Published on 18/03/2015 by admin
Filed under Dermatology
Last modified 22/04/2025
This article have been viewed 1791 times
James Lee Landero, Kurt W. Grelck and Carlos H. Nousari
Evidence Levels: A Double-blind study B Clinical trial ≥ 20 subjects C Clinical trial < 20 subjects D Series ≥ 5 subjects E Anecdotal case reports
Graft-versus-host disease (GVHD) affects the skin, liver, and gastrointestinal tract and typically occurs in the setting of allogeneic bone marrow transplants. Host disease results from interactions between adaptive and innate immune systems of both host and donor (graft), in which host tissues are identified as foreign by the graft.
Acute GVHD (aGVHD) classically occurs 100 days after transplantation (usually several weeks) and presents as a maculopapular eruption which may progress to erythroderma, and less commonly to a toxic epidermal necrolysis-like eruption. Dermatologic findings are frequently accompanied by diarrhea and rising bilirubin levels.
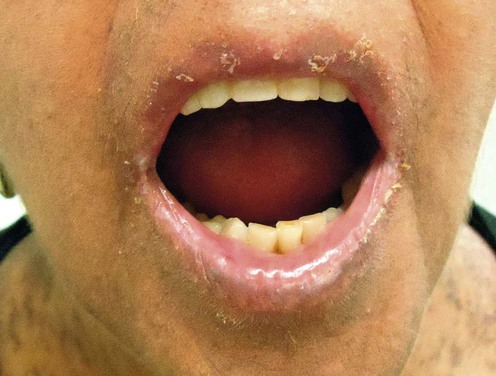
Chronic GVHD (cGVHD) occurs 100 days after transplantation as a mucocutaneous lichen-planus-like eruption and/or sclerodermatous process, with hepatic, gastrointestinal, and pulmonary pathology.
Treatment, timing and presentation of GVHD depend on the type of transplant, pre-transplantation ablative therapy, marrow preparation, prophylactic medications, and previous treatments. Evolution of transplant strategies such as reduced-intensity conditioning, and donor lymphocyte infusion, combined with recognition of overlap phenomena, and late-onset aGVHD, have blurred the classic temporally defined division of aGVHD and cGVHD.
Prevention of GVHD is typically with a combination of methotrexate (MTX) and calcineurin inhibitor, with or without additional corticosteroids. Combinations using tacrolimus, cyclophosphamide, or mycophenolate mofetil (MMF) are also effective. Sirolimus, thalidomide, hydroxychloroquine, muromonab-CD3, alemtuzumab, suberoylanilide hydroxamic acid, keratinocyte growth factor, IL-1 receptor antibody, IL-2 receptor antibody, antithymocyte globulin, intravenous immunoglobulin, pentostatin, and extracorporeal photopheresis (ECP) have also been evaluated with mixed or preliminary results. Corticosteroids are not part of prophylaxis in spite of reductions in mild and severe aGVHD, as overall survival, disease-free survival, and incidence of relapse are not affected.
Following transplantation, 25–80% will manifest with aGVHD. For stage I aGVHD topical steroids are reasonable with or without phototherapy. For grade II-IV aGVHD first-line therapy is systemic corticosteroids, given in consultation with a transplant specialist (methylprednisolone 2 mg/kg/day, with eventual taper). If within 5 days there is no response, second-line therapy should be considered. Response to first-line therapy is the most important factor predicting long-term survival.
Second-line therapy should be initiated after non-response to high-dose steroids for 3 to 5 days, with MMF, tacrolimus, pentostatin, or antithymocyte globulin. Well designed trials do not exist to adequately compare therapies. Supportive care includes cessation of oral intake, total parenteral nutrition with hyperalimentation, antibiotic and antiviral prophylaxis, and pain control.
cGVHD treatment depends on extent of organ involvement. Skin or mucosal disease requires local therapy, whereas extensive disease (generalized cutaneous or localized cutaneous with visceral involvement) requires systemic therapy. Standard treatment is a combination of systemic corticosteroids with or without calcineurin inhibitor (prednisone 1 mg/kg/day and cyclosporine 10 mg/kg/day given as an alternating day regimen).
Refractory cGVHD has no standard therapy due to a lack of randomized controlled trials. Patients refractory to corticosteroids should be considered for clinical trials. Studies show MMF alone or in combination with cyclosporine, or tacrolimus, is beneficial in refractory disease. ECP is becoming reasonable first-line therapy in refractory cGVHD, where available. For sclerodermatous disease, salvage therapy with imatinib, or mTOR inhibitors are advocated. Lichenoid disease responds more with non-pharmacologic therapies such as 8-methoxypsoralen plus ultraviolet A irradiation (PUVA), and ECP.
Skin biopsy
Medication history
Liver function tests
Complete blood count
Serum chemistries
Biomarker panel
Consideration for viral testing
Consideration for colonoscopy/endoscopy
Clinical differentiation of acute cutaneous graft-versus-host disease from drug hypersensitivity reactions.
Byun HJ, Yang JI, Kim BK, Cho KH. J Am Acad Dermatol 2011; 65:726–32.
Facial and hand-foot involvement suggests GVHD, whereas rashes greater than 2 to 3 days’ duration without diarrhea or hyperbilirubinemia are suggestive of drug effects.
Role of skin biopsy to confirm suspected acute graft-vs-host disease: results of decision analysis.
Firoz BF, Lee SJ, Nghiem P, Qureshi AA. Arch Dermatol. 2006; 142: 175.
Best outcomes are obtained from immediate treatment initiation rather than waiting for guidance from biopsy.
Acute graft-versus-host disease biomarkers measured during therapy can predict treatment outcomes: a Blood and Marrow Transplant Clinical Trials Network Study.
Levine JE, Logan BR, Wu J, Alousi AM, Bolaños-Meade J, et al. Blood 2012; 119: 3854–60.
Six validated biomarkers (IL-2 receptor-α, tumor necrosis factor receptor-1, hepatocyte growth factor, IL-8, elafin, and regenerating islet-derived 3-α) identified patients at high or low risk of treatment non-responsiveness or death.
Early treatment of acute graft-versus-host disease with high- or low-dose 6-methylprednisolone: a multicenter randomized trial from the Italian Group for Bone Marrow Transplantation.
Van Lint MT, Uderzo C, Locasciulli A, Majolino I, Scimé R, Locatelli F, et al. Blood 1998; 92: 2288–93.
Comparison of methylprednisolone 2 mg/kg/day vs 10 mg/kg/day, for 5 days, with those non-responsive on low-dose switched to high-dose therapy. There were no differences in mean response rates or survival at 3 years.
Low-dose steroids are an appropriate initial regimen with non-responders given high-dose therapy or alternative agents.
First- and second-line systemic treatment of acute graft-versus-host disease: recommendations of the American Society of Blood and Marrow Transplantation.
Martin PJ, Rizzo JD, Wingard JR, Ballen K, Curtin PT, Cutler C, et al. Biol Blood Marrow Transpl 2012.
An excellent review of primary and secondary treatments for aGVHD.
Steroid-refractory acute GVHD: lack of long-term improved survival using new generation anticytokine treatment.
Xhaard A, Rocha V, Bueno B, de Latour RP, Lenglet J, Petropoulou A, et al. Biol Blood Marrow Transplant 2012; 18: 406–13.
No consensus for treatment of refractory aGVHD exists. Oerall response rate was similar between MMF, inolimomab, and etanercept, although infectious bacterial complications were higher with anticytokines.
Etanercept, mycophenolate, denileukin, or pentostatin plus corticosteroids for acute graft-versus-host disease: a randomized phase 2 trial from the Blood and Marrow Transplant Clinical Trials Network.
Alousi AM, Weisdorf DJ, Logan BR, Bolaños-Meade J, Carter S, Difronzo N, et al. Blood 2009; 114: 511–17.
MMF with corticosteroids was compared to etanercept, pentostatin, and denileukin difitox. MMF had the highest complete response rates, overall survival (64%), and lowest infection rates; however, this trial was under-powered for comparison among treatment arms.
Role of extracorporeal photopheresis (ECP) in treatment of steroid-refractory acute graft-versus-host disease.
Greinix HT, Worel N, Knobler R. Biol Blood Marrow Transplant 2010; 16: 1747–8.
ECP has an excellent safety profile and can induce complete response of grade I-IV steroid-refractory aGVHD.
A phase III study of infliximab and corticosteroids for the initial treatment of acute graft-versus-host disease.
Couriel DR, Saliba R, de Lima M, Giralt S, Andersson B, Khouri I, et al. Biol Blood Marrow Transplant. 2009; 15: 1555–62.
Although several case series demonstrated benefit from infliximab, this trial’s 63 patients with grade II-IV aGVHD had no benefit compared to methylprednisolone alone.
Etanercept plus methylprednisolone as initial therapy for acute graft-versus-host disease.
Levine JE, Paczesny S, Mineishi S, Braun T, Choi SW, Hutchinson RJ, et al. Blood 2008; 111: 2470–5.
Etanercept with corticosteroids was more likely to achieve complete response than patients treated with steroids alone (69% vs 33%).
Inflammatory cytokine inhibition with combination daclizumab and infliximab for steroid-refractory acute GVHD.
Rager A, Frey N, Goldstein SC, Reshef R, Hexner EO, Loren A, et al. Bone Marrow Transplant 2011; 46: 430–5.
Seventeen patients had a 47% clinical response rate for refractory aGVHD; however, all patients died at a median 35 days following treatment.
Sirolimus for treatment of steroid-refractory acute graft-versus-host disease.
Hoda D, Pidala J, Salgado-Vila N, Kim J, Perkins J, Bookout R, et al. Bone Marrow Transplant 2010; 45: 1347–51.
Thirty-four patients with refractory aGVHD had an overall response rate of 76%, with 44% achieving complete response.
Diagnosis and management of acute graft-versus-host disease.
Dignan FL, Clark A, Amrolia P, Cornish J, Jackson G, Mahendra P, et al. Br J Haematol 2012.
Evidence-based guidelines for aGVHD. Pentostatin, alemtuzumab, mesenchymal stem cells, and MTX are third-line therapies, used after second-line agents have failed or in clinical trials. Agents relegated to a possible role in aGVHD are antithymocyte globulin, and ex-vivo expanded regulatory T cells. Agents not recommended include: rituximab (data limited), visilizumab, intra-arterial methylprednisolone, thalidomide, azathioprine, and anti-CD147 antibody.
Narrowband ultraviolet B phototherapy for treatment of steroid-refractory and steroid-dependent acute graft-versus-host disease.
Feldstein JV, Bolaños-Meade J, Anders VL, Abuav R. J Am Acad Dermatol 2011; 65: 733–8.
Of 14 patients with cutaneous predominant aGVHD, only 21% had no response.
Skin biopsy (4 mm punch from forearm and back)
Direct immunofluorescence (to exclude paraneoplastic pemphigus)
Schirmer’s test (<5 mm wetting)
Pulmonary function tests/ABG analysis
Serum immunoglobulins
Quality of life assessment
Evaluation of other organs (ocular, mucosal, gastrointestinal, neurologic, endocrine)
Diagnosis and management of chronic graft-versus-host disease.
Dignan FL, Amrolia P, Clark A, Cornish J, Jackson G, Mahendra P, et al. Br J Haematol 2012.
Update and review of diagnosis and staging of cGVHD. Grading correlates with prognosis and survival.
National Institutes of Health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: I. Diagnosis and staging working group report.
Filipovich AH, Weisdorf D, Pavletic S, Socie G, Wingard JR, Lee SJ, et al. Biol Blood Marrow Transplant 2005; 11: 945–56.
Diagnosis requires >1 clinical manifestation and confirmation by biopsy or other relevant tests (e.g., Schirmer). Standardization of response criteria, staging, and grading are detailed. Response and data collection forms are available at www.asbmt.org.
Recommended screening and preventive practices for long-term survivors after hematopoietic cell transplantation: joint recommendations of the European Group for Blood and Marrow Transplantation, the Center for International Blood and Marrow Transplant Research, and the American Society of Blood and Marrow Transplantation.
Rizzo JD, Wingard JR, Tichelli A, Lee SJ, Van Lint MT, Burns LJ, et al. Biol Blood Marrow Transplant 2006; 12: 138–51.
Comprehensive organ system based screening recommendations are detailed.
Consensus Conference on Clinical Practice in ChronicGVHD: Second-Line Treatment of Chronic Graft-versus-Host Disease.
Wolff D, Schleuning M, von Harsdorf S, Bacher U, Gerbitz A, Stadler M, et al. Biol Blood Marrow Transplant 2011; 17: 1–17.
Corticosteroids remain primary therapy, although there are no adequate trials comparing dose. Standard dose is 1 mg/kg/day, with eventual taper depending on clinical response.
Therapy for chronic graft-versus-host disease: a randomized trial comparing cyclosporine plus prednisone versus prednisone alone.
Koc S, Leisenring W, Flowers ME, Anasetti C, Deeg HJ, Nash RA, et al. Blood 2002; 100: 48–51.
287 cGVHD patients were given prednisone versus prednisone and cyclosporine, with no difference in efficacy or median interval to therapy discontinuation. The combination arm had a reduced rate of avascular necrosis.
Secondary therapies lack controlled trials for comparison. ECP (skin, oral, and liver disease), mTOR inhibitors, pentostatin, rituximab (skin, musculoskeletal disease), and imatinib (sclerotic skin, lung disease) are recommended secondary agents. If second-line treatment fails, a different second-line treatment should be offered prior to third-line agents.
Progressive improvement in cutaneous and extracutaneous chronic graft-versus-host disease after a 24-week course of extracorporeal photopheresis: results of a crossover randomized study.
Greinix HT, van Besien K, Elmaagacli AH, Hillen U, Grigg A, Knobler R, et al. Biol Blood Marrow Transplant 2011; 17: 1775–82.
Following positive results of standard therapy plus ECP versus standard therapy, patients with inadequate response on standard benefited from ECP. Improved results were seen with cutaneous, oral, hepatic, pulmonary, and ocular disease.
Therapy of sclerodermatous chronic graft-versus-host disease with mammalian target of rapamycin inhibitors.
Jedlickova Z, Burlakova I, Bug G, Baurmann H, Schwerdtfeger R, Schleuning M. Biol Blood Marrow Transplant 2011; 17: 657–63.
Thirty-four patients with severe sclerodermatous cGVHD had an overall response rate of 76%. Hyperlipidemia, poor wound healing, and thrombotic microangiopathy were seen in a minority.
Weekly rituximab followed by monthly rituximab treatment for steroid-refractory chronic graft-versus-host disease: results from a prospective, multicenter, phase II study.
Kim SJ, Lee JW, Jung CW, Min CK, Cho B, Shin HJ, et al. Haematologica 2010; 95: 1935–42.
Of 37 patients treated with rituximab, eight patients showed complete and 24 patients had partial responses. Results improved with cutaneous, oral, and musculoskeletal involvement. Infectious complications were increased.
Phase II study of pentostatin in patients with corticosteroid-refractory chronic graft-versus-host disease.
Jacobsohn DA, Chen AR, Zahurak M, Piantadosi S, Anders V, Bolaños-Meade J, et al. J Clin Oncol 2007; 25: 4255–61.
Fifty-eight previously treated patients (median four previous regimens) were given pentostatin 4 mg/m2 every 2 weeks for 12 doses. Overall response rate was 55% with major improvements in 31 patients. Survival was 70% at 2 years with infectious complications predominant.
Graft-versus-host disease: part II. Management of cutaneous graft-versus-host disease.
Hymes SR, Alousi AM, Cowen EW. J Am Acad Dermatol 2012; 66: 535.
PUVA, PUVA bath, UVB, narrowband (NB)-UVB, and UVA1 have shown efficacy in small series. Lichenoid manifestations respond to UVB and NB-UVB, while PUVA and UVA1 are better for sclerodermatous disease.
Mesenchymal stem cell as salvage treatment for refractory chronic GVHD.
Weng JY, Du X, Geng SX, Peng YW, Wang Z, Lu ZS, et al. Bone Marrow Transplant 2010; 45: 1732–40.
Of 19 patients with cGVHD, there was a 2-year survival rate of 77.7%.
Evaluation of mycophenolate mofetil for initial treatment of chronic graft-versus-host disease.
Martin PJ, Storer BE, Rowley SD, Flowers ME, Lee SJ, Carpenter PA, et al. Blood 2009; 113: 5074–82.
There was no benefit from adding MMF to the systemic regimen.
Other series have shown response rates between 40% and 75%, with high rates of infectious complications.
Effectiveness of subcutaneous low-dose alemtuzumab and rituximab combination therapy for steroid-resistant chronic graft-versus-host disease.
Gutiérrez-Aguirre CH, Cantú-Rodríguez OG, Borjas-Almaguer OD, González-Llano O, Jaime-Pérez JC, Solano-Genesta M, et al. Haematologica 2012; 97: 717–22.
Combination treatment of 15 patients had 33% complete, and 50% partial remissions. Adverse effects were mainly infectious.
Treatment of Skin Disease Comprehensive Therapeutic Strategies 4e
WhatsApp us








 Corticosteroids (methylprednisolone 2 mg/kg/day)
Corticosteroids (methylprednisolone 2 mg/kg/day) Mycophenolate mofetil
Mycophenolate mofetil Extracorporeal photopheresis
Extracorporeal photopheresis Monoclonal antibodies:
Monoclonal antibodies: Cyclosporine
Cyclosporine Tacrolimus
Tacrolimus Sirolimus
Sirolimus
 Pentostatin
Pentostatin Antithymocyte globulin
Antithymocyte globulin Mesenchymal stem cells
Mesenchymal stem cells Methotrexate
Methotrexate Anti-CD52 antibody (alemtuzumab)
Anti-CD52 antibody (alemtuzumab) Anti-CD3 antibody (visilizumab)
Anti-CD3 antibody (visilizumab) Anti-CD2 antibody (siplizumab)
Anti-CD2 antibody (siplizumab) Intra-arterial methyprednisolone
Intra-arterial methyprednisolone CD5-specific immunotoxin
CD5-specific immunotoxin Denileukin diftitox
Denileukin diftitox Rituximab
Rituximab Ustekinumab
Ustekinumab Cyclophosphamide
Cyclophosphamide PUVA
PUVA Narrowband UVB
Narrowband UVB Tocilizimab
Tocilizimab








 Systemic corticosteroids
Systemic corticosteroids Systemic corticosteroid and calcineurin inhibitor
Systemic corticosteroid and calcineurin inhibitor Extracorporeal photopheresis
Extracorporeal photopheresis mTOR inhibitors (sirolimus, tacrolimus, everolimus)
mTOR inhibitors (sirolimus, tacrolimus, everolimus) Rituximab
Rituximab Pentostatin
Pentostatin UVB, narrow-band UVB
UVB, narrow-band UVB PUVA
PUVA Extracorporeal photopheresis
Extracorporeal photopheresis Imatinib
Imatinib UVA1/PUVA
UVA1/PUVA Etretinate
Etretinate Topical halofuginone
Topical halofuginone
 Mycophenolate mofetil
Mycophenolate mofetil Thalidomide
Thalidomide Hydroxychloroquine
Hydroxychloroquine Cyclophosphamide
Cyclophosphamide Pentostatin
Pentostatin Infliximab
Infliximab Etanercept
Etanercept Daclizumab
Daclizumab Alefacept
Alefacept Alemtuzumab
Alemtuzumab Mesenchymal stromal cell therapy
Mesenchymal stromal cell therapy Interleukin-2
Interleukin-2 Thoracoabdominal irradiation
Thoracoabdominal irradiation Azathioprine
Azathioprine Low-dose methotrexate
Low-dose methotrexate Pulse corticosteroids
Pulse corticosteroids Clofazimine
Clofazimine UVA1 and mycophenolate mofetil
UVA1 and mycophenolate mofetil Topical corticosteroids
Topical corticosteroids Topical cyclosporine
Topical cyclosporine Intraoral PUVA
Intraoral PUVA Oral UVB
Oral UVB Topical calcineurin inhibitors
Topical calcineurin inhibitors Topical azathioprine
Topical azathioprine