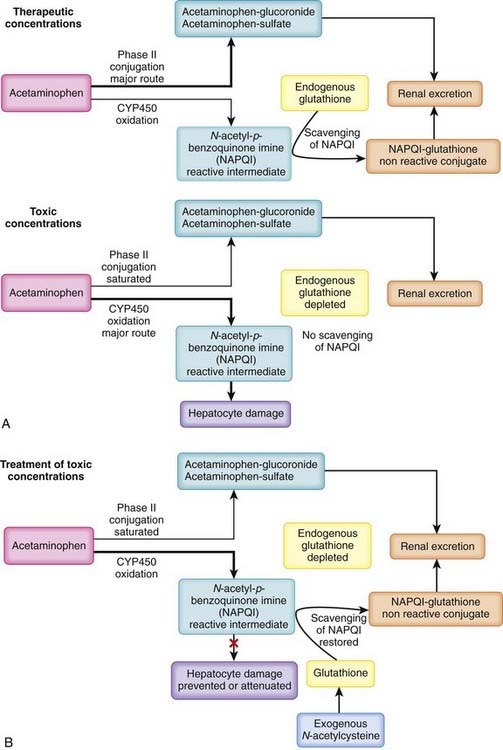
 Acetaminophen is not toxic per se but is metabolized to a reactive intermediate that is toxic (Figure 7-6, A).
Acetaminophen is not toxic per se but is metabolized to a reactive intermediate that is toxic (Figure 7-6, A).
 At therapeutic concentrations:
At therapeutic concentrations:




 Treatment of acetaminophen poisoning
Treatment of acetaminophen poisoning

 N-acetylcysteine (NAC). A primary treatment strategy for acetaminophen toxicity is replenishment of cellular glutathione via the administration of NAC, a precursor of glutathione (see Figure 7-6, B).
N-acetylcysteine (NAC). A primary treatment strategy for acetaminophen toxicity is replenishment of cellular glutathione via the administration of NAC, a precursor of glutathione (see Figure 7-6, B).







Salicylates



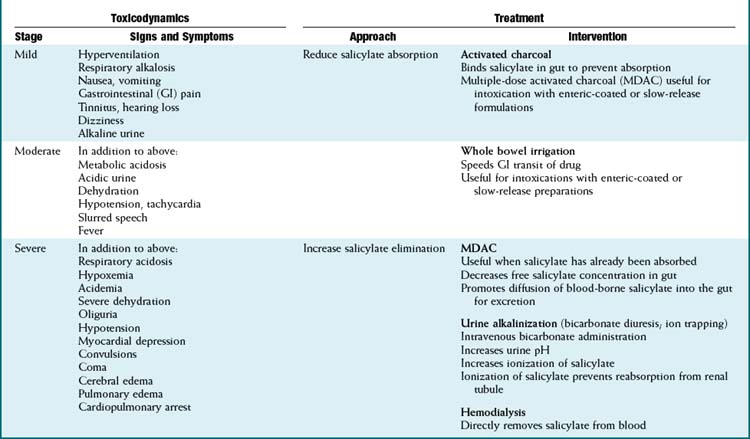
 Salicylate toxicity (Table 7-1)
Salicylate toxicity (Table 7-1)
 The widespread availability of salicylate preparations has resulted in a relatively high incidence of salicylate poisoning. Acute ingestion of toxic quantities may occur in accidental overdoses or in suicide attempts. Toxicity may also occur chronically because at high therapeutic doses (e.g., antiinflammatory doses) elimination mechanisms are nearly or completely saturated and salicylates exhibit zero-order kinetics. Some of the early-phase signs and symptoms of salicylate poisoning (see later) may be apparent at high therapeutic doses.
The widespread availability of salicylate preparations has resulted in a relatively high incidence of salicylate poisoning. Acute ingestion of toxic quantities may occur in accidental overdoses or in suicide attempts. Toxicity may also occur chronically because at high therapeutic doses (e.g., antiinflammatory doses) elimination mechanisms are nearly or completely saturated and salicylates exhibit zero-order kinetics. Some of the early-phase signs and symptoms of salicylate poisoning (see later) may be apparent at high therapeutic doses.


 Accumulation of free salicylic acid has several toxic effects, which include:
Accumulation of free salicylic acid has several toxic effects, which include:














 Salicylate poisoning is progressive. The early (mild) phase involves:
Salicylate poisoning is progressive. The early (mild) phase involves:







 The moderate phase of salicylate poisoning involves:
The moderate phase of salicylate poisoning involves:





 The severe (late) phase of salicylate poisoning involves:
The severe (late) phase of salicylate poisoning involves:







 Treatment of salicylate poisoning
Treatment of salicylate poisoning











Opioid Analgesics



 Treatment of opioid toxicity
Treatment of opioid toxicity


 Opioid receptor antagonists
Opioid receptor antagonists


Ethylene Glycol, Methanol
 Although relatively infrequent, intoxication with alcohols such as ethylene glycol and methanol can result in a high rate of mortality if not treated appropriately.
Although relatively infrequent, intoxication with alcohols such as ethylene glycol and methanol can result in a high rate of mortality if not treated appropriately.

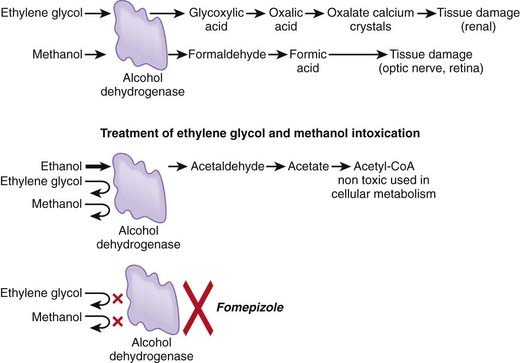
 Neither ethylene glycol nor methanol is particularly toxic per se, but these compounds are biotransformed into toxic metabolites (Figure 7-7).
Neither ethylene glycol nor methanol is particularly toxic per se, but these compounds are biotransformed into toxic metabolites (Figure 7-7). Ethylene glycol
Ethylene glycol







Treatment of Ethylene Glycol or Methanol Poisoning
 Inhibition of metabolite formation
Inhibition of metabolite formation
 Ethanol (ethyl alcohol)
Ethanol (ethyl alcohol)



 Fomepizole
Fomepizole



Cardiac Glycosides



 Cardiac glycoside toxicity
Cardiac glycoside toxicity


 Treatment of cardiac glycoside toxicity
Treatment of cardiac glycoside toxicity

 Manipulation of distribution or enhancement of elimination
Manipulation of distribution or enhancement of elimination
Pesticides
 Many pesticides act as inhibitors of acetylcholinesterase, the endogenous enzyme responsible for the degradation of acetylcholine.
Many pesticides act as inhibitors of acetylcholinesterase, the endogenous enzyme responsible for the degradation of acetylcholine.

 Toxicity of organophosphate and carbamate pesticides
Toxicity of organophosphate and carbamate pesticides
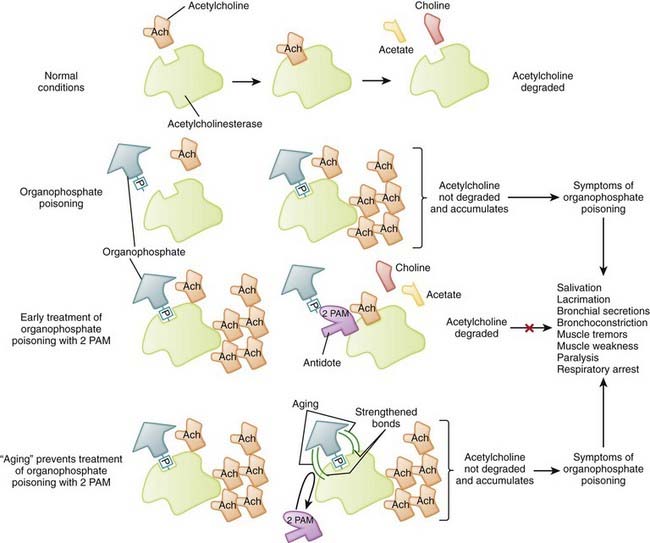
 The primary mechanism of action of these agents is inhibition of acetylcholinesterase, the enzyme responsible for degrading acetylcholine into choline and acetate, with the resultant accumulation of acetylcholine (ACh) in neuroeffector junctions. Overstimulation of cholinergic receptors is responsible for the signs and symptoms and toxicity of organophosphate and carbamate poisoning (Figure 7-8).
The primary mechanism of action of these agents is inhibition of acetylcholinesterase, the enzyme responsible for degrading acetylcholine into choline and acetate, with the resultant accumulation of acetylcholine (ACh) in neuroeffector junctions. Overstimulation of cholinergic receptors is responsible for the signs and symptoms and toxicity of organophosphate and carbamate poisoning (Figure 7-8). Excess acetylcholine results in overstimulation of cholinergic muscarinic and nicotinic receptors in various tissues.
Excess acetylcholine results in overstimulation of cholinergic muscarinic and nicotinic receptors in various tissues.





 Treatment of organophosphate and carbamate pesticide toxicity
Treatment of organophosphate and carbamate pesticide toxicity





Calcium Channel Blockers and β-Blockers
 Calcium channel blockers are prescribed for a number of cardiovascular conditions (e.g., angina, hypertension, tachycardia).
Calcium channel blockers are prescribed for a number of cardiovascular conditions (e.g., angina, hypertension, tachycardia).

 Toxicity of calcium channel blockers and β-blockers
Toxicity of calcium channel blockers and β-blockers




 Treatment of calcium channel blocker and β-blocker toxicity
Treatment of calcium channel blocker and β-blocker toxicity



 Physiologic treatments
Physiologic treatments






American Association of Poison Control Centers. www.aapcc.org
Canadian Association of Poison Control Centres. www.capcc.ca/resources/resources.php
Glossary of toxicologic terms Glossary of toxicologic terms. http://sis.nlm.nih.gov/enviro/iupacglossary/frontmatter.html
National Library of Medicine (U.S.). www.toxnet.nlm.nih.gov
National Toxicology Program (U.S.). http://cerhr.niehs.nih.gov/reports/index.html
World Health Organization. www.who.int/ipcs/poisons/centre/directory/en/index.html
[/level-membership-for-basic-science-category][not-level-membership-for-basic-science-category]
Chapter 7 Toxicology
Descriptive toxicology focuses on toxicity testing with the intent of defining the degree of risk associated with substances.General Principles
General Mechanisms of Toxicity
Target Organs
Toxicity may be systemic, affecting the whole body, or it may be largely confined to select target organs, the so-called toxic effect organs. Some organs, such as the liver, brain, lungs, heart, and kidney, play a central role in poisonings (Figure 7-1). When toxicity is site specific, the word toxic is preceded by an indication of the specific target organ. Thus, hepatotoxicity refers to effects on the liver, nephrotoxicity refers to effects on the kidney, ototoxicity refers to effects on the auditory system, and so on. A number of factors interact to determine the susceptibility of organs to toxic effects. These include the organ’s anatomic location, blood flow, metabolic processes and activity, affinity for the toxicant, and capacity for self-repair. Major toxic effect organs include the following:
Liver. The liver is exposed to a high concentration of toxic substances. Orally absorbed toxicants are presented first to the liver via the portal circulation. The liver also receives a large proportion of systemic blood flow. Enterohepatic cycling extends exposure to toxicants excreted through the bile. The high metabolic activity of the liver also results in the generation of reactive intermediates that may have toxic actions.Risk Assessment
Because virtually all substances are potentially toxic, key questions in toxicology are how much risk is associated with a particular substance and under what conditions does this risk become apparent? In addition, the level of acceptable risk will vary. In some circumstances, very toxic substances (e.g., anticancer drugs) are used therapeutically despite their known toxic effects because the benefits of such treatments outweigh the risks. Accordingly, risk assessment is a primary consideration in the management of toxic events (Figure 7-2).
Key factors contributing to risk assessment include the following:
Hazard identification. What substances are involved and what are the adverse effects of each substance? Knowledge of the physicochemical properties, toxicokinetics, and toxicodynamics of the suspected toxicant(s) is invaluable in designing treatment strategies. Exposure assessment. Exposure assessment is a key process in determining the urgency and strategy for treatment of toxic events. Exposure assessment includes estimation of the following:
Time since exposure. An estimate of the time since the exposure will be helpful in estimating the following:
General Strategies for Management of Toxic Events
Antibodies that neutralize toxicants or prevent their distribution to target organs (e.g., antivenin for snake bites)In addition to specific treatments, a number of generalized treatment strategies can be used in poisonings (Figure 7-3). These are toxicokinetic treatment strategies targeted at reducing or preventing the absorption of the toxicant, at reducing the distribution of the toxicant, at manipulating biotransformation to reduce formation of the toxicant, or at hastening excretion of the toxicant. These approaches rely heavily on the concepts of pharmacokinetics presented earlier, which will not be repeated here. These generalized approaches are very useful in situations in which there are no specific antidotes or the causative toxicant(s) and/or modes of action are not sufficiently well defined to allow application of a specific antidote.
Reduction or Prevention of Absorption
Gastric Lavage
Activated Charcoal
Activation of charcoal by oxidization increases its adsorptive surface area. The large surface area of charcoal is capable of adsorbing many toxicants, thus sequestering them in the gut. Because only free molecules are able to diffuse across membranes, reduction of the concentration of free toxicant in the gut by charcoal greatly reduces absorption into the bloodstream (Figure 7-4). This treatment is administered as a slurry of the activated charcoal powder.
