CHAPTER 12 The ankle
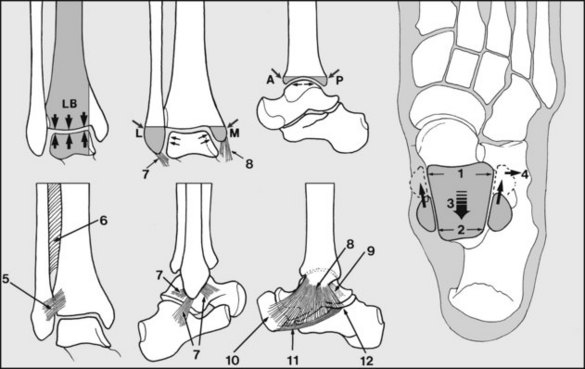
Fig. 12.A
Anatomical Features
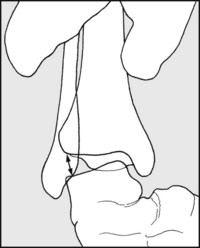
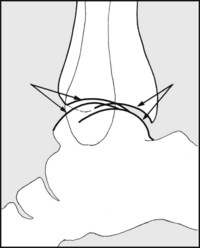
The ankle joint is basically a simple hinge joint, normally permitting movement in one plane (dorsiflexion and plantarflexion), but in addition, up to 18° of axial rotation of the talus in the tibial mortice may occur. Load-bearing stresses (LB) are taken by the upper articular surface of the talus and the tibia; the fibula plays no part in this.
Medial displacement (translation) of the talus is prevented by the medial malleolus (M), and lateral displacement by the lateral malleolus (L). Posterior talar shift is blocked by the downward-projecting curved articular surface of the tibia (P) behind, and the corresponding surface in front (A) prevents anterior subluxation. Any of these bony prominences may be fractured, resulting in potential instability.
When viewed from above, the articular surface of the talus may be seen to be wider anteriorly (1) than posteriorly (2). This means that as the ankle is dorsiflexed (3), the talus is gripped more firmly between the malleoli and pushes the fibula laterally (4). When the ankle is plantarflexed there is a greater degree of freedom (and instability) of the talus in the ankle mortice.
The natural congruency of the bony components of the ankle accounts for its inherent stability and this is reinforced by the disposition and strength of the associated ligaments. These include the following:
Note that a careful examination of the foot is often also required in the investigation of many ankle complaints.
Soft Tissue Injuries of the Ankle
Soft tissue injuries of the ankle are extremely common and in more severe cases difficult to differentiate from undisplaced fractures. Radiographic examination is essential in all but the most minor lesions, and is also necessary where symptoms are persistent. When fracture has been excluded after a significant injury a diagnosis has still to be made, as this manifestly affects treatment.
Injuries of the Lateral Ligament
The lateral ligament is damaged through inversion injuries. In an incomplete tear, some fibres only are ruptured (ankle sprain). Treatment is then symptomatic and a full early recovery can be expected. When the ligament is completely torn or detached from the fibula, the talus is free to tilt in the mortice of the tibia and fibula. If the lateral ligament fails to heal, chronic instability of the ankle results. If this injury is diagnosed in the acute stages, it should be treated by prolonged immobilisation in a plaster cast or orthosis, or by operative repair. In late-diagnosed cases good results generally follow lateral ligament reconstruction procedures.
In functional instability of the ankle the patient complains of frequent sensations of the ankle giving way, and pain, stiffness and swelling related to activity, but no evidence of ligament laxity can be found. It is thought that in many of these cases there is a degree of motor incoordination arising from some disorder of proprioception. Most respond to specialised physiotherapy (using tilt boards and other measures to improve muscular coordination).
Inferior Tibiofibular Ligaments
When the foot is dorsiflexed the distal end of the fibula moves laterally (and proximally) as it is engaged by the wedge-shaped upper articular surface of the talus. This movement is restricted by the inferior tibiofibular ligaments, and to a lesser extent the interosseous membrane. Damage to these structures may lead to lateral displacement of the fibula and lateral drift of the talus (diastasis). In treatment, the talus must be realigned with the tibia and any fibular displacement reduced. This reduction may be held by cross-screwing of the fibula to the tibia, or by plaster fixation.
Medial Ligament
The medial ligament is immensely strong, and if stressed in ankle joint injuries it generally avulses the medial malleolus rather than itself tearing. Nevertheless, tears do occur, and are seen particularly in conjunction with lateral malleolar fractures. Meticulous reduction of any associated fracture is essential, and this often requires an open procedure. Operative repair of the ligament may be required.
Achilles Tendon (Tendo Calcaneus)
Achilles Tendinopathy
This generally results from excessive repetitive overload of the tendon to a degree that exceeds its capacity to recover. The preferred term ‘tendinopathy’ includes a number of conditions which may only be differentiated by direct inspection and histological examination of the tendon or surrounding structures. These include tendinitis, where there is a clear inflammatory process involving the tendon; tendinosis, where there is collagen degeneration within the tendon; and paratendinitis, when there are inflammatory changes in the sheath of the tendon.
The condition is common in athletes, particularly runners and jumpers, but also in footballers, tennis players and ballet dancers. It gives rise to localised pain which is related to lower limb activity. In severe cases of tendinopathy there may be progressive weakness of plantarflexion, accompanied by impaired function and, in some cases, spontaneous rupture of the tendon.
Most cases are treated conservatively by restricting activities, supplemented when required by physiotherapy in the form of tendon stretching exercises, tendon massage, orthotic devices for the shoes, and therapeutic ultrasound. In some resistant cases surgical measures such as the removal of fibrotic nodules from within the tendon and the release of tendon adhesions may be required.
Acute Traumatic Achilles Tendon Rupture
Sudden plantarflexion of the foot may rupture the Achilles tendon, especially when it is weakened as a result of tendinosis and the degenerative changes often seen in middle age. Surgical repair may be carried out, although in most cases excellent results may be achieved by conservative management in a plaster cast or an orthosis.
Other Common Conditions Seen Around the Ankle
Tenosynovitis
Inflammatory changes in the tendon sheaths behind the malleoli may give rise to pain at the sides of the ankle joint. Tenosynovitis may follow unusual excessive activity or be associated with degenerative changes, flat foot or rheumatoid arthritis. There is puffy swelling in the line of the tendons, with tenderness extending often for several centimetres along their length. Tibialis posterior and peroneus longus are most frequently involved, and stretching of these structures during inversion and eversion of the foot gives rise to pain. Spontaneous rupture is not uncommon. Symptoms generally respond to immobilisation for short periods in a below-knee walking plaster or an orthosis.
Footballer’s Ankle
Ill-localised pain in the front of the ankle may follow repeated incidents of forced plantarflexion of the foot which result in tearing of the anterior capsule of the ankle joint. This occurs frequently in footballers, where this form of stress is common. Calcification in the resulting areas of avulsion and haemorrhage leads to the appearance of characteristic exostoses, which show in lateral radiographic projections of the ankle. These may lead to mechanical restriction of dorsiflexion.
Osteochondritis of the Talus
Although rather uncommon, this condition, which is seen most frequently in adolescents and young men, may give disabling pain in the ankle. It is now generally agreed that the condition starts as an osteochondral fracture. It is the frequent source of complaints of chronic disability following a so-called simple sprain of the ankle. The diagnosis is made on the radiological findings, although the site of the pain and local tenderness over the upper articular surface of the talus may lead one to suspect it. CT and MRI scans are invaluable in doubtful cases. If loose bodies are produced, they must be excised. The treatment of the local lesion follows in principle that of osteochondritis dissecans of the knee.
Snapping Peroneal Tendons
This is an uncommon cause of ankle pain and is due to tearing of the superior peroneal retinaculum. The patient complains of a clicking sensation in the ankle and is usually able to demonstrate the peroneal tendons riding over the lateral malleolus. The treatment is by surgical reconstruction of the retinaculum.
Osteoarthritis
Primary osteoarthritis of the ankle is rare. Secondary osteoarthritis is sometimes seen after ankle fractures, avascular necrosis of the talus, or osteochondritis of the talus.
Rheumatoid Arthritis
Rheumatoid arthritis of the ankle is not uncommon but is seldom seen as a primary manifestation of the disease, so that the diagnosis seldom presents difficulty.
Tuberculosis
Tuberculous infections of the ankle joint are now rare in the UK. When they occur there is swelling of the joint, wasting of the calf, and the usual signs of inflammation. The patient develops a painful limp, and as the joint is comparatively superficial, sinus formation is common at a comparatively early stage.
Shortening of the Achilles Tendon (Tendo Calcaneus)
Shortening of the Achilles tendon results in plantarflexion of the foot and clumsiness of gait as the heel fails to reach the ground. The more severe degrees of Achilles tendon shortening are accompanied by a tendency to flat foot. In many cases flexion of the knee, by taking the tension off the gastrocnemius, will permit dorsiflexion of the foot. Shortening of the Achilles tendon may occur as an apparently isolated condition with no obvious predisposing cause, but in a great many cases it is associated with congenital deformities of the foot or neurological disorders, of which subclinical poliomyelitis is one of the most common (for talipes deformities see Chapter 13). Occasionally it may result from ischaemic contracture of the calf muscles.
Guide to Painful Conditions Around the Ankle
| History of recent injury | Sprain of lateral ligament |
| Complete tear of lateral ligament | |
| (Ankle fracture, fracture of the fifth metatarsal base) | |
| Tibiofibular diastasis | |
| Ruptured Achilles tendon (tendo calcaneus) | |
| History of past injury | Complete tear of lateral ligament |
| Secondary osteoarthritis (e.g. previous ankle fracture) | |
| No history of injury | Osteochondritis tali |
| Rheumatoid arthritis | |
| Primary osteoarthritis | |
| Footballer’s ankle | |
| Secondary osteoarthritis (e.g. from osteochondritis tali) | |
| Tenosynovitis | |
| Achilles tendinopathy | |
| Snapping peroneal tendons |
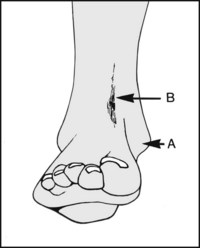
Look for (A) deformity of shape, suggesting recent or old fracture; (B) sinus scars, suggesting old infection, particularly tuberculosis.
Look for deformity of posture (e.g. plantarflexion owing to short tendo calcaneus, talipes deformity, ruptured tendo calcaneus or drop foot).
Look for bruising, swelling or oedema. If there is any swelling, note whether it is diffuse or localised. Note also whether oedema is bilateral, suggesting a systemic rather than a local cause.
When there is tenderness localised over the malleoli following injury, radiographic examination is necessary to exclude fracture.

After inversion sprains, tenderness is often diffuse. Swelling to begin with lies in the line of the fasciculi of the lateral ligament.
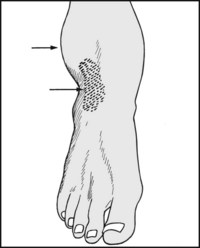
12.6. Lateral ligament (1): complete lateral ligament tear:
Swelling is rapid, and if seen within 2 hours of injury is eggshaped and placed over the lateral malleolus (McKenzie’s sign).

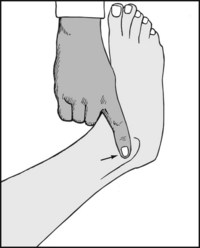
12.7. Lateral ligament (2): stress testing for complete lateral ligament tears (1):
Grasp the heel and forcibly invert the foot, feeling for any opening-up of the lateral side of the ankle between the tibia and the talus.

12.8. Lateral ligament (3): stress testing for complete lateral ligament tears (2):
If in doubt, have a radiograph taken while the foot is forcibly inverted.
12.9. Lateral ligament (4): stress testing for complete lateral ligament tears (3):
If tilting of the talus in the ankle mortice is demonstrated, repeat the examination on the other side and compare the films.
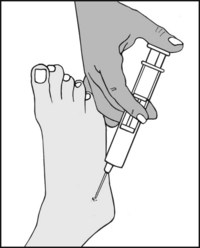
12.10. Lateral ligament (5): stress testing for complete lateral ligament tears (4):
If the injury is fresh and painful, the examination may be more readily permitted after the injection of 15–20 mL of 0.5% lidocaine widely in the region of the lateral ligament.
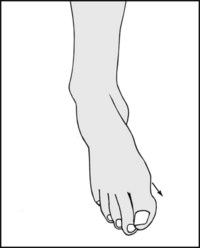
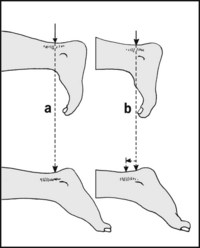
12.11. Lateral ligament (6): stress testing of the anterior talofibular component of the lateral ligament (1):
Instability may sometimes follow tears of the anterior talofibular portion only of the lateral ligament. With the patient prone, press downwards on the heel, looking for anterior displacement of the talus, which is often accompanied by dimpling of the skin on either side of the tendo calcaneus.
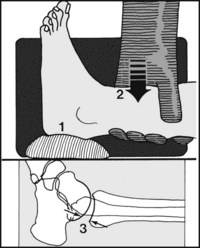
12.12. Lateral ligament (6): Stress testing of the anterior tibiofibular ligament (2):
Anterior displacement may be confirmed by radiographs taken in the prone position; alternatively, with the patient supine (and preferably with local anaesthesia), support the heel on a sandbag (1) and press firmly downwards on the tibia (2) for 30 seconds up to exposure. A gap on the radiograph between the talus and tibia of more than 6 mm is regarded as pathological (3).

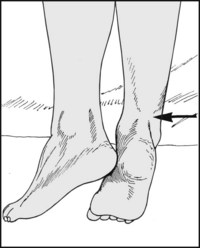
12.13. Inferior tibiofibular ligament (1):
In tears of this ligament (which has anterior and posterior components) tenderness is present over the ligament just above the line of the ankle joint.

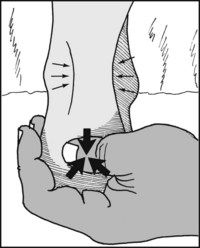
12.14. Inferior tibiofibular ligament (2):
In tears of the inferior tibiofibular ligament pain is produced by dorsiflexion of the foot, which displaces the fibula laterally.

12.15. Inferior tibiofibular ligament (3):
Grasp the heel and try to move the talus directly laterally in the ankle mortice. Lateral displacement indicates a tear of the ligament.

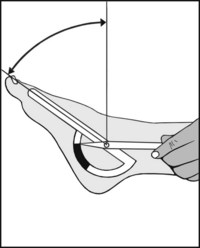
12.16. Ankle joint movements (1):
First confirm that the ankle is mobile, and that any apparent movement is not arising in the midtarsal or more distal joints. Firmly grasp the foot proximal to the midtarsal joint; try to produce dorsiflexion and plantarflexion.
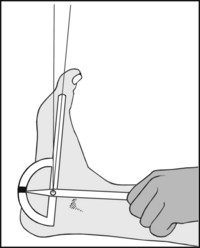
12.17. Ankle joint movements (2):
Measure plantarflexion from the zero position. This reference lies at right angles to the line of the leg.

12.19. Ankle joint movements (4):
If dorsiflexion is restricted, bend the knee. If this restores a normal range, the Achilles tendon is tight. If it makes no difference, joint pathology (such as osteoarthritis, rheumatoid arthritis or infection) is the likely cause.

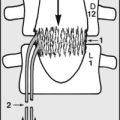
12.20. Ankle joint movements (5):
If there is loss of active dorsiflexion (drop foot) a full neurological examination is required. The commonest causes are stroke, old poliomyelitis, prolapsed lumbar intervertebral discs, and local lesions of the common peroneal (lateral popliteal) nerve.
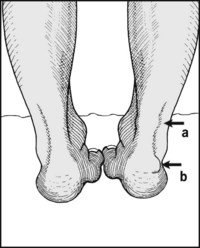
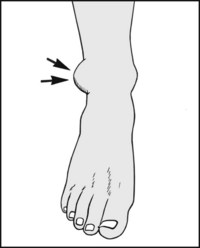
12.21. Tendo calcaneus (Achilles tendon): suspected tendinopathy (1):
The patient should be prone, with the feet over the edge of the couch. Inspect and compare the sides. Note any local (a) or diffuse swelling, redness of the skin, or the presence of a Hagland deformity (b): this is an exostosis affecting the posterosuperior aspect of the heel on its lateral aspect. It is commonly associated with an Achilles insertional tendinitis, although it does not directly involve the tendon.
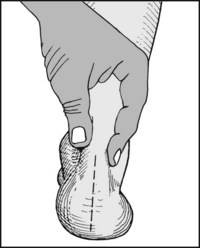
12.22. Suspected tendinopathy (2):
Now look for tenderness, which in the case of a tendinopathy is normally situated 3–5 cm proximal to the tendon insertion. Check for any increase in local heat. Palpate the tendon, noting any localised or fusiform swelling, and any nodularity. Gently squeeze the tendon (illus.); marked pain is a feature of tendinosis with an associated paratendinitis.
12.23. Suspected tendinopathy (3):
If tenderness is found, note whether the site of maximum tenderness changes with dorsiflexion and plantarflexion of the foot. If the pain is secondary to paratendinitis the site of maximum tenderness will remain fixed (a). If it is due to tendinosus alone, it will move with the tendon (b). Note also any weakness of plantarflexion.
12.24. Suspected tendon rupture (1):
Again the patient should be examined with the feet over the end of the couch. Defects in the contour of the tendon may be obvious.

Test the power of plantarflexion by asking the patient to press the foot against your hand. Compare one side with the other, and note the shape of each contracting calf and the prominence of each tendon.

Palpate the tendon while the patient continues resisted plantarflexion. Compare the sides. Any gap in the tendon (ruptured tendo calcaneus) should be obvious. The integrity of the tendon may also be tested by inserting a needle vertically into the middle of the calf. Normally the needle should tilt when the ankle is passively dorsiflexed and plantarflexed.

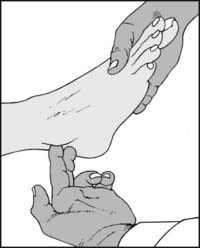
12.27. Tendo calcaneus (4): Thomson test:
Normally when the calf is squeezed the foot moves as the ankle plantarflexes. Loss of this movement is pathognomonic of an acute rupture of the tendo calcaneus.

12.28. Tenosynovitis (1): medial (1):
Look for tenderness along the line of the long flexor tendons. Tenderness is usually diffuse and linear in pattern. Note the site and extent of any local thickening.

12.29. Tenosynovitis (2): medial (2):
Look for synovitis in relation to the flexor tendons. There may be obvious swelling. Demonstrate the presence of any excess synovial fluid by milking the tendon sheaths in a proximal direction.

12.30. Tenosynovitis (3): medial (3):
Plantarflex and evert the foot. This may produce pain where tenosynovitis involves the tendon of tibialis posterior.

12.31. Tenosynovitis (4): medial (4):
With the foot held in the plantarflexed and everted position, look for tenderness or gaps in the line of the tendon of tibialis posterior. Spontaneous rupture is seen most frequently in association with flat foot and rheumatoid arthritis.

12.32. Tenosynovitis (5): lateral (1):
Examine the peroneal tendons for tenderness and the presence of excess synovial fluid in their sheaths.

12.33. Tenosynovitis (6): lateral (2):
Force the foot into plantarflexion and inversion. This will give rise to pain and increased tenderness along the line of the peroneal tendons if tenosynovitis of the peroneal tendons is present.

12.34. Tenosynovitis (7): lateral (3):
Feel for crepitus along the line of the tendon sheaths behind both malleoli as the foot is swung backwards and forwards between inversion and eversion. Confirm by auscultation.
Lightly palpate the peroneal tendons with the fingers; look and feel for displacement of the tendons as the patient everts the foot against light resistance. Displacement occurs in the condition known as ‘snapping peroneal tendons’.

12.36. Articular surfaces (1):
Forcibly plantarflex the foot to allow palpation of the anterior part of the superior articular surface of the talus. Tenderness occurs in arthritic conditions, and in osteochondritis of the talus. A tender exostosis may be palpable in cases of footballer’s ankle.

12.37. Articular surfaces (2):
Place a hand across the front of the ankle and passively dorsiflex and plantarflex the foot. Crepitus, which may be confirmed by auscultation, suggests articular surface damage.


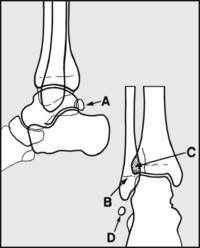
In the standard AP and lateral projections do not mistake (A) the common os trigonum accessory bone and (B) the epiphyseal line of the fibula for fractures. The amount of tibiofibular overlap (C) is dependent on positioning and any diastasis. The os fibulare (D) is thought to represent an avulsion of the anterior talofibular ligament, and may be associated with instability.
The articular margins of tibia and talus should appear as two congruent circular arcs. If there is some difficulty in positioning that cannot be improved upon, four arcs will be seen. Two pairs should be congruent, as shown. If not, there is a subluxation.
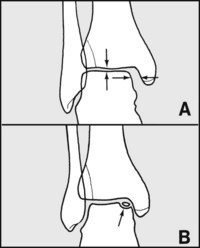
Note any widening of the gap (A) between talus and medial malleolus: this is suggestive of diastasis (compare its size with the one between the upper surface of talus and the tibia: they should normally be equal). (B) Note the presence of any defects in the articular surface of the talus, suggestive of osteochondritis tali. CT and MRI scans may help in the doubtful case.
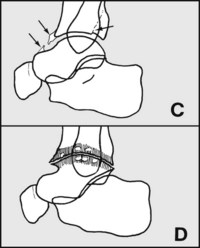
(C) Note any irregularity in the joint surfaces that may suggest previous fracture, e.g. of the posterior malleolus; note any anterior exostoses of the tibia (and/or the talus), which are a feature of footballer’s ankle. (D) Examine the articular margins for exostoses, joint space narrowing and cystic change, which are common features of osteoarthritis. If these are present, look for a possible cause (such as osteochondritis dissecans), as primary osteoarthritis of the ankle is uncommon.
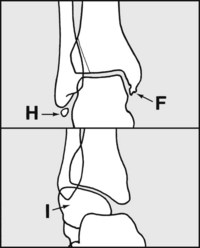
Look at the malleoli, where deformity (F) or rounded shadows (H) suggest previous avulsion injuries. Distortion of the talus occurs in association with talipes deformities (I) and after injuries which have resulted in avascular necrosis, and where there may be increases in bone density.

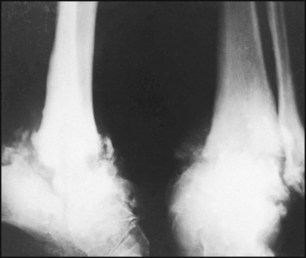
12.45. Radiographs of the ankle: examples of pathology (1):
The upper articular surface of the talus is distorted on its medial side.
Diagnosis: the appearances are typical of osteochondritis dissecans. More complete assessment of the defect may be obtained by a CT or MRI scan.

This inversion film shows tilting of the talus in the ankle mortice. There was no tilting elicited in comparison films of the other side.
Diagnosis: unilateral complete tear of the lateral ligament.

There is a large defect in the talus, which also shows increased density inferiorly.
Diagnosis: tuberculosis of the ankle with gross involvement of the talus.

There is gross decalcification of the ankle following a minor fracture in the foot. The ankle was stiff and painful, and there was marked swelling of the foot and leg below the knee.
Diagnosis: Sudeck’s atrophy (post-traumatic osteodystrophy, complex regional pain syndrome).
The radiographs show gross disorganisation of the ankle.
Diagnosis: Neuropathic ankle joint (Charcot’s disease). In this case the pathology was syphilitic in origin.

The talus is grossly misshapen and its upper articular surface flattened; clinically this was associated with pain, swelling and stiffness of the ankle and foot. There was a history of a severe injury to the ankle and foot a year previously.
Diagnosis: compression failure of the talus from avascular necrosis, with secondary osteoarthritic change. This occurred as a sequel to a dislocation of the talus, in spite of a good reduction.

There is narrowing of the joint space and the rounding of the upper articular surface of the talus (known as a so-called ‘ball and socket’ ankle joint).
Diagnosis: osteoarthritis of the ankle. This was secondary to fracture, although all traces of this in the AP projection have disappeared.

The bones of the ankle and foot show evidence of disuse osteoporosis, having a ground-glass appearance outlined with narrow, dense cortical margins. The ankle joint space is absent, and there is bony continuity between the talus and the tibia.
Diagnosis: bony ankylosis of the ankle following a chronic joint infection (TB).