Chapter 13 Dermatology
Retinoids




Moa (Mechanism of Action)
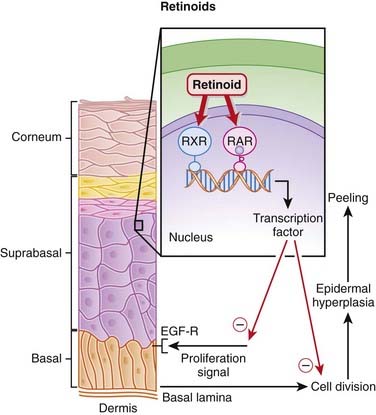
 A retinoid is a molecule (or a metabolite of a molecule) that binds to and activates RARs. There are also retinoid X receptors (RXRs), which also play a role in transducing retinoid signaling (Figure 13-1).
A retinoid is a molecule (or a metabolite of a molecule) that binds to and activates RARs. There are also retinoid X receptors (RXRs), which also play a role in transducing retinoid signaling (Figure 13-1).


Acne










Pharmacokinetics










Contraindications


Side Effects

















Important Notes




Evidence
Photoaged Skin
 A Cochrane review in 2005 (eight studies, N = 460) showed that topical tretinoin cream in concentrations of 0.02% or higher was superior to placebo for participants with mild to severe photodamage on the face and forearms. The relative risk of improvement for 0.05% tretinoin cream compared with placebo (three studies) at 24 weeks was 1.73. This effect was not seen for 0.001% (one study) or 0.01% (three studies) topical tretinoin. A dose-response relationship was evident for both effectiveness and skin irritation.
A Cochrane review in 2005 (eight studies, N = 460) showed that topical tretinoin cream in concentrations of 0.02% or higher was superior to placebo for participants with mild to severe photodamage on the face and forearms. The relative risk of improvement for 0.05% tretinoin cream compared with placebo (three studies) at 24 weeks was 1.73. This effect was not seen for 0.001% (one study) or 0.01% (three studies) topical tretinoin. A dose-response relationship was evident for both effectiveness and skin irritation.









Steroids, Topical
Common Drugs




Moa (Mechanism of Action)
 As topical agents, steroids are used for their antiinflammatory properties, which are exerted through the following mechanisms:
As topical agents, steroids are used for their antiinflammatory properties, which are exerted through the following mechanisms:
 Inhibition of the release of phospholipase A2, which is the principle enzyme for the formation of arachidonic acid–based inflammatory mediators prostaglandins and leukotrienes.
Inhibition of the release of phospholipase A2, which is the principle enzyme for the formation of arachidonic acid–based inflammatory mediators prostaglandins and leukotrienes.



 The second benefit topical steroids provide to skin is immunosuppression, which is mediated through the following:
The second benefit topical steroids provide to skin is immunosuppression, which is mediated through the following:













Pharmacokinetics
Absorption
 Corticosteroids are only minimally absorbed after application to normal skin—for example, approximately 1% of a dose of hydrocortisone solution is absorbed.
Corticosteroids are only minimally absorbed after application to normal skin—for example, approximately 1% of a dose of hydrocortisone solution is absorbed.



Potency

 The delivery vehicle can exert a large influence on the potency of a topical steroid. Combinations of powders, oils, and water-based liquids comprise the vehicles. Combinations of ingredients in these three forms in varying proportions make up the most commonly used and are vehicles:
The delivery vehicle can exert a large influence on the potency of a topical steroid. Combinations of powders, oils, and water-based liquids comprise the vehicles. Combinations of ingredients in these three forms in varying proportions make up the most commonly used and are vehicles:
 Ointments are water suspended in oil and are the most potent because of their occlusive effect, but are greasy and not useful on hairy areas. Ointments should be applied two or three times per day, particularly after the skin has been moistened. They are useful for dry lesions because they form a water barrier.
Ointments are water suspended in oil and are the most potent because of their occlusive effect, but are greasy and not useful on hairy areas. Ointments should be applied two or three times per day, particularly after the skin has been moistened. They are useful for dry lesions because they form a water barrier.





















































Side Effects
 All side effects are more common with higher-potency steroids, larger surface areas treated, and longer durations of treatment.
All side effects are more common with higher-potency steroids, larger surface areas treated, and longer durations of treatment. Skin atrophy: Skin atrophy is demonstrated by thin shiny-appearing skin, telangiectasia (small readily visible blood vessels), ecchymoses (bruises), striae (stretch marks), hypertrichosis (increased hair), redness, and pigmentation changes.
Skin atrophy: Skin atrophy is demonstrated by thin shiny-appearing skin, telangiectasia (small readily visible blood vessels), ecchymoses (bruises), striae (stretch marks), hypertrichosis (increased hair), redness, and pigmentation changes.










Important Notes
 There are many different topical steroids. Through modification of the original steroid (hydrocortisone), the antiinflammatory potency, mineralocorticoid versus glucocorticoid ratio, and side effects are changed.
There are many different topical steroids. Through modification of the original steroid (hydrocortisone), the antiinflammatory potency, mineralocorticoid versus glucocorticoid ratio, and side effects are changed.






Evidence
Steroids and Psoriasis
 A 2009 Cochrane review (16 studies, N = 1916 patients) found that use of potent and very potent steroids over a 2- to 3-week period by patients with psoriasis resulted in statistically significant improvement, as measured by an “investigator assessment of overall global improvement.” Note that duration of effect investigated is short and that psoriasis is a chronic disease.
A 2009 Cochrane review (16 studies, N = 1916 patients) found that use of potent and very potent steroids over a 2- to 3-week period by patients with psoriasis resulted in statistically significant improvement, as measured by an “investigator assessment of overall global improvement.” Note that duration of effect investigated is short and that psoriasis is a chronic disease.
Keratolytics


Moa (Mechanism of Action)
 Keratin is a fibrous insoluble protein found in the skin, hair, and nails. In some dermatologic conditions the amount of keratin is increased, resulting in a thicker epidermis termed hyperkeratosis. One of the most commonly recognized causes of hyperkeratosis is warts. Psoriasis and eczema are two other common hyperkeratotic conditions.
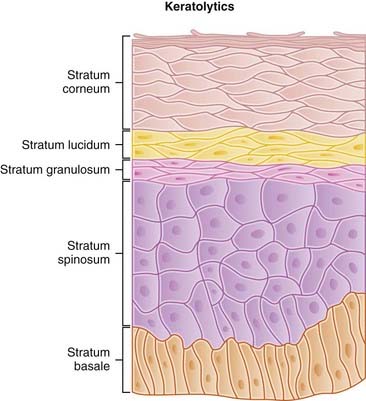
Keratin is a fibrous insoluble protein found in the skin, hair, and nails. In some dermatologic conditions the amount of keratin is increased, resulting in a thicker epidermis termed hyperkeratosis. One of the most commonly recognized causes of hyperkeratosis is warts. Psoriasis and eczema are two other common hyperkeratotic conditions. The stratum corneum is the outermost layer of the epidermis where the keratin is present; it is composed of the dead squamous cells that are produced in the stratum germinativum. The primary roles of the stratum corneum are to prevent water evaporation and to impart physical strength to the skin (Figure 13-2).
The stratum corneum is the outermost layer of the epidermis where the keratin is present; it is composed of the dead squamous cells that are produced in the stratum germinativum. The primary roles of the stratum corneum are to prevent water evaporation and to impart physical strength to the skin (Figure 13-2).




Pharmacokinetics










Important Notes






Imiquimod

Moa (Mechanism of Action)
 Imiquimod enhances both the innate and the acquired immune systems and thereby stimulates a response against abnormal skin cells, which are then eliminated through the body’s own mechanisms.
Imiquimod enhances both the innate and the acquired immune systems and thereby stimulates a response against abnormal skin cells, which are then eliminated through the body’s own mechanisms.





Pharmacokinetics






Side Effects








Important Notes
 Lesions suspected to be cancerous (basal cell carcinoma) should be biopsy proven before therapy is started. Treatment success rates are about 80% with imiquimod alone.
Lesions suspected to be cancerous (basal cell carcinoma) should be biopsy proven before therapy is started. Treatment success rates are about 80% with imiquimod alone.



Advanced







Evidence
Imiquimod versus Vehicle (Placebo) for Basal Cell Carcinoma
 A Cochrane review in 2007 (five studies N = 1145 patients) found a short-term success rate (defined histologically with biopsy) of 87% to 88% at 6 weeks and 76% at 12 weeks. This was a not a comparison with other therapy, but a trial comparing surgery with imiquimod is underway. Furthermore, 12 weeks is a very short period of time to declare success in cancer treatment. More studies are required to define the usefulness of imiquimod in treatment of basal cell carcinoma.
A Cochrane review in 2007 (five studies N = 1145 patients) found a short-term success rate (defined histologically with biopsy) of 87% to 88% at 6 weeks and 76% at 12 weeks. This was a not a comparison with other therapy, but a trial comparing surgery with imiquimod is underway. Furthermore, 12 weeks is a very short period of time to declare success in cancer treatment. More studies are required to define the usefulness of imiquimod in treatment of basal cell carcinoma.