Morphea

Management strategy
Initial evaluation
The initial evaluation of patients with morphea should involve:
 Questions regarding recent development of new lesions/extension of existing lesions to determine level of activity
Questions regarding recent development of new lesions/extension of existing lesions to determine level of activity


 Palpation of affected areas for depth of sclerosis
Palpation of affected areas for depth of sclerosis



 Imaging with MRI if musculoskeletal involvement is suspected.
Imaging with MRI if musculoskeletal involvement is suspected.
Active morphea lesions should be treated as the lesions are frequently symptomatic and can produce permanent cosmetic and functional sequelae. Initial evaluation should be focused on determining the extent, severity, and activity of morphea lesions laying the groundwork for rational therapeutic choices.
Specific investigations





First-line therapies
 Phototherapy: BB-UVA, NB-UVB, UVA1
Phototherapy: BB-UVA, NB-UVB, UVA1 Methotrexate + IV corticosteroids (PCMT)
Methotrexate + IV corticosteroids (PCMT) Methotrexate + oral steroids
Methotrexate + oral steroids Calciprotriene under occlusion
Calciprotriene under occlusion Topical tacrolimus (occluded)
Topical tacrolimus (occluded) Intralesional steroids
Intralesional steroids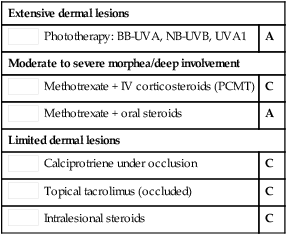
Second-line therapies
 PUVA (bath or cream)
PUVA (bath or cream) Mycophenolate mofetil
Mycophenolate mofetil Abatacept
Abatacept Imiquimod
Imiquimod Calciprotriol–betamethasone
Calciprotriol–betamethasone
 Cyclosporine
Cyclosporine Combination of oral medications
Combination of oral medications Combination of oral medications with light
Combination of oral medications with light








