[level-membership-for-dermatology-category]
Paronychia



First-line therapies
 Amoxicillin with clavulinic acid
Amoxicillin with clavulinic acid Surgical drainage
Surgical drainage Topical corticosteroid preparations
Topical corticosteroid preparations Topical tacrolimus 0.1% ointment
Topical tacrolimus 0.1% ointment Topical clotrimazole drops
Topical clotrimazole drops Topical clindamycin solution
Topical clindamycin solution Avulsion of nail plate
Avulsion of nail plate Mupirocin and clobetasol propionate
Mupirocin and clobetasol propionate Doxycycline
Doxycycline Dose reduction
Dose reduction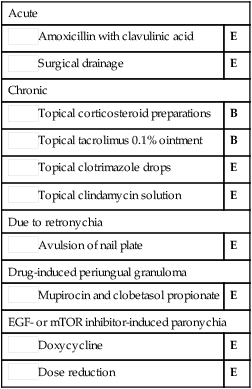
 Nystatin ointment
Nystatin ointment Intralesional or systemic corticosteroids and antibiotics
Intralesional or systemic corticosteroids and antibiotics Leeches
Leeches Eponychial marsupialization
Eponychial marsupialization Excision of nailfold
Excision of nailfold Superficial low-dose radiotherapy
Superficial low-dose radiotherapy[/level-membership-for-dermatology-category][not-level-membership-for-dermatology-category]
Paronychia
[level-membership-for-dermatology-category]
[/level-membership-for-dermatology-category][not-level-membership-for-dermatology-category]
