Published on 18/03/2015 by admin
Filed under Dermatology
Last modified 22/04/2025
This article have been viewed 2354 times
Drore Eisen
Evidence Levels: A Double-blind study B Clinical trial ≥ 20 subjects C Clinical trial < 20 subjects D Series ≥ 5 subjects E Anecdotal case reports
Oral lichen planus (OLP) is a common chronic inflammatory disorder which rarely undergoes complete remission even with treatment.
All treatment should be aimed at eliminating erythematous and ulcerative lesions, alleviating symptoms, and potentially reducing the risk of malignant transformation. Given the uncertainty of the premalignant nature of OLP, it is important to monitor all patients carefully and long term.
Although the etiology of OLP is unknown, the possibility of a hypersensitivity reaction (oral lichenoid reaction, OLR) should be considered when lesions are confined to mucosa in close proximity to a dental restoration. In such cases, identifying allergies to dental materials by patch testing, and then removing the fillings with positive reactions, or empirically removing the filling, often results in resolution of lesions. Another uncommon cause of OLR is drugs. A thorough medication history, with emphasis on NSAIDs, ACE inhibitors, oral hypoglycemics, antimalarials, and others is warranted, as drug-induced reactions are reversible when the implicated drug is withdrawn.
Eliminating exacerbating factors, including sharp dental restorations, fractured teeth, and poorly fitting dental appliances, should be attempted before medical therapy is initiated. An optimal oral hygiene program that eliminates dental plaque and calculus also significantly improves gingival OLP.
All agents used for the treatment of OLP are for off-label indications and lack adequate efficacy studies; thus, optimal dose, duration of treatment, safety, and their true efficacy remain unknown.
The most useful agents for the treatment of symptomatic OLP are potent topical corticosteroids (i.e., fluocinonide or clobetasol). Asymptomatic reticular lesions do not require therapy. For gingival OLP, custom dental trays that cover the teeth are filled with topical corticosteroids and worn for prolonged periods. For intractable erosive lesions, intralesional triamcinolone acetonide (10–20 mg/mL) repeated every 2 to 4 weeks is highly effective.
Unresponsive OLP may benefit from topical immunomodulators (i.e., tacrolimus, pimecrolimus, and cyclosporine) which may be used as alternatives to, or in conjunction with, topical corticosteroids. Burning and stinging are the most frequent adverse effects, and relapses after cessation of therapy are to be expected. Given the potential increased risk of cancer with these immunosuppressants, their long-term use for this chronic, potentially premalignant disease may be limited.
A number of herbal preparations have been reported to benefit OLP. These include purslane (235 mg/day), curcuminoids (6000 mg/day), lycopene (8 mg/day), and topical aloe vera (70% concentration).
A variety of lasers have also been shown to be beneficial in alleviating OLP symptoms.
For patients with severe oral disease or with extraoral manifestations, the addition of systemic immunosuppressives is indicated. The author has found that methotrexate (12.5–20 mg/week), azathioprine (100–150 mg/day), mycophenolate mofetil (1–2 g/day), acitretin (25–50 mg/day), and hydroxychloroquine (400 mg/day) are the most useful systemic agents. Cyclosporine, thalidomide, and TNF-α inhibitors may be used for refractory cases, but data are limited.
Systemic corticosteroids (30–80 mg of prednisone) should be reserved for acute flares and not as maintenance therapy. Secondary candidiasis frequently complicates all therapy and requires treatment with topical or systemic agents. All treatments for OLP are palliative and not curative, and patients should expect a chronic course with intermittent acute exacerbations.
Biopsy for confirmation; direct immunofluorescence when needed to rule out other vesiculoerosive diseases
Monitoring for malignant transformation
Hepatitis serologies when risk factors are present
Consider lichenoid reactions
Raghu AR, Nirmala NR, Sreekumaran N. Quintessence Int 2002; 33: 234–9.
Biopsies of gingival OLP are often non-diagnostic, but immunofluorescence shows characteristic shaggy fibrinogen deposition at the basement membrane zone in both OLP and lichenoid reactions.
Bombeccari GP, Guzzi G, Tettamanti M, Giannì AB, Baj A, Pallotti F, et al. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011; 112: 328–34.
Although the malignant potential of OLP remains controversial, the frequency of malignant change ranges from 0.4% to 3.3%, over periods of observation from 0.5 to over 20 years.
Carbone M, Arduino PG, Carrozzo M, Gandolfo S, Argiolas MR, Bertolusso G, et al. Oral Dis 2009; 15: 235–43.
Routine hepatitis screening in northern European and American OLP patients without risk factors may not be warranted but OLP is significantly associated with hepatitis C infections in southern Europe and Japan.
Pezelj-Ribaric S, Prpic J, Miletic I, Brumini G, Soskic MS, Anic I. J Eur Acad Dermatol Venereol 2008; 22: 1163–7.
When patch test reactions to mercury compounds were positive, partial or complete replacement of amalgam fillings led to a significant improvement in nearly all patients.
Carbone M, Goss E, Carrozzo M, Castellano S, Conrotto D, Broccoletti R, et al. J Oral Pathol Med 2003; 32: 323–9.
Patients treated with topical clobetasol, or prednisone and then clobetasol, responded similarly, suggesting that prednisone should be reserved only for acute exacerbations.
High-potency preparations appear to be more effective than mid-potency ones. Once the disease becomes inactive, therapy may be temporarily discontinued.
Xia J, Li C, Hong Y, Yang L, Huang Y, Cheng B. J Oral Pathol Med 2006; 35: 327–31.
Of the 45 patients treated with intralesional triamcinolone, 85% achieved complete resolution of ulcerations.
Radfar L, Wild RC, Suresh L. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008; 105: 187–93.
In this 6-week, 30-patient study, tacrolimus was shown to be as useful as clobetasol.
Hodgson TA, Sahni N, Kaliakatsou F, Buchanan JA, Porter SR. Eur J Dermatol 2003; 13: 466–70.
Of 50 patients who used tacrolimus for 2 to 39 months, 14% had complete resolution of ulcers, 80% had partial resolution, and 6% reported no benefit.
Gorouhi, F, Solhpour A, Beitollahi JM, Afshar S, Davari P, Hashemi P, et al. J Am Acad Dermatol 2007; 57: 806–13.
In a 20-patient, 2-month study, pimecrolimus was as effective as triamcinolone 0.1%.
McCaughey C, Machan M, Bennett R, Zone JJ, Hull CM. J Eur Acad Dermatol Venereol 2011; 25: 1061–7.
Highly effective when used twice daily for 6 weeks, but blood concentrations were detected in most patients. Relapses occurred in all patients after discontinuing therapy.
Tacrolimus and pimecrolimus are not always effective and do not result in long-term benefits when they are discontinued. Given the potential for systemic absorption and their association with an increased risk of cancer, their safety for long-term use in the oral cavity remains unknown.
Conrotto D, Carbone M, Carrozzo M, Arduino P, Broccoletti R, Pentenero M, et al. Br J Dermatol 2006; 154: 139–45.
In this 2-month study of 40 patients, 65% improved with cyclosporine versus 95% with clobetasol. Two months after discontinuing treatment, one-third of the clobetasol group remained clear, versus three-quarters of the cyclosporine group.
Cyclosporine benefits are inconsistent. The high cost of swishing cyclosporine (500 mg/5 mL three times a day) limits its use, but swishing a smaller quantity or applying a finger rub dose (50 mg/day) has been shown to be beneficial and lowers the cost.
Torti DC, Jorizzo JL, McCarty MA. Arch Dermatol 2007; 143: 511–15.
About 50% treated with low doses of methotrexate (2.5–12.5 mg/week) responded to therapy.
Dalmau J, Puig L, Roe E, Peramiquel L, Campos M, Alomar A. J Eur Acad Dermatol Venereol 2007; 21: 259–60.
Silverman S Jr, Gorsky M, Lozada-Nur F, Giannotti K. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1991; 72: 665–70.
Azathioprine (50–150 mg/day) is effective but requires 3 to 6 months before maximal benefit is achieved.
Eisen D. J Am Acad Dermatol 1993; 28: 609–12.
Nine of 10 patients had an excellent response to hydroxychloroquine 200–400 mg/day for 6 months.
Chao TJ. Cutis 2009; 84: 325–8.
Yarom N. Am J Clin Dermatol 2007; 8: 121.
Won TH, Park SY, Kim BS, Seo PS, Park SD. Ann Dermatol 2009; 21: 250–4.
Levamisole 50 mg three times a day for 3 consecutive days per week was admistered to 11 patients. After 3 months, five patients reported complete improvement.
Systemic agents appear to offer significantly better results than topical medications. None produces long-term remission when discontinued, but significant clinical benefits are achieved and maintained with long-term administration. Topical agents should be administered concomitantly.
Sloberg K, Hersle K, Mobacken H, Thilander H. Arch Dermatol 1979; 115: 716–18.
More than 70% of the 23 patients treated with 0.1% tretinoin improved.
As a monotherapy, topical retinoids have limited value and should be used in combination with topical corticosteroids.
Laurberg G, Geiger JM, Hjorth N, Holm P, Hou-Jensen K, Jacobsen KU, et al. J Am Acad Dermatol 1991; 24: 434–7.
In this 2-month study in 65 patients, some with OLP, acitretin (30 mg/day) resulted in remission or marked improvement in most cases. The majority of patients experienced adverse effects.
Levell NJ, Munro CS, Marks JM. Br J Dermatol 1992; 127: 66–7.
Camisa C, Popovsky JL. Arch Dermatol 2000; 136: 1442–3.
A single report resolving with thalidomide (50–100 mg/day).
Agha-Hosseini F, Borhan-Mojabi K, Monsef-Esfahani HR, Mirzaii-Dizgah I, Etemad-Moghadam S, Karagah A. Phytother Res 2010; 24: 240–4.
In this double-blind placebo study of 37 patients, 83% receiving purslane (235 mg/day) showed partial to complete improvement.
Purslane is consumed worldwide, is highly nutritive and contains significant levels of omega-3 fatty acids.
Chainani-Wu N, Madden E, Lozada-Nur F, Silverman S Jr. J Am Acad Dermatol 2012; 66(5): 752–60.
Twenty patients in this double-blind placebo used curcuminoids (6000 mg/day) which produced modest benefits.
Saawarn N, Shashikanth MC, Saawarn S, Jirge V, Chaitanya NC, Pinakapani R. Indian J Dent Res 2011; 22: 639–43.
In 15 patients, lycopene (8 mg/day) was administerd for 6 weeks, and 73% of patients showed 70–100% benefit.
Salazar-Sanchez N, Lopez-Jornet P, Camacho-Alonso F, Sanchez-Siles M. J Oral Pathol Med 2010; 39: 735–40.
In 32 patients, a 70% concentration of aloe vera administered three times a day for 12 weeks resulted in most patients improving.
Cafaro A, Albanese G, Arduino PG, Mario C, Massolini G, Mozzati M. et al. Photomed Laser Surg 2010; 28(Suppl 2): S99–S103.
Fornaini C, Raybaud H, Augros C, Rocca JP. Photomed Laser Surg 2012; 30: 234–8.
Jajarm HH, Falaki F, Mahdavi O. Photomed Laser Surg 2011; 29: 421–5.
In a trial of 30 patients, the 630 nm diode laser versus dexamethasone wash was studied; both were effective with equal response rates.
Laser therapy is an emerging treatment for OLP that appears to be well tolerated, painless, with few or no postoperative complications.
Treatment of Skin Disease Comprehensive Therapeutic Strategies 4e
WhatsApp us





 Topical corticosteroids
Topical corticosteroids Intralesional corticosteroids
Intralesional corticosteroids Tacrolimus
Tacrolimus Pimecrolimus
Pimecrolimus Cyclosporine
Cyclosporine Methotrexate
Methotrexate Mycophenolate mofetil
Mycophenolate mofetil Azathioprine
Azathioprine Hydroxychloroquine sulfate
Hydroxychloroquine sulfate TNF-α inhibitors (adalimumab, etanercept)
TNF-α inhibitors (adalimumab, etanercept) Levamisole
Levamisole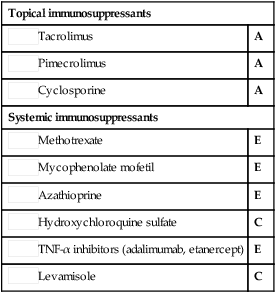

 Topical and systemic retinoids
Topical and systemic retinoids Systemic cyclosporine
Systemic cyclosporine Thalidomide
Thalidomide Purslane
Purslane Curcuminoids
Curcuminoids Lycopene
Lycopene Aloe vera gel
Aloe vera gel Laser
Laser