[level-membership-for-basic-science-category]
Chapter 16 Hematology
Heparins





MOA (Mechanism of Action)
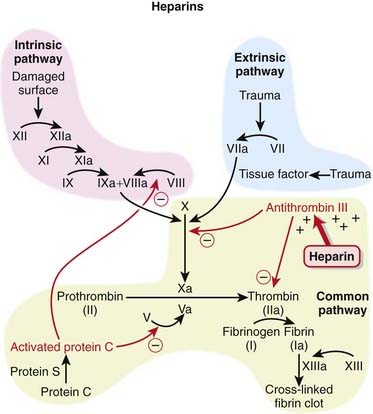
 The coagulation (clotting) system is composed of many proteins. Most of these proteins are procoagulants, which means they contribute to clotting. Some proteins are anticoagulants that serve to keep the coagulation system in balance.
The coagulation (clotting) system is composed of many proteins. Most of these proteins are procoagulants, which means they contribute to clotting. Some proteins are anticoagulants that serve to keep the coagulation system in balance. When a protein is activated, its name is followed by a small letter a. Each activated protein serves as an enzyme for the next protein downstream in the cascade (Figure 16-1).
When a protein is activated, its name is followed by a small letter a. Each activated protein serves as an enzyme for the next protein downstream in the cascade (Figure 16-1).




Pharmacokinetics
Unfractionated Heparin
 Very complex pharmacokinetics exist because there is a large range in molecular weight of the molecules
Very complex pharmacokinetics exist because there is a large range in molecular weight of the molecules











Indications
 Treatment and prevention of inappropriate thrombosis
Treatment and prevention of inappropriate thrombosis

















Important Notes
 To measure the effect of UFH, the aPTT test is used (compare this with prothrombin time [PT] or International Normalized Ratio [INR], which is used with warfarin). It is a measure of time to coagulation (in the laboratory) and is measured in seconds. The higher the number, the more strongly a patient is anticoagulated.
To measure the effect of UFH, the aPTT test is used (compare this with prothrombin time [PT] or International Normalized Ratio [INR], which is used with warfarin). It is a measure of time to coagulation (in the laboratory) and is measured in seconds. The higher the number, the more strongly a patient is anticoagulated.




Evidence

LMWH versus Warfarin for Treatment of Venous Thromboembolism
 A 2001 Cochrane review (seven studies, N = 1137 participants), updated in 2003, compared warfarin with LMWH for long-term treatment of VTE. There was no difference in the risk of recurrent VTE between warfarin and LMWH. There was a lower risk of bleeding with LMWH (odds ratio [OR] 0.38), and no difference in mortality rates between these two interventions was found.
A 2001 Cochrane review (seven studies, N = 1137 participants), updated in 2003, compared warfarin with LMWH for long-term treatment of VTE. There was no difference in the risk of recurrent VTE between warfarin and LMWH. There was a lower risk of bleeding with LMWH (odds ratio [OR] 0.38), and no difference in mortality rates between these two interventions was found.LMWH and Heparinoids versus UFH for Ischemic Stroke
 A 2008 Cochrane review (nine studies, N = 3137 patients) compared LMWH and heparinoids (danaparoid) with UFH in patients with acute, presumed or confirmed ischemic stroke. The odds of developing a deep vein thrombosis (DVT) were reduced with LMWH compared with UFH (OR 0.55); however, the incidence of key clinical outcomes such as PE, death, and hemorrhage (intracranial or extracranial) was too small to provide a reliable comparison.
A 2008 Cochrane review (nine studies, N = 3137 patients) compared LMWH and heparinoids (danaparoid) with UFH in patients with acute, presumed or confirmed ischemic stroke. The odds of developing a deep vein thrombosis (DVT) were reduced with LMWH compared with UFH (OR 0.55); however, the incidence of key clinical outcomes such as PE, death, and hemorrhage (intracranial or extracranial) was too small to provide a reliable comparison.


Direct Factor Xa Inhibitors

MOA (Mechanism of Action)
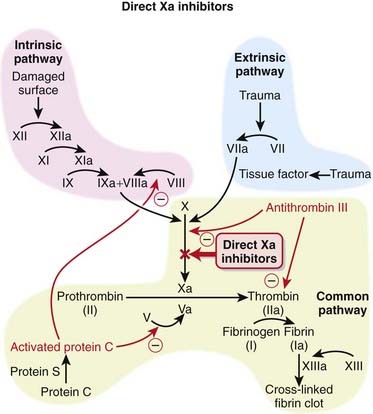
 The coagulation system is composed of many proteins: most of these proteins are procoagulants, which means they contribute to clotting. Some proteins are anticoagulants, which serve to keep the coagulation system in balance.
The coagulation system is composed of many proteins: most of these proteins are procoagulants, which means they contribute to clotting. Some proteins are anticoagulants, which serve to keep the coagulation system in balance.





Pharmacokinetics








Important Notes
 There are no monitoring requirements for rivaroxaban. This and the fact that it is an orally administered agent suggest that drugs in its class, and perhaps the direct thrombin inhibitors, will supplant warfarin as the drugs of choice among oral anticoagulants.
There are no monitoring requirements for rivaroxaban. This and the fact that it is an orally administered agent suggest that drugs in its class, and perhaps the direct thrombin inhibitors, will supplant warfarin as the drugs of choice among oral anticoagulants.Advanced
Drug Interactions
 CYP450 3A4 enzymes are involved in the metabolism of rivaroxaban; thus the potential exists for pharmacokinetic drug interactions with inhibitors or inducers of this isozyme. Rivaroxaban is also a P-glycoprotein (Pgp) substrate, and therefore its levels could also be affected by inhibitors or inducers of Pgp.
CYP450 3A4 enzymes are involved in the metabolism of rivaroxaban; thus the potential exists for pharmacokinetic drug interactions with inhibitors or inducers of this isozyme. Rivaroxaban is also a P-glycoprotein (Pgp) substrate, and therefore its levels could also be affected by inhibitors or inducers of Pgp.Evidence
Postsurgical Venous Thromboembolism Prophylaxis
 The RECORD trials were a series of double-blind randomized controlled trials that compared rivaroxaban with enoxaparin for the prophylactic treatment of VTE after total hip replacement (RECORD-1 and RECORD-2) or total knee replacement (RECORD-3 and RECORD-4). The trials were all relatively large, randomizing 2509 to 4541 patients between the two treatment groups. Rivaroxaban-treated patients had fewer events of VTE and all-cause deaths compared with enoxaparin in each of the four studies. The risk of bleeding was slightly higher with rivaroxaban than with enoxaparin.
The RECORD trials were a series of double-blind randomized controlled trials that compared rivaroxaban with enoxaparin for the prophylactic treatment of VTE after total hip replacement (RECORD-1 and RECORD-2) or total knee replacement (RECORD-3 and RECORD-4). The trials were all relatively large, randomizing 2509 to 4541 patients between the two treatment groups. Rivaroxaban-treated patients had fewer events of VTE and all-cause deaths compared with enoxaparin in each of the four studies. The risk of bleeding was slightly higher with rivaroxaban than with enoxaparin.FYI
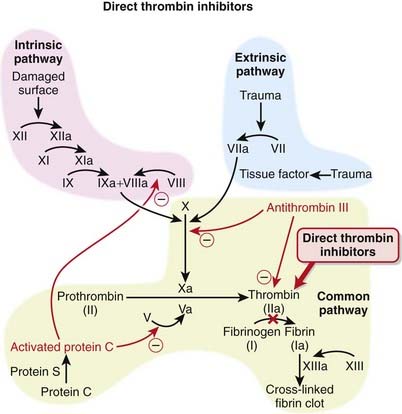
 For a quick summary of the difference between two of the newer oral anticoagulants—direct factor Xa and direct thrombin inhibitors. Direct factor Xa inhibitors inhibit the formation of thrombin, whereas direct thrombin inhibitors allow thrombin to be formed but interfere with the actions of thrombin.
For a quick summary of the difference between two of the newer oral anticoagulants—direct factor Xa and direct thrombin inhibitors. Direct factor Xa inhibitors inhibit the formation of thrombin, whereas direct thrombin inhibitors allow thrombin to be formed but interfere with the actions of thrombin.Direct Thrombin Inhibitors




MOA (Mechanism of Action)
 The coagulation (clotting) system is a multistep cascade that eventually leads to the formation of fibrin and development of a clot.
The coagulation (clotting) system is a multistep cascade that eventually leads to the formation of fibrin and development of a clot.


















Important Notes
 All of the agents in this class are approved for prophylaxis of DVT and VTE after orthopedic surgery. Patients undergoing knee or hip replacement surgeries, in particular, are at high risk for developing a DVT or VTE. The risk is so high that these patients receive prophylactic anticoagulants for several days postsurgery.
All of the agents in this class are approved for prophylaxis of DVT and VTE after orthopedic surgery. Patients undergoing knee or hip replacement surgeries, in particular, are at high risk for developing a DVT or VTE. The risk is so high that these patients receive prophylactic anticoagulants for several days postsurgery.




Vitamin K Antagonists

MOA (Mechanism of Action)









Indications














Important Notes
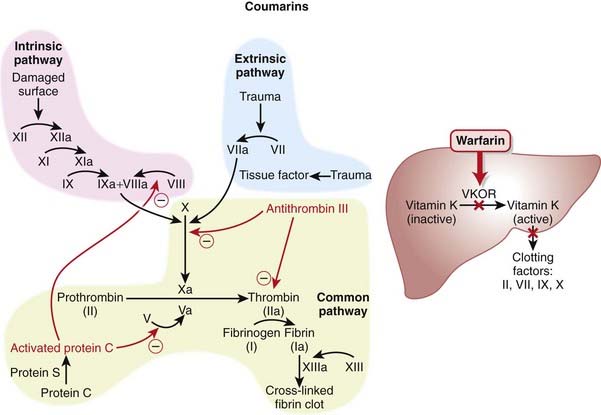
 Warfarin therapy is monitored using the International Normalized Ratio (INR), which is a standardized form of the PT test. Because different laboratories use different reagents to test the PT, every laboratory generates a slightly different result, so the INR corrects for this discrepancy among laboratories.
Warfarin therapy is monitored using the International Normalized Ratio (INR), which is a standardized form of the PT test. Because different laboratories use different reagents to test the PT, every laboratory generates a slightly different result, so the INR corrects for this discrepancy among laboratories.







Evidence
Warfarin versus LMWH for Treatment of Venous Thromboembolism
 A 2001 Cochrane review (seven studies, N = 1137 participants), updated in 2003, compared warfarin with LMWHs for long-term treatment of VTE. There was no difference in the risk of recurrent VTE between warfarin and LMWH. There was a lower risk of bleeding with LMWH (OR 0.38), and no difference in mortality rates between these two interventions.
A 2001 Cochrane review (seven studies, N = 1137 participants), updated in 2003, compared warfarin with LMWHs for long-term treatment of VTE. There was no difference in the risk of recurrent VTE between warfarin and LMWH. There was a lower risk of bleeding with LMWH (OR 0.38), and no difference in mortality rates between these two interventions.Warfarin versus Acetylsalicylic Acid for Atrial Fibrillation
 A 2007 Cochrane review (eight studies, N = 9598 participants) compared warfarin with acetylsalicylic acid (ASA) in atrial fibrillation patients who had not had a prior stroke or transient ischemic attack (TIA). Treatment with warfarin led to a lower risk of stroke (OR 0.68), ischemic stroke (OR 0.53), and systemic emboli (OR 0.48). The risk of intracranial hemorrhage was increased with warfarin (OR 1.98). All-cause mortality and vascular deaths were similar between groups, and disabling or fatal strokes and MI were almost reduced with oral anticoagulants, but this did not reach statistical significance.
A 2007 Cochrane review (eight studies, N = 9598 participants) compared warfarin with acetylsalicylic acid (ASA) in atrial fibrillation patients who had not had a prior stroke or transient ischemic attack (TIA). Treatment with warfarin led to a lower risk of stroke (OR 0.68), ischemic stroke (OR 0.53), and systemic emboli (OR 0.48). The risk of intracranial hemorrhage was increased with warfarin (OR 1.98). All-cause mortality and vascular deaths were similar between groups, and disabling or fatal strokes and MI were almost reduced with oral anticoagulants, but this did not reach statistical significance.

Salicylates





MOA (Mechanism of Action)
Salicylates
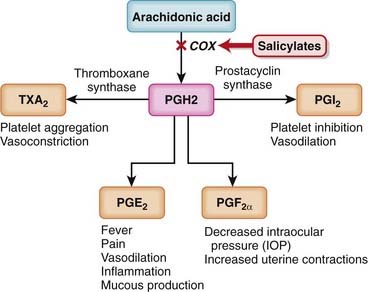
 Like nonsteroidal antiinflammatory drugs (NSAIDs), the salicylates work by inhibiting the actions of the cyclooxygenase (COX) enzyme (Figure 16-5).
Like nonsteroidal antiinflammatory drugs (NSAIDs), the salicylates work by inhibiting the actions of the cyclooxygenase (COX) enzyme (Figure 16-5).





Pharmacokinetics
Salicylates














Side Effects






Important Notes
 Because the binding of ASA to the platelets is irreversible, the antiplatelet effect of ASA lasts for the lifespan of the platelet, which is about 5 to 7 days. Patients preparing for surgery must stop taking ASA 7 days before surgery.
Because the binding of ASA to the platelets is irreversible, the antiplatelet effect of ASA lasts for the lifespan of the platelet, which is about 5 to 7 days. Patients preparing for surgery must stop taking ASA 7 days before surgery.

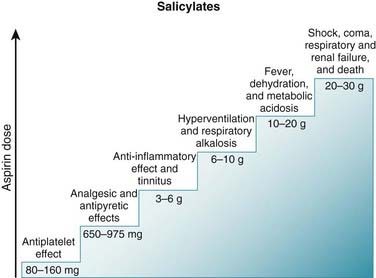
 Salicylate poisoning can therefore lead to severe acid-base disturbances. Stimulation of respiration leads to a respiratory alkalosis, which is compensated for by the kidneys (Figure 16-7).
Salicylate poisoning can therefore lead to severe acid-base disturbances. Stimulation of respiration leads to a respiratory alkalosis, which is compensated for by the kidneys (Figure 16-7).


Advanced
 Salicylates are rapidly absorbed after oral administration. Despite the fact that salicylates are acids, and are therefore ionized in an alkaline environment, raising the pH of the stomach will enhance dissolution, and the net effect will be to enhance absorption. Therefore buffered preparations confer minimal advantage when it comes to rapid absorption.
Salicylates are rapidly absorbed after oral administration. Despite the fact that salicylates are acids, and are therefore ionized in an alkaline environment, raising the pH of the stomach will enhance dissolution, and the net effect will be to enhance absorption. Therefore buffered preparations confer minimal advantage when it comes to rapid absorption.Evidence
Aspirin Alone or in Combination with Clopidogrel for Prevention of Cardiovascular Events
 A 2007 Cochrane review (two studies, N = 28,165 patients) compared the combination of clopidogrel and aspirin with aspirin alone for preventing cardiovascular events in patients at high risk for cardiovascular disease and those with established cardiovascular disease. The authors included two large trials. CHARISMA patients were at high risk for cardiovascular events, with or without established cardiovascular disease, whereas patients in CURE had had a recent non–ST-segment elevation acute coronary syndrome. In CHARISMA the benefit of combination therapy was minimal: five cardiovascular events avoided and three major bleeds for every 1000 patients over 28 months. In CURE the benefits were more obvious, with 23 events avoided and 10 major bleeds over 9 months.
A 2007 Cochrane review (two studies, N = 28,165 patients) compared the combination of clopidogrel and aspirin with aspirin alone for preventing cardiovascular events in patients at high risk for cardiovascular disease and those with established cardiovascular disease. The authors included two large trials. CHARISMA patients were at high risk for cardiovascular events, with or without established cardiovascular disease, whereas patients in CURE had had a recent non–ST-segment elevation acute coronary syndrome. In CHARISMA the benefit of combination therapy was minimal: five cardiovascular events avoided and three major bleeds for every 1000 patients over 28 months. In CURE the benefits were more obvious, with 23 events avoided and 10 major bleeds over 9 months.Single-Dose Aspirin versus Placebo for Acute Pain
 A 1999 Cochrane review (72 trials, N = 3253 participants) compared a single dose of aspirin with placebo for acute pain of moderate to severe intensity. The number needed to treat (NNT) for at least 50% pain relief was 4.4 for 600- to 650-mg doses, 4.0 for a 1000-mg dose, and 2.4 for a 1200-mg dose. A single dose of aspirin produced more drowsiness (number needed to harm [NNH] 28) and gastric irritation (NNH 38) than placebo.
A 1999 Cochrane review (72 trials, N = 3253 participants) compared a single dose of aspirin with placebo for acute pain of moderate to severe intensity. The number needed to treat (NNT) for at least 50% pain relief was 4.4 for 600- to 650-mg doses, 4.0 for a 1000-mg dose, and 2.4 for a 1200-mg dose. A single dose of aspirin produced more drowsiness (number needed to harm [NNH] 28) and gastric irritation (NNH 38) than placebo.Aspirin for Prevention or Regression of Sporadic Colorectal Adenomas
 A 2004 Cochrane review (nine trials, N = 24,143 participants) examined the use of NSAIDs and aspirin for the prevention or regression of sporadic colorectal adenomas and colorectal cancer. Fewer patients treated with low-dose ASA developed recurrent sporadic colorectal adenomas after 1 to 3 years (NNT 12.5) compared with controls, and these results were driven by one large placebo-controlled study. There was no significant difference in the outcomes for colorectal cancer or for adverse events in any trials.
A 2004 Cochrane review (nine trials, N = 24,143 participants) examined the use of NSAIDs and aspirin for the prevention or regression of sporadic colorectal adenomas and colorectal cancer. Fewer patients treated with low-dose ASA developed recurrent sporadic colorectal adenomas after 1 to 3 years (NNT 12.5) compared with controls, and these results were driven by one large placebo-controlled study. There was no significant difference in the outcomes for colorectal cancer or for adverse events in any trials.Aspirin versus Other Antiplatelets for Preventing Serious Vascular Events in High-Risk Patients
 A 2000 Cochrane review (four trials, N = 22,656 patients) compared the thienopyridines ticlopidine and clopidogrel with aspirin for the prevention of serious vascular events in high-risk patients, particularly those who had had previous TIA or ischemic stroke. Thienopyridines reduced the risk of a serious vascular event compared with aspirin, avoiding 11 events per 1000 patients over 2 years (OR 0.91). Thienopyridines also reduced the risk of stroke by seven events per 1000 patients over 2 years. This reduction in risk increased to 16 events per 1000 patients in individuals with a history of TIA or ischemic stroke. The thienopyridines reduced the risk of GI hemorrhage but increased the risk of skin rash and diarrhea versus aspirin. Ticlopidine also significantly increased the risk of neutropenia.
A 2000 Cochrane review (four trials, N = 22,656 patients) compared the thienopyridines ticlopidine and clopidogrel with aspirin for the prevention of serious vascular events in high-risk patients, particularly those who had had previous TIA or ischemic stroke. Thienopyridines reduced the risk of a serious vascular event compared with aspirin, avoiding 11 events per 1000 patients over 2 years (OR 0.91). Thienopyridines also reduced the risk of stroke by seven events per 1000 patients over 2 years. This reduction in risk increased to 16 events per 1000 patients in individuals with a history of TIA or ischemic stroke. The thienopyridines reduced the risk of GI hemorrhage but increased the risk of skin rash and diarrhea versus aspirin. Ticlopidine also significantly increased the risk of neutropenia.Maintenance of Remission in Ulcerative Colitis
 A 2006 Cochrane review (16 studies, N = 2479) assessed the newer release formulations of 5-ASA versus placebo or sulfasalazine in the maintenance of remission in ulcerative colitis. Compared with placebo, the NNT for failure to maintain clinical or endoscopic remission was six. However, newer formulations of 5-ASA were less effective than sulfasalazine (OR 1.29). Although the incidence of side effects was similar with 5-ASA and with sulfasalazine, the authors noted that sulfasalazine trials enrolled patients who were already tolerating sulfasalazine, perhaps biasing the comparison of side effects in favor of sulfasalazine.
A 2006 Cochrane review (16 studies, N = 2479) assessed the newer release formulations of 5-ASA versus placebo or sulfasalazine in the maintenance of remission in ulcerative colitis. Compared with placebo, the NNT for failure to maintain clinical or endoscopic remission was six. However, newer formulations of 5-ASA were less effective than sulfasalazine (OR 1.29). Although the incidence of side effects was similar with 5-ASA and with sulfasalazine, the authors noted that sulfasalazine trials enrolled patients who were already tolerating sulfasalazine, perhaps biasing the comparison of side effects in favor of sulfasalazine.FYI
 ASA originated from salicylic acid, derived from the bark of the willow tree. The use of salicylic acid dates back to ancient times, both in North America and in Europe, and its first official medical use was ascribed to Hippocrates. Chemists began synthesizing salicylic acid in the later nineteenth century. Salicylic acid had some significant GI side effects, and it was these side effects that led Hoffman, a chemist at Bayer, to acetylate the molecule and create what is still perhaps the most successful nonantibiotic in the history of pharmaceutical development.
ASA originated from salicylic acid, derived from the bark of the willow tree. The use of salicylic acid dates back to ancient times, both in North America and in Europe, and its first official medical use was ascribed to Hippocrates. Chemists began synthesizing salicylic acid in the later nineteenth century. Salicylic acid had some significant GI side effects, and it was these side effects that led Hoffman, a chemist at Bayer, to acetylate the molecule and create what is still perhaps the most successful nonantibiotic in the history of pharmaceutical development.


Adenosine Diphosphate (ADP) Blockers


MOA (Mechanism of Action)
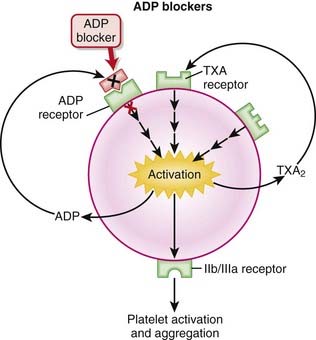
 Platelets are activated by adhering to damaged endothelium by linking of glycoprotein Ia (GPIa) receptors with collagen and GPIb receptors with von Willebrand factor (vWF). The activation of platelets leads to aggregation and clot formation.
Platelets are activated by adhering to damaged endothelium by linking of glycoprotein Ia (GPIa) receptors with collagen and GPIb receptors with von Willebrand factor (vWF). The activation of platelets leads to aggregation and clot formation.





Pharmacokinetics












Important Notes
 There is a significant range of responses to clopidogrel among patients. The extent of platelet inhibition can range from 5% to 90%, with patients at the lower end of the range (<10%) deemed to be “clopidogrel unresponsive.” Genetic polymorphisms are thought to play a role in these variable responses, including alterations in the PGY12 receptor as well as CYP450 mutations.
There is a significant range of responses to clopidogrel among patients. The extent of platelet inhibition can range from 5% to 90%, with patients at the lower end of the range (<10%) deemed to be “clopidogrel unresponsive.” Genetic polymorphisms are thought to play a role in these variable responses, including alterations in the PGY12 receptor as well as CYP450 mutations.
Advanced
 TTP is a life-threatening disease caused by abnormal activation and aggregation of platelets because of vWF macromolecules. The platelets aggregate in vessels and form pathologic thrombi, resulting in hemolysis (and anemia), a decreased platelet count (from consumption), central nervous system (CNS) dysfunction or stroke, and renal compromise because of vascular occlusion and fever. These five findings comprise the pentad of TTP.
TTP is a life-threatening disease caused by abnormal activation and aggregation of platelets because of vWF macromolecules. The platelets aggregate in vessels and form pathologic thrombi, resulting in hemolysis (and anemia), a decreased platelet count (from consumption), central nervous system (CNS) dysfunction or stroke, and renal compromise because of vascular occlusion and fever. These five findings comprise the pentad of TTP.Evidence
Adenosine Diphosphate Blockers versus Aspirin for Stroke Prevention in High-Risk Patients
 A 2000 Cochrane review (four trials, N = 22,656 patients) compared ADP inhibitors with aspirin for preventing serious vascular events in high-risk patients, including those who had had a prior TIA or ischemic stroke. One large trial (N = 19,185 patients) included clopidogrel, whereas the other three (N = 3471) included ticlopidine. Results suggested that ADP blockers would result in 11 fewer serious vascular events per 1000 patients treated over approximately 2 years. Strokes were also reduced, by seven events per 1000 patients.
A 2000 Cochrane review (four trials, N = 22,656 patients) compared ADP inhibitors with aspirin for preventing serious vascular events in high-risk patients, including those who had had a prior TIA or ischemic stroke. One large trial (N = 19,185 patients) included clopidogrel, whereas the other three (N = 3471) included ticlopidine. Results suggested that ADP blockers would result in 11 fewer serious vascular events per 1000 patients treated over approximately 2 years. Strokes were also reduced, by seven events per 1000 patients.
Clopidogrel with or without Aspirin for Preventing Cardiovascular Disease
 A 2007 Cochrane review included two large studies (CHARISMA and CURE, N = 28,165 patients). CHARISMA patients were at high risk for cardiovascular disease but did not necessarily have established cardiovascular disease, whereas patients in CURE had had a recent non–ST-segment elevation acute coronary syndrome. The combination of clopidogrel and aspirin reduced the risk of cardiovascular events by 13 events for every 1000 patients treated; however, six major bleeds would be caused over the same number of patients.
A 2007 Cochrane review included two large studies (CHARISMA and CURE, N = 28,165 patients). CHARISMA patients were at high risk for cardiovascular disease but did not necessarily have established cardiovascular disease, whereas patients in CURE had had a recent non–ST-segment elevation acute coronary syndrome. The combination of clopidogrel and aspirin reduced the risk of cardiovascular events by 13 events for every 1000 patients treated; however, six major bleeds would be caused over the same number of patients.

Antiplatelet IIb/IIIa Inhibitors
Description
Antiplatelet IIb/IIIa inhibitors are antiplatelet drugs; they inhibit platelet function.


MOA (Mechanism of Action)
 IIb/IIIa receptors are located on the outside of platelets, in very high numbers (50,000 to 80,000 per cell); in the resting platelet they are inactive.
IIb/IIIa receptors are located on the outside of platelets, in very high numbers (50,000 to 80,000 per cell); in the resting platelet they are inactive.





















Evidence
Coronary Angioplasty
 A meta-analysis in 2007 (38 trials, N = 58,495 patients) demonstrated that with angioplasty compared with placebo, IIb/IIIa blockers decreased mortality at 30 days (OR 0.74) but not at 6 months. Death or MI was decreased both at 30 days (OR 0.67) and at 6 months (OR 0.71), although severe bleeding was increased (OR 1.38; absolute risk increase 8.6 per 1000).
A meta-analysis in 2007 (38 trials, N = 58,495 patients) demonstrated that with angioplasty compared with placebo, IIb/IIIa blockers decreased mortality at 30 days (OR 0.74) but not at 6 months. Death or MI was decreased both at 30 days (OR 0.67) and at 6 months (OR 0.71), although severe bleeding was increased (OR 1.38; absolute risk increase 8.6 per 1000).


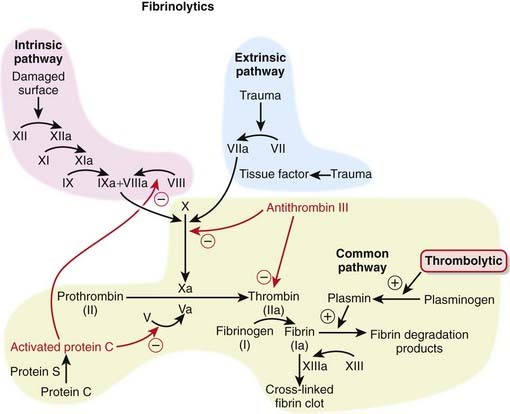
Fibrinolytics
Description
Fibrinolytics lyse (break up) blood clots. They are also called clot busters and thrombolytics.






















Side Effects


Important Notes
 There are advantages and disadvantages to using streptokinase versus rt-PA. rt-PA is more clot selective than urokinase or streptokinase, as it does a poor job of activating plasminogen in the absence of fibrin. However streptokinase is much cheaper than rt-PA. Streptokinase also elicits an immune response that can harm the patient.
There are advantages and disadvantages to using streptokinase versus rt-PA. rt-PA is more clot selective than urokinase or streptokinase, as it does a poor job of activating plasminogen in the absence of fibrin. However streptokinase is much cheaper than rt-PA. Streptokinase also elicits an immune response that can harm the patient.



Evidence
Thrombolytics versus Heparin or Placebo for Treatment of Acute Pulmonary Embolism
 A 2009 Cochrane review (eight trials, N = 679 participants) compared thrombolytics with placebo or heparin in patients with acute PE. The rates of mortality, PE recurrence, major hemorrhagic events, and minor hemorrhagic events were similar between thrombolytics and heparin. In one study that examined combination therapy, the use of rt-PA combined with heparin versus heparin alone reduced the need for further treatment for in-hospital events (OR 0.35).
A 2009 Cochrane review (eight trials, N = 679 participants) compared thrombolytics with placebo or heparin in patients with acute PE. The rates of mortality, PE recurrence, major hemorrhagic events, and minor hemorrhagic events were similar between thrombolytics and heparin. In one study that examined combination therapy, the use of rt-PA combined with heparin versus heparin alone reduced the need for further treatment for in-hospital events (OR 0.35).Thrombolytics for Treatment of Ischemic Stroke
 A 2009 Cochrane review (26 trials, N = 7152 participants) compared thrombolytics with controls in patients with definite ischemic stroke. Although thrombolytics reduced the proportion of patients who were dead or dependent at 3 to 6 months after stroke (OR 0.81), they increased the risk of symptomatic intracranial hemorrhage (OR 3.49) and death by 3 to 6 months after stroke (OR 1.31).
A 2009 Cochrane review (26 trials, N = 7152 participants) compared thrombolytics with controls in patients with definite ischemic stroke. Although thrombolytics reduced the proportion of patients who were dead or dependent at 3 to 6 months after stroke (OR 0.81), they increased the risk of symptomatic intracranial hemorrhage (OR 3.49) and death by 3 to 6 months after stroke (OR 1.31).Thrombolytics versus Angioplasty in Myocardial Infarction
 A 2003 systematic review (23 trials, N = 7739 participants) compared percutaneous transluminal coronary angioplasty (PTCA) with thrombolytics for acute STEMI. There were fewer overall deaths in the short term with PTCA compared with thrombolytics (incidence of 7% versus 9%, respectively), and also a lower incidence of nonfatal reinfarction (3% versus 7%) and stroke (1% versus 2%) with PTCA versus thrombolytics. The results for PTCA continued to be better than thrombolytics during long-term follow-up.
A 2003 systematic review (23 trials, N = 7739 participants) compared percutaneous transluminal coronary angioplasty (PTCA) with thrombolytics for acute STEMI. There were fewer overall deaths in the short term with PTCA compared with thrombolytics (incidence of 7% versus 9%, respectively), and also a lower incidence of nonfatal reinfarction (3% versus 7%) and stroke (1% versus 2%) with PTCA versus thrombolytics. The results for PTCA continued to be better than thrombolytics during long-term follow-up.




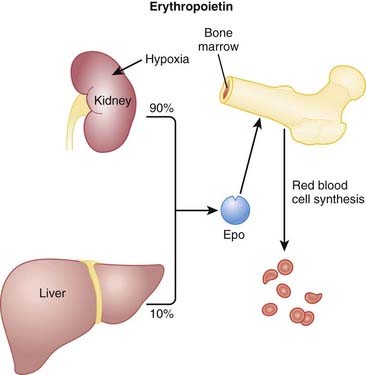
Erythropoietins


MOA (Mechanism of Action)



Pharmacokinetics






Side Effects




Important Notes



Evidence
Recombinant Human Erythropoietin in Predialysis Patients with Anemia
 A 2005 Cochrane review (15 trials, N = 461 participants) compared the use of rHuEPO with no treatment or placebo in predialysis patients with renal anemia. rHuEPO significantly improved hemoglobin and hematocrit and significantly reduced the number of patients requiring blood transfusions (relative risk [RR] 0.32). Quality of life and exercise capacity were also improved, where reported. rHuEPO did not appear to have an effect on the progression of renal disease, and there was no increase in the incidence of adverse events with rHuEPO therapy.
A 2005 Cochrane review (15 trials, N = 461 participants) compared the use of rHuEPO with no treatment or placebo in predialysis patients with renal anemia. rHuEPO significantly improved hemoglobin and hematocrit and significantly reduced the number of patients requiring blood transfusions (relative risk [RR] 0.32). Quality of life and exercise capacity were also improved, where reported. rHuEPO did not appear to have an effect on the progression of renal disease, and there was no increase in the incidence of adverse events with rHuEPO therapy.Recombinant Human Erythropoietin in Preventing Transfusion in Premature Infants
 A 2006 Cochrane review (19 studies, N = 912 infants) compared rHuEPO with placebo or no treatment in reducing the use of RBC transfusions in preterm and/or low–birth-weight infants. The authors found that rHuEPO reduced the risk of having one or more transfusions (typical RR 0.66 [0.59 to 0.74]). rHuEPO also reduced the average volume of blood transfused per infant by 7 mL and the average number of transfusions per infant; however, the clinical significance of these small differences was questioned by the authors. Several hard outcomes such as mortality, hypertension, and numerous other complications were not affected by therapy.
A 2006 Cochrane review (19 studies, N = 912 infants) compared rHuEPO with placebo or no treatment in reducing the use of RBC transfusions in preterm and/or low–birth-weight infants. The authors found that rHuEPO reduced the risk of having one or more transfusions (typical RR 0.66 [0.59 to 0.74]). rHuEPO also reduced the average volume of blood transfused per infant by 7 mL and the average number of transfusions per infant; however, the clinical significance of these small differences was questioned by the authors. Several hard outcomes such as mortality, hypertension, and numerous other complications were not affected by therapy.Darbepoetin or Epoetin in Anemia Associated with Cancer Treatment
 A 2006 Cochrane review (57 trials, N = 9353 participants) assessed darbepoetin and epoetin in the prevention or treatment of anemia in cancer patients. Both agents reduced the risk of transfusions (RR 0.64 [0.60 to 0.68]) and resulted in a requirement for an average of one less unit of blood. However, the risk of thromboembolic events was increased (RR 1.67 [1.35 to 2.06]). The authors were not able to conclude whether these agents have an impact on tumor response or overall survival.
A 2006 Cochrane review (57 trials, N = 9353 participants) assessed darbepoetin and epoetin in the prevention or treatment of anemia in cancer patients. Both agents reduced the risk of transfusions (RR 0.64 [0.60 to 0.68]) and resulted in a requirement for an average of one less unit of blood. However, the risk of thromboembolic events was increased (RR 1.67 [1.35 to 2.06]). The authors were not able to conclude whether these agents have an impact on tumor response or overall survival.FYI
 The chemical structure of epoetin alfa differs slightly from that of human endogenous erythropoietin. Although this difference does not have any clinical relevance, it has proven useful in trying to detect athletes who have been using epoetin alfa for blood doping. This is a practice by which athletes will try to stimulate an artificial increase in hematocrit before a competition to increase the oxygen-carrying capacity of their blood, presumably enhancing performance.
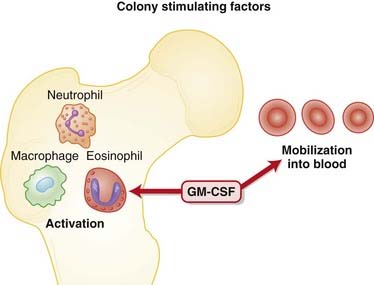
The chemical structure of epoetin alfa differs slightly from that of human endogenous erythropoietin. Although this difference does not have any clinical relevance, it has proven useful in trying to detect athletes who have been using epoetin alfa for blood doping. This is a practice by which athletes will try to stimulate an artificial increase in hematocrit before a competition to increase the oxygen-carrying capacity of their blood, presumably enhancing performance.Colony-Stimulating Factors



MOA (Mechanism of Action)
 Neutropenia is a common and serious side effect of cytotoxic cancer chemotherapy. Cytotoxic agents preferentially target rapidly dividing cells, including those of the bone marrow. The major complication of neutropenia is a reduced immune response, greatly increasing the probability of developing infections of both “normal” and opportunistic microbes.
Neutropenia is a common and serious side effect of cytotoxic cancer chemotherapy. Cytotoxic agents preferentially target rapidly dividing cells, including those of the bone marrow. The major complication of neutropenia is a reduced immune response, greatly increasing the probability of developing infections of both “normal” and opportunistic microbes.


Pharmacokinetics












Evidence
Colony-Stimulating Factor in Children with Acute Lymphocytic Leukemia
 A 2005 Cochrane review (six studies, N = 332 patients) looked at safety and effectiveness of adjunctive G-CSF or GM-CSF in children with acute lymphocytic leukemia (ALL). There was not enough data to assess survival. CSF significantly reduced the number of episodes of febrile neutropenia, length of hospitalization, and number of infectious disease episodes. CSF did not affect the length of neutropenia episodes or delays in chemotherapy episodes.
A 2005 Cochrane review (six studies, N = 332 patients) looked at safety and effectiveness of adjunctive G-CSF or GM-CSF in children with acute lymphocytic leukemia (ALL). There was not enough data to assess survival. CSF significantly reduced the number of episodes of febrile neutropenia, length of hospitalization, and number of infectious disease episodes. CSF did not affect the length of neutropenia episodes or delays in chemotherapy episodes.
B Vitamins






MOA (Mechanism of Action)
Vitamin B1
 Vitamin B1 is converted to thiamine in the body and is a coenzyme in carbohydrate metabolism, including the decarboxylation of pyruvic acid. Increased pyruvic acid levels are therefore indicative of vitamin B1 deficiency. Deficiency can lead to damage in regions of the brain, including the thalamus, midbrain, and brainstem, and this appears to be mediated, at least in part, by oxidative stress. This brain damage manifests as Wernicke-Korsakoff syndrome, a condition associated with alcoholism (Figure 16-13).
Vitamin B1 is converted to thiamine in the body and is a coenzyme in carbohydrate metabolism, including the decarboxylation of pyruvic acid. Increased pyruvic acid levels are therefore indicative of vitamin B1 deficiency. Deficiency can lead to damage in regions of the brain, including the thalamus, midbrain, and brainstem, and this appears to be mediated, at least in part, by oxidative stress. This brain damage manifests as Wernicke-Korsakoff syndrome, a condition associated with alcoholism (Figure 16-13).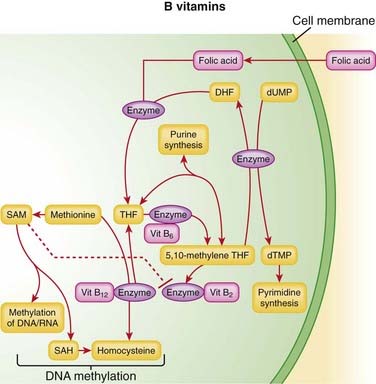
Vitamin B2
 The two coenzyme forms of vitamin B2 (riboflavin-5-phosphate and flavin adenine dinucleotide) play a role in adenosine triphosphate (ATP) production, through the metabolism of carbohydrates, fats, and proteins. Deficiency typically manifests as fissures in lips or cracks in the mouth, swelling of the tongue, or seborrheic dermatitis. Normochromic-normocytic anemias can also occur, as well as peripheral neuropathy.
The two coenzyme forms of vitamin B2 (riboflavin-5-phosphate and flavin adenine dinucleotide) play a role in adenosine triphosphate (ATP) production, through the metabolism of carbohydrates, fats, and proteins. Deficiency typically manifests as fissures in lips or cracks in the mouth, swelling of the tongue, or seborrheic dermatitis. Normochromic-normocytic anemias can also occur, as well as peripheral neuropathy.Niacin (Vitamin B3)







Pharmacokinetics


















Side Effects


Niacin
 At the recommended daily intake, niacin is well tolerated; however, when used as an antihyperlipidemic, it is often used at high doses, which can result in the following:
At the recommended daily intake, niacin is well tolerated; however, when used as an antihyperlipidemic, it is often used at high doses, which can result in the following:




Important Notes
 B12 preparations are available that contain intrinsic factor from animal sources. Although these might be useful initially in patients with intrinsic factor deficiency, patients typically become less responsive to the intrinsic factor, perhaps because of an antibody response launched against the animal protein.
B12 preparations are available that contain intrinsic factor from animal sources. Although these might be useful initially in patients with intrinsic factor deficiency, patients typically become less responsive to the intrinsic factor, perhaps because of an antibody response launched against the animal protein.



| Overdose Agent | Mechanism of Toxicity | Mechanism of Pyridoxine as Antidote |
|---|---|---|
| Isoniazid (INH) |
Evidence
Folic Acid with or without Vitamin B12 for Cognition
 A 2008 Cochrane review (eight studies, N = 1317 participants) examined the effects of folic acid supplementation, with or without vitamin B12, on healthy elderly or demented participants, in preventing cognitive impairment or slowing its progress. The authors found no evidence that folic acid, with or without B12, has a positive impact on mood and cognitive function in healthy elderly people.
A 2008 Cochrane review (eight studies, N = 1317 participants) examined the effects of folic acid supplementation, with or without vitamin B12, on healthy elderly or demented participants, in preventing cognitive impairment or slowing its progress. The authors found no evidence that folic acid, with or without B12, has a positive impact on mood and cognitive function in healthy elderly people.

FYI


 The preferred source of B vitamins for daily supplementation is from the diet. Food sources and recommended intakes are summarized in Table 16-2.
The preferred source of B vitamins for daily supplementation is from the diet. Food sources and recommended intakes are summarized in Table 16-2.TABLE 16-2 Sources and Recommended Dietary Intakes for Various B Vitamins
| Vitamin | Recommended Dietary Allowances | Sources |
|---|---|---|
| B1 (thiamine) |
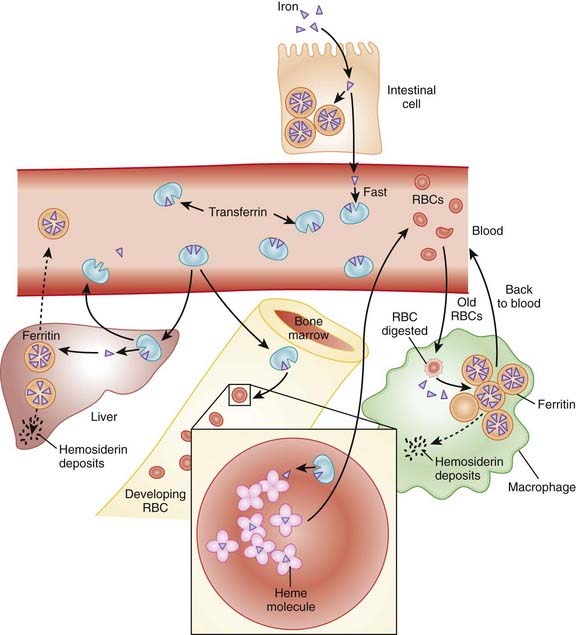
Iron




MOA (Mechanism of Action)
 Most iron is recycled through the body; RBCs contain the majority of iron in hemoglobin. Because the life span of an RBC is about 120 days, in 1 day about 0.8% of the RBCs are broken down, and their iron is recycled:
Most iron is recycled through the body; RBCs contain the majority of iron in hemoglobin. Because the life span of an RBC is about 120 days, in 1 day about 0.8% of the RBCs are broken down, and their iron is recycled:





Pharmacokinetics








Side Effects
Oral Administration




Important Notes
 Free inorganic iron is extremely toxic; therefore iron is quickly bound by transferrin and subsequently stored in the body in the form of hemoglobin, myoglobin, ferritin, and, to a small degree, transferrin. Hemoglobin and myoglobin constitute about 80% of all stored iron.
Free inorganic iron is extremely toxic; therefore iron is quickly bound by transferrin and subsequently stored in the body in the form of hemoglobin, myoglobin, ferritin, and, to a small degree, transferrin. Hemoglobin and myoglobin constitute about 80% of all stored iron.




 A number of laboratory measurements can be used for the diagnosis of iron deficiency. See Table 16-3.
A number of laboratory measurements can be used for the diagnosis of iron deficiency. See Table 16-3.







 Iron toxicity is treated with phlebotomy (removing blood) and iron chelators deferoxamine (parenteral), deferasirox (oral), and deferiprone (oral but not available in the United States). Phlebotomy is not indicated when the patient is anemic or being treating for anemia. Chelators are discussed further in Chapter 7.
Iron toxicity is treated with phlebotomy (removing blood) and iron chelators deferoxamine (parenteral), deferasirox (oral), and deferiprone (oral but not available in the United States). Phlebotomy is not indicated when the patient is anemic or being treating for anemia. Chelators are discussed further in Chapter 7.TABLE 16-3 Laboratory Measurements Used for Diagnosis of Iron Deficiency
| Hemoglobin | Low |
| Serum iron: measure of iron bound to serum ferritin | Low |
| Ferritin: ferritin level correlates with total body iron stores | Low |
| Total iron binding capacity (TIBC): refers to the number of unoccupied binding sites on transferrin and is determined by both the iron levels and the transferrin levels | High |
| Transferrin percent saturation: percent of iron bound to transferrin; a calculated value based on serum iron and TIBC | Low |
| Bone marrow iron | Low |














[/level-membership-for-basic-science-category][not-level-membership-for-basic-science-category]
Chapter 16 Hematology
Heparins
MOA (Mechanism of Action)
The coagulation (clotting) system is composed of many proteins. Most of these proteins are procoagulants, which means they contribute to clotting. Some proteins are anticoagulants that serve to keep the coagulation system in balance. When a protein is activated, its name is followed by a small letter a. Each activated protein serves as an enzyme for the next protein downstream in the cascade (Figure 16-1).Pharmacokinetics
Unfractionated Heparin
Very complex pharmacokinetics exist because there is a large range in molecular weight of the moleculesIndications
Treatment and prevention of inappropriate thrombosis
Important Notes
To measure the effect of UFH, the aPTT test is used (compare this with prothrombin time [PT] or International Normalized Ratio [INR], which is used with warfarin). It is a measure of time to coagulation (in the laboratory) and is measured in seconds. The higher the number, the more strongly a patient is anticoagulated.Evidence
LMWH versus Warfarin for Treatment of Venous Thromboembolism
A 2001 Cochrane review (seven studies, N = 1137 participants), updated in 2003, compared warfarin with LMWH for long-term treatment of VTE. There was no difference in the risk of recurrent VTE between warfarin and LMWH. There was a lower risk of bleeding with LMWH (odds ratio [OR] 0.38), and no difference in mortality rates between these two interventions was found.LMWH and Heparinoids versus UFH for Ischemic Stroke
A 2008 Cochrane review (nine studies, N = 3137 patients) compared LMWH and heparinoids (danaparoid) with UFH in patients with acute, presumed or confirmed ischemic stroke. The odds of developing a deep vein thrombosis (DVT) were reduced with LMWH compared with UFH (OR 0.55); however, the incidence of key clinical outcomes such as PE, death, and hemorrhage (intracranial or extracranial) was too small to provide a reliable comparison.Direct Factor Xa Inhibitors
MOA (Mechanism of Action)
The coagulation system is composed of many proteins: most of these proteins are procoagulants, which means they contribute to clotting. Some proteins are anticoagulants, which serve to keep the coagulation system in balance.Pharmacokinetics
Important Notes
There are no monitoring requirements for rivaroxaban. This and the fact that it is an orally administered agent suggest that drugs in its class, and perhaps the direct thrombin inhibitors, will supplant warfarin as the drugs of choice among oral anticoagulants.Advanced
Drug Interactions
CYP450 3A4 enzymes are involved in the metabolism of rivaroxaban; thus the potential exists for pharmacokinetic drug interactions with inhibitors or inducers of this isozyme. Rivaroxaban is also a P-glycoprotein (Pgp) substrate, and therefore its levels could also be affected by inhibitors or inducers of Pgp.Evidence
Postsurgical Venous Thromboembolism Prophylaxis
The RECORD trials were a series of double-blind randomized controlled trials that compared rivaroxaban with enoxaparin for the prophylactic treatment of VTE after total hip replacement (RECORD-1 and RECORD-2) or total knee replacement (RECORD-3 and RECORD-4). The trials were all relatively large, randomizing 2509 to 4541 patients between the two treatment groups. Rivaroxaban-treated patients had fewer events of VTE and all-cause deaths compared with enoxaparin in each of the four studies. The risk of bleeding was slightly higher with rivaroxaban than with enoxaparin.FYI
For a quick summary of the difference between two of the newer oral anticoagulants—direct factor Xa and direct thrombin inhibitors. Direct factor Xa inhibitors inhibit the formation of thrombin, whereas direct thrombin inhibitors allow thrombin to be formed but interfere with the actions of thrombin.Direct Thrombin Inhibitors
MOA (Mechanism of Action)
The coagulation (clotting) system is a multistep cascade that eventually leads to the formation of fibrin and development of a clot.Important Notes
All of the agents in this class are approved for prophylaxis of DVT and VTE after orthopedic surgery. Patients undergoing knee or hip replacement surgeries, in particular, are at high risk for developing a DVT or VTE. The risk is so high that these patients receive prophylactic anticoagulants for several days postsurgery.Vitamin K Antagonists
MOA (Mechanism of Action)
Indications
Important Notes
Warfarin therapy is monitored using the International Normalized Ratio (INR), which is a standardized form of the PT test. Because different laboratories use different reagents to test the PT, every laboratory generates a slightly different result, so the INR corrects for this discrepancy among laboratories.Evidence
Warfarin versus LMWH for Treatment of Venous Thromboembolism
A 2001 Cochrane review (seven studies, N = 1137 participants), updated in 2003, compared warfarin with LMWHs for long-term treatment of VTE. There was no difference in the risk of recurrent VTE between warfarin and LMWH. There was a lower risk of bleeding with LMWH (OR 0.38), and no difference in mortality rates between these two interventions.Warfarin versus Acetylsalicylic Acid for Atrial Fibrillation
A 2007 Cochrane review (eight studies, N = 9598 participants) compared warfarin with acetylsalicylic acid (ASA) in atrial fibrillation patients who had not had a prior stroke or transient ischemic attack (TIA). Treatment with warfarin led to a lower risk of stroke (OR 0.68), ischemic stroke (OR 0.53), and systemic emboli (OR 0.48). The risk of intracranial hemorrhage was increased with warfarin (OR 1.98). All-cause mortality and vascular deaths were similar between groups, and disabling or fatal strokes and MI were almost reduced with oral anticoagulants, but this did not reach statistical significance.Salicylates
MOA (Mechanism of Action)
Salicylates
Like nonsteroidal antiinflammatory drugs (NSAIDs), the salicylates work by inhibiting the actions of the cyclooxygenase (COX) enzyme (Figure 16-5).Aminosalicylates
 Although the aminosalicylates are related to salicylates in chemical structure, inhibition of prostaglandin (PG) synthesis is believed to play only a minor role, if any, in their efficacy in inflammatory bowel disease.
Although the aminosalicylates are related to salicylates in chemical structure, inhibition of prostaglandin (PG) synthesis is believed to play only a minor role, if any, in their efficacy in inflammatory bowel disease.Buy Membership for Basic Science Category to continue reading. Learn more here
[/not-level-membership-for-basic-science-category]
