Published on 18/03/2015 by admin
Filed under Dermatology
Last modified 22/04/2025
This article have been viewed 2466 times
Joshua A. Zeichner
Evidence Levels: A Double-blind study B Clinical trial ≥ 20 subjects C Clinical trial < 20 subjects D Series ≥ 5 subjects E Anecdotal case reports
Radiation dermatitis is a potential complication of cutaneous radiation exposure, most commonly from interventional radiologic procedures or treatment of malignancies. Appendageal structures and basal layer cells are the most sensitive to radiation exposure. Their damage leads to acute skin changes, including pruritus, desquamation, erythema, epilation, edema, and blistering. Atrophy, dyspigmentation, telangiectasia, fibrosis, ulceration, and necrosis are later effects resulting from dermal and vascular damage. Radiation recall is a dermatitis developing at sites of previous radiation exposure, usually induced by chemotherapeutic drugs such as doxorubicin or dactinomycin.
Severity of skin changes correlates with the cumulative dose of ionizing radiation, therefore minimizing exposure is important. While exposure to high levels of radiation is important in some cancer treatment algorithms, treatment of the skin consists of supportive care, pain control, and prevention of infection. Maintaining skin integrity, improving patient comfort, and reducing infection risk and skin trauma are keys to improving outcomes. Cornstarch and emollient creams treat dry desquamation (painless peeling of the skin), while moist desquamation (painful, full-thickness loss of the epidermis) should be treated with occlusive dressings and care to prevent infections. Topical corticosteroids control pruritus and reduce inflammation. Patients should also avoid friction from tight-fitting clothing. Topical antifungal ointments treat and may provide prophylaxis against fungal infections, especially in the intertriginous areas. Patients may gently wash the skin with water and mild soap. In addition, a topical trolamine-containing cream (Biafine) has been shown to improve wound healing and has been used in acute radiation dermatitis.
Like acute changes, chronic radiation dermatitis is treated symptomatically. Topical emollient creams and corticosteroids can be employed as needed. Skin necrosis or ulceration must be carefully monitored for signs of infection. Some recommend physical massage of the skin to improve fibrosis.
History of previous radiation exposure and chemotherapeutic drugs
Evaluation of affected skin for development of malignancy
Maalej M, Frikha H, Kochbati L, Bouaouina N, Sellami D, Benna F, et al. Cancer Radiother 2004; 8: 81–7.
Basal cell carcinomas are the most common malignancies to develop in the skin at sites of previous radiation exposure, especially on the head and the neck.
McQuestion M. Semin Oncol Nurs 2011; 27: e1–17.
There is minimal evidence available to guide the management of skin reactions that result from radiation exposure. This paper reviews the available reports of topical treatments for radiation dermatitis.
Bolderston A, Lloyd NS, Wong RK, Holden L, Robb-Blenderman L; Supportive Care Guidelines Group of Cancer Care Ontario Program in Evidence-Based Care. Support Care Cancer 2006; 14: 802–17.
This article reviews the literature, and the authors conclude that gentle washing of the skin with water alone, or with mild soap, may help prevent acute radiation dermatitis.
There is not enough evidence to make conclusions on the efficacy of topical or oral agents. However, plain, fragrance- and lanolin-free emollient creams as well as mild corticosteroid creams may be beneficial.
Schmuth M, Wimmer MA, Hofer S, Sztankay A, Weinlich G, Linder DM, et al. Br J Dermatol 2002; 146: 983–91.
Neither topical corticosteroids nor dexpanthenol prevented the onset of radiation dermatitis. However, both reduced the severity of the skin changes, more so in the topical corticosteroids group than the dexpanthenol group.
Pommier P, Gomez F, Sunyach MP, D’Hombres A, Carrie C, Montbarbon X. J Clin Oncol 2004; 22: 1447–53.
In this study, acute radiation dermatitis developed in a higher percentage of patients using trolamine emulsion than in those using topical calendula.
Del Rosso JQ, Bikowski J. Cutis 2008; 8: 209–14.
Trolamine emulsion has been used to improve wound healing by expedited the formation of granulation tissue and new collagen. It has also been used in patients post-radiation therapy.
Lokkevik E, Skovlund E, Reitan JB, Hannisdal E, Tanum G. Acta Oncol 1996; 35: 1021–6.
This study demonstrated the efficacy of dexpanthenol-containing cream in treating radiation dermatitis.
Hemati S, Asnaashari O, Sarvizadeh M, Motlagh BN, Akbari M, Tajvidi M, et al. Support Care Cancer 2012; 20: 1613–18.
Topical silver sulfadiazine (SSD) 1% cream was applied to three times a day, 3 days a week, for 5 weeks and three times a day for 1 week after evaluation in women receiving radiation for breast cancer. Patients using the SSD cream developed significantly less severe dermatitis compared to controls that were treated with general skin care alone.
Vavassis P, Gelinas M, Chabot Tr J, Nguyen-Tân PF. J Otolaryngol 2008; 37: 124–9.
In this study, silver leaf dressings seem to reduce the severity of skin reactions after radiation. In addition, it accelerated healing and provided improved pain control. The results of the study warrants further investigation.
Vuong T, Franco E, Lehnert S, Lambert C, Portelance L, Nasr E, et al. Int J Radiat Oncol Biol Phys 2004; 59: 809–14.
Silver leaf nylon dressings have antimicrobial and healing properties in patients with skin burns and grafts. This study suggested that silver leaf nylon dressings are also effective in reducing radiation dermatitis, perhaps owing to their antimicrobial properties.
Matceyevsky D, Hahoshen NY, Vexler A, Noam A, Khafif A, Ben-Yosef R. Israel Med Assoc J 2007; 9: 439–42.
In this phase II study from Israel, products made using water from the Dead Sea were shown to reduce skin and mucosal toxicity in patients receiving radiation and chemotherapy for cancers of the head and neck.
Kouvaris J, Kouloulias V, Kokakis J, Matsopoulos G, Myrsini B, Vlahos L. Eur J Dermatol 2002; 12: 458–62.
Amifostine is a cytoprotective drug used to reduce toxicities from cancer chemotherapy and radiation therapy. In this retrospective analysis, the authors found a significant protective effect in the skin in patients receiving radiation therapy.
Aygenc E, Celikkanat S, Kaymakci M, Aksaray F, Ozdem C. Otolaryngol Head Neck Surg 2004; 130: 351–6.
Many late changes in radiation dermatitis are thought to be due to vascular insufficiency. In this trial, the group taking pentoxifylline had less severe fibrosis and necrosis than the placebo group. This report is the only case series of its kind in the literature.
Pentoxifylline is still under investigation for this application. Confirmatory studies have not yet been published.
Liang L, Hu D, Liu W, Williams JP, Okunieff P, Ding I. Am J Clin Oncol 2003; 26: S114–21.
In a mouse model, celecoxib was shown to reduce necrosis, inflammatory infiltrate, and chemokine expression in irradiated skin. This effect was selective for the skin, without affecting the irradiated tissue of the tumor in question.
Cyclo-oxygenase-2 (COX-2) inhibitors are currently not a standard part of treatment for radiation dermatitis, but this discovery warrants further investigation.
Uzaraga I, Gerbis B, Holwerda E, Gillis D, Wai E. Support Care Cancer 2012; 20: 1515–24.
This pilot study of 16 patients assessed a topical preparation of amitriptyline, ketamine, and lidocaine (AKL) to reduce neuropathic pain from radiation dermatitis. The cream was applied to affected areas three times a day daily until 2 weeks post-radiotherapy. AKL was shown to reduce burning levels. A larger-scale study is needed to further evaluate these results.
Barnea Y, Amir A, Shafir R, Weiss J, Gur E. Ann Plast Surg 2002; 49: 668–72.
The authors present two patients with painful, non-healing wounds at the site of chronic radiation dermatitis. The patients underwent wound excision with skin grafting. The skin healed completely, but the pain was only partially relieved. In practice, skin grafting is extremely rare.
Treatment of Skin Disease Comprehensive Therapeutic Strategies 4e
WhatsApp us
 Silver leaf dressings (under investigation)
Silver leaf dressings (under investigation) Dead Sea products (under investigation)
Dead Sea products (under investigation) Amifostine
Amifostine Pentoxifylline (under investigation)
Pentoxifylline (under investigation) Celecoxib (under investigation)
Celecoxib (under investigation) Amitriptyline, ketamine, and lidocaine gel
Amitriptyline, ketamine, and lidocaine gel



 Avoidance of excessive ionizing radiation exposure
Avoidance of excessive ionizing radiation exposure Emollient creams
Emollient creams Topical corticosteroids
Topical corticosteroids Topical trolamine-containing emulsion
Topical trolamine-containing emulsion Topical calendula
Topical calendula Dexpanthenol
Dexpanthenol Topical silver sulfadiazine
Topical silver sulfadiazine Emollient creams
Emollient creams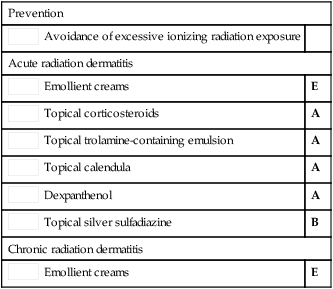
 Skin grafting
Skin grafting