Xanthomas
Lucile E. White, Marcelo G. Horenstein and Christopher R. Shea
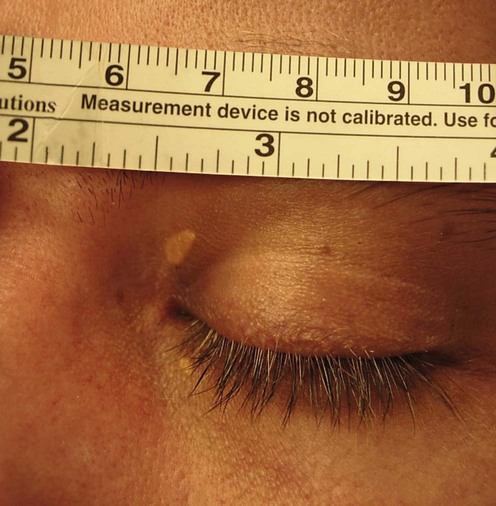
(Courtesy of Arlene Ruiz de Luzuriaga, MD, MPH)
Specific investigations
 Serum lipid panel of cholesterol, triglycerides, VLDL, LDL, and HDL
Serum lipid panel of cholesterol, triglycerides, VLDL, LDL, and HDL
 Gas–liquid and high-performance liquid chromatography to diagnose sitosterolemia
Gas–liquid and high-performance liquid chromatography to diagnose sitosterolemia
 Capillary gas chromatography of urine to diagnose cerebrotendinous xanthomatosis
Capillary gas chromatography of urine to diagnose cerebrotendinous xanthomatosis
 Serum protein electrophoresis, immunoelectrophoresis, or immunofixation to detect M proteins
Serum protein electrophoresis, immunoelectrophoresis, or immunofixation to detect M proteins
First-line therapies
 Low-fat diet and systemic lipid-lowering therapy: statins, bile acid-binding resins, fibrates, and/or nicotinic acid
Low-fat diet and systemic lipid-lowering therapy: statins, bile acid-binding resins, fibrates, and/or nicotinic acidSecond-line therapies
 Surgery
Surgery CO2 laser
CO2 laser Erbium : YAG laser
Erbium : YAG laser Pulsed dye laser
Pulsed dye laser Argon laser
Argon laser Q-switched Nd : YAG laser
Q-switched Nd : YAG laser KTP laser
KTP laser 1450-nm-diode laser
1450-nm-diode laser Low-voltage radiofrequency
Low-voltage radiofrequency
 Di- or trichloracetic acid
Di- or trichloracetic acid Cryotherapy
Cryotherapy Bleomycin
Bleomycin Intralesional triamcinolone acetonide
Intralesional triamcinolone acetonide Chlorambucil
Chlorambucil Prednisolone
Prednisolone Intravenous immunoglobulin
Intravenous immunoglobulin