CHAPTER 8 The thoracic and lumbar spine
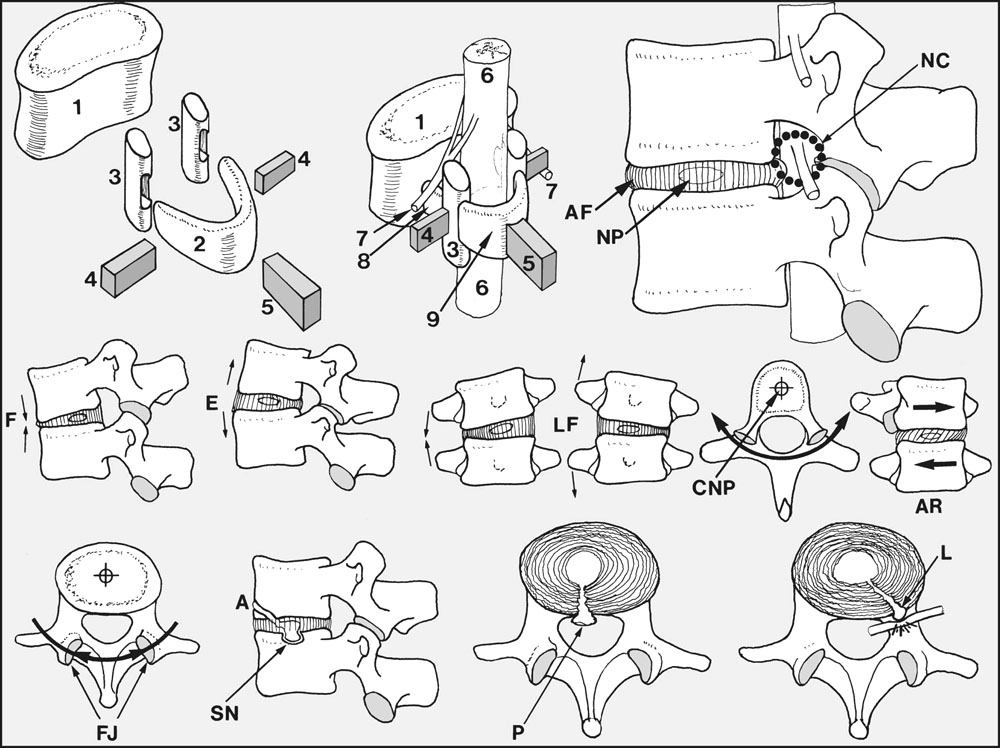
Fig. 8.A
The Spine: Anatomical Features
The complex relationships of the components of a typical vertebra may be illustrated by an exploded diagram (shown here after Kapandji). The bony elements comprise the vertebral body (1), composed of cancellous bone covered with an outer shell of cortical bone; the horseshoe-shaped neural arch (2); two articular masses or processes (3) which take part in the facet (interarticular) joints; the transverse processes (4); and the spinous processes (5). When these components are brought together they form a protective covering for the cord (6) and issuing nerve roots (7). The neural arch (2) is divided by the articular processes (3) into pedicles (8) and laminae (9).
Each vertebra articulates with the one above and below by means of the facet joints and the intervertebral discs. Each disc, lying between the hyaline cartilage endplates of adjacent vertebral bodies, is composed of a nucleus pulposus (NP) surrounded by concentric sheets of fibrous tissue (annulus fibrosis) (AF).
Movements between the vertebrae are possible in several planes, and the axes of these movements pass through the approximate centres of the intervertebral discs. At all levels of the spine, flexion (F) and extension (E), and lateral flexion (LF) to both sides are possible. In the thoracic spine, the plane of the facet joints lies in the arc of a circle which has its centre in the nucleus pulposus (CNP); as a result, (axial) rotation (AR) is possible in this part of the spine. In contrast, the orientation of the facet joints (FJ) in the lumbar region is such that rotation is blocked, i.e. virtually no vertebral rotation occurs in the lumbar spine.
As a result of the elasticity of the annulus the nucleus pulposus is under constant pressure, and may (uncommonly) herniate into a vertebral body anteriorly (A), or centrally (Schmorl’s node) (SN). A much more common occurrence is for the annular fibres to tear (as a result of trauma or degenerative changes) so that the nucleus can bulge posteriorly (P) or laterally (L): (’slipped discs’ – central or lateral protrusions). A posterior (central) disc protrusion may affect the cord directly (or the cauda equina in the lower lumbar spine); this may lead to bilateral lower limb signs with or without bladder involvement. With lateral protrusions the neurological disturbance usually results from pressure on one or two nerve roots only, so that the effects are more localised and usually predominate on one side. In the neural canals (NC, circled, top right) the space for the segmental nerves is restricted, and in this region symptoms may be caused not only by disc prolapse but by any other pathology compromising the space available (e.g. arthritic facet joint lipping).
Back Pain
Back pain is one of the commonest and most troublesome of complaints; its causes are legion and an exact diagnosis is often difficult. The disability with which it is usually associated is often severe and prolonged; therapy is often ineffective, and the anxious, impatient and dissatisfied sufferer often resorts to lines of treatment which are unproven, illogical and irrational. In this difficult area it is not possible to provide a guide to pathology and diagnosis which is simple and at the same time comprehensive and foolproof. Nevertheless, it may be helpful to consider this subject under three headings:
In taking a history, examining and investigating a patient suffering from back pain, possible extraspinal causes should be excluded and an attempt should be made to place the patient in one of the three groups described above. Thereafter, and if possible, a more precise diagnosis may be attempted.
Important points in history-taking:
Note that pain radiating into the legs is not necessarily due to nerve root involvement: it seems that irritation of facet joints, ligaments and muscles may produce dull, aching pain in the buttocks and backs of the thighs. In contrast, pain arising from nerve roots is usually sharp and knife-like, and in addition, in the case of the commonly affected L5 and S1 roots, it often extends below the knee to the ankle or foot. In the common situation where there is involvement of one, or at the most two, nerve roots, the whole limb cannot be affected; instead, the area of sensory disturbance should correspond with the relevant dermatome(s); and it should be noted whether paraesthesia occurs within the same restricted territory.
A positive answer to any of these questions will generally necessitate appropriate further investigation. The possibility of an invasive primary tumour or metastatic lesion must always be kept in mind, and examination of the abdomen, rectum, and common sites of primary tumour is wise if there is any likelihood of malignancy.
The spine should then be examined clinically; if the symptoms have remained unchanged over a 2-week period, radiological examination and estimation of the sedimentation rate should be carried out. At this stage any well defined spinal pathology should be detected (such as spondylolisthesis, ankylosing spondylitis, osteitis of the spine etc.). If conditions such as these have been eliminated, the question as to whether the symptoms are due to a prolapsed intervertebral disc should be considered. The history, clinical findings, and plain radiographs of the spine should be in harmony before it is reasonable to make this diagnosis. By the process of elimination, if a diagnosis has not yet been made the patient is likely to be suffering from mechanical back pain: but note that both the history and findings should be in accord with this. If not, caution must be exercised, close surveillance should be maintained, and further investigation may be indicated.
Scoliosis
Scoliosis is primarily a lateral curvature of the spine, but there is often a degree of associated kyphosis. Mathematical analysis of the curves has revealed several distinct patterns, which are dependent on the relative contributions of these two deformities.
In the management of any case, the first and most important decision to make is whether there is any deformity of the vertebrae (structural scoliosis). If the vertebrae are normal (non-structural scoliosis) the deformity is usually due to one of the following conditions: it may be compensatory, resulting from tilting of the pelvis from real or apparent shortening of one leg. It may be sciatic and due to unilateral protective muscle spasm, especially that accompanying a prolapsed intervertebral disc. Postural scoliosis occurs most commonly in adolescent girls and generally resolves spontaneously.
In structural scoliosis there is alteration in vertebral shape and mobility, and the deformity cannot be corrected by alteration of posture. A careful history and examination is required in an attempt to find a cause and give a prognosis, the two factors on which treatment depends. Structural scoliosis may be congenital, the deformity being due, for example, to a hemivertebra (only half of a single vertebra is fully formed), fused vertebrae, or absent or fused ribs.
In paralytic scoliosis the deformity is secondary to loss of the supportive action of the trunk and spinal muscles, nearly always as a sequel to anterior poliomyelitis.
Neuropathic scoliosis is seen as a complication of neurofibromatosis, cerebral palsy, spina bifida, syringomyelia, Friedreich’s ataxia and neuropathic conditions. Primary disorders of the supportive musculature of the spine are responsible for myopathic scoliosis (e.g. in muscular dystrophy, arthrogryphosis). Metabolic scoliosis is uncommon, but occurs in cystine storage disease, Marfan’s syndrome and rickets.
Idiopathic scoliosis is the commonest and by far the most important of the structural scolioses, and its cause remains obscure. Several vertebrae at one or, less commonly, two distinct levels are affected (primary curve). In the area of the primary curve there is loss of mobility (the fixed curve) and rotational deformity of the vertebrae (the spinous processes rotate into the concavity, and the bodies that carry the ribs in the thoracic region rotate into the convexity). Above and below the fixed primary curves, secondary curves which are mobile develop in an effort to maintain the normal position of the head and pelvis. The spinal deformity is accompanied by shortening of the trunk (which may be assessed by using anthropometric tables of normal values) and there is often impairment of respiratory and cardiac function. In severe cases this may lead to invalidism. Cor pulmonale may feature in cases where the primary curve exceeds 80°.
Once scoliosis has appeared in the growing child the natural tendency is towards deterioration. The prognosis of a given case is dependent on the age of onset, the level of the spine affected, the size and number of the primary curves, and the type of structural scoliosis (e.g. idiopathic or congenital). The maximal rate of deterioration tends to occur between the ages of 11 and 13 in girls, and 13 and 15 in boys, during the growth spurt that takes place around puberty. In assessing or observing any case it is usual to record the height, and the current stage of sexual and skeletal maturity. In many cases deterioration stops when skeletal maturity is reached, but sometimes continues as a result of disc degeneration and vertebral subluxation: 17° deterioration in 70° thoracic curves, and 20° deterioration in 30° lumbar curves have been recorded. Generally speaking, the higher the level of the spine involved in the primary curve, and the younger the patient, the worse the prognosis. There is the notable exception that in some cases occurring in infancy there is spontaneous recovery, which is as remarkable as its mysterious onset. Favourable factors are left-sided curves occurring in the first year of life in males where there is a rib–vertebral angle of less than 20°. Life expectancy may be reduced in congenital and paralytic scolioses, but not in idiopathic scoliosis.
In all cases of structural scoliosis appropriate investigation, radiographic measurement of the curves and careful observation is essential. Note in particular:
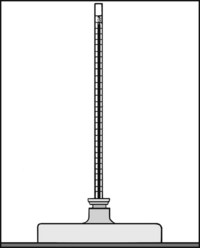
Treatment may be advised in the face of a poor prognosis, evidence of rapid deterioration, or for cosmetic purposes. (Curves are not usually considered for correction unless they are in excess of 25–30°.) The methods available are highly specialised, as is the decision regarding their use and timing. Deterioration in a curve may be controlled by use of the Milwaukee brace (a device incorporating moulded supports for the chin, occiput and pelvis, interconnected by vertical metal struts). This support is employed in older children approaching skeletal maturity who have just acceptable curves, or it may be used in the young child until an age suitable for spinal fusion (10 or over) is reached. Other patterns of support are available, although none has been shown to have statistical superiority (and some doubts have been recently cast on their overall effectiveness). Fusion of the entire primary curve is aimed at preventing further deterioration and at allowing braces to be discarded. Prior to fusion it is necessary to correct the primary deformity as much as is possible. Often a hinged plaster spica (Risser jacket) or the surgical insertion of internal apparatus (e.g. Harrington instrumentation) is employed.
Kyphosis
Kyphosis is the term used to describe an increased convexity of the thoracic spine. This is usually obvious when the patient is viewed from the side. (Diminution of the lumbar concave curve is referred to as loss of lumbar lordosis or flattening of the lumbar curvature; in extreme cases there is reversed lordosis, or posterior convexity of the lumbar curve.)
Kyphosis generally affects a major part of the thoracic spine (i.e. several vertebrae are affected), and the increased curvature is then said to be regular. In angular kyphosis, which must be carefully distinguished, there is an abrupt alteration in the thoracic curvature which is usually accompanied by undue prominence of a spinous process (gibbus).
Where mobility is normal in the kyphotic spine, the deformity is most frequently postural in origin; this is often seen (as is postural scoliosis) in adolescent girls. In some cases the deformity is secondary to an increased lumbar lordosis (which in turn may be due to abnormal forward tilting of the pelvis, and sometimes to flexion contracture of the hips or congenital dislocation of the hips). Less commonly, kyphosis may result from muscle weakness secondary to anterior poliomyelitis or muscular dystrophy.
When the thoracic curvature is not mobile but fixed, the most frequent causes are senile kyphosis, Scheuermann’s disease (spinal osteochondrosis), ankylosing spondylitis and Paget’s disease. When there is an angular kyphosis the most common causes are tuberculous or other infections of the spine, fracture (traumatic or pathological, e.g. secondary to osteoporosis), or tumours. In adults the commonest tumour is the metastatic deposit, and in children the eosinophilic granuloma.
Scheuermann’s Disease (Spinal Osteochondrosis)
This condition (whose exact aetiology is unknown, although there is a strong familial tendency), results in a growth disturbance of the thoracic vertebral bodies which in lateral radiographs of the spine are seen to be narrower anteriorly than posteriorly (anterior wedging). There may be associated back pain. The diagnostic protocol for the condition specifies that no fewer than three adjacent vertebrae should have at least 5° of anterior wedging. The epiphyses of the vertebral bodies are often irregular and may be disturbed by herniations of the nucleus pulposus. Nuclear herniation may occur between the epiphyses and bodies anteriorly, or into the centre of the bodies (Schmorl’s nodes), thought to be due to ischaemic necrosis of the cartilaginous end-plates. Mobility is impaired, thoracic kyphosis is regular and often quite marked, and there is a compensatory increase in lumbar lordosis. Secondary osteoarthritic changes may supervene in the thoracic and lumbar spine.
The normal upper limit of the convexity of the thoracic spine (as measured by the Cobb method) is reckoned to be 45°, and cases of Scheuermann’s disease in adolescence with curves of 50° or less should be observed. Where the curve is in excess of this, a Milwaukee brace, worn continuously for not less than 12–18 months (and afterwards till skeletal maturity) may be advised in an attempt to prevent deterioration. (Some question the efficacy of this method of spinal bracing.) If the curve cannot be controlled and reaches 75°, correction by surgical instrumentation should be considered. In the adult with uncontrollable pain and a curve in excess of 60°, surgical fusion may be performed.
Calvé’s Disease
Back pain in children may be accompanied by gross flattening of a single vertebral body. Symptoms usually resolve spontaneously. In many cases the pathology is due to an eosinophilic granuloma.
Ankylosing Spondylitis
In this chronic inflammatory disease there is progressive ossification of the joints of the spine; its aetiology is unknown but there is a hereditary tendency, with the overall risks of children of an affected parent developing the condition being 1 in 6. Unlike rheumatoid arthritis, to which it is often related, it is comparatively rare in women. The male/female ratio varies from 6 : 1 to 2 : 1, depending on the age of onset. The commonest presentation is that of a male during the third and fourth decades.
The joints between T12 and L1 are often first affected, but the rest of the thoracic and lumbar spine is rapidly involved. The costovertebral joints are usually affected, leading to a reduction in chest expansion and vital capacity. Pulmonary tuberculosis, or pulmonary infections with Aspergillus are sometimes found in association, and there may be cardiovascular, renal, gastrointestinal and ocular complications.
Stiffness of the back and pain are the presenting symptoms in the majority of cases, but on occasion involvement of the hip joints, or the knees with effusions, may first attract attention. There may be pain at the insertions of the Achilles tendons or the plantar fascia (enthesopathy). Stiffness is usually worse in the mornings, and may wake the patient from sleep; it tends to improve with activity as the day wears on.
The disease is progressive, and although it sometimes arrests spontaneously at an early stage it usually leads to complete ankylosis of the spine, with characteristic changes in the radiographs (bambooing of the spine). Progressive flexion of the spine may be severe, so that forward vision becomes impossible as the head is flexed on to the chest. The sacroiliac joints are almost invariably involved at an early stage, and there may be fusion of the manubriosternal joint. There may be a history of iritis or its sequelae. The sedimentation rate is high (40–120 mm/h), rheumatoid factor is not present, and estimations of human leucocyte antigen-B27 (HLA-B27) are usually positive. There is often associated anaemia, muscle wasting and weight loss.
As far as treatment is concerned, exercise and physiotherapy are generally regarded as being beneficial. Non-steroidal anti-inflammatory drugs (NSAIDs) are usually helpful, although the risks of cardiovascular toxicity with long term use must be considered. Disease-modifying anti-rheumatic drugs (DMARDs) have not been found to be particularly useful. Deep X-ray therapy is often effective, but carries the risk of aplastic anaemia. Remarkable improvements in disease activity, mobility, function and pain have followed the use of anti-tumour necrosis factor (TNFα) in the form of infliximab or etanercept.
Where deformity of the spine is gross, spinal osteotomy is occasionally undertaken to give the patient a tolerably erect posture. Replacement arthroplasty of the hips or knees is often carried out, even if these joints have progressed to fusion.
Diffuse Idiopathic Skeletal Hyperostosis (Dish)
This comparatively benign condition, also known as Forestier’s disease, is sometimes mistaken for ankylosing spondylitis. It is characterised and diagnosed by the presence of flowing calcification and ossification along the anterolateral borders of at least four contiguous vertebral bodies. The disc spaces are, however, preserved (unlike in ankylosing spondylitis), without loss of height or other degenerative changes, and the sacroiliac and the facet joints do not ankylose. Most cases are asymptomatic, or have mild or moderate restriction of movements in the parts of the spine affected. No treatment is effective.
Senile Kyphosis
In true senile kyphosis the ageing patient becomes progressively stooped and shorter in stature through degenerative thinning of the intervertebral discs. Pain may occur if there is associated osteoarthritis.
In elderly women the kyphosis may be aggravated by senile osteoporosis or osteomalacia, which lead to anterior vertebral wedging and often pathological fractures. There is usually radiographic evidence of decalcification, the serum chemistry may be disturbed, and pain is a feature if there are recent vertebral body fractures.
Treatment is directed towards controlling the underlying osteoporosis or osteomalacia. Thoracic spinal supports are not particularly effective and cannot be tolerated by the elderly, but often a simple lumbar corset is helpful in relieving pain arising from the secondary increase in lumbar lordosis.
Paget’s Disease
Paget’s disease of the spine is comparatively uncommon, and although the diagnosis is made on the radiographic findings, it may be suggested clinically by other stigmata of the disease. Paget’s disease may lead to disturbance of cord function, which may often be successfully treated with bisphosphonates (e.g. etidronate and pamidronate).
Tuberculosis of the Spine
Bone and joint tuberculosis is uncommon in Britain, but the incidence is increasing. The factors responsible include the increase in numbers of immunosuppressed individuals, the development of drug-resistant strains of Mycobacterium tuberculosis, and an ageing population. HIV is the leading risk factor for the reactivation of latent tuberculous infections. The World Health Organization reckons that a third of the global population is infected with the organism, and that it is the commonest cause of death and disability on a worldwide basis. About a fifth of newly diagnosed cases are extrapulmonary, and the spine is involved in 50% of cases of bone and joint tuberculosis.
The onset of spinal tuberculosis is often slow, with aching pain in the back and stiffness of the spine. There may be fever and weight loss. Radiographs taken in the earliest stages of the disease show narrowing of a single disc space; later, as the anterior portions of the vertebral bodies become progressively involved, they collapse, leading to anterior and sometimes lateral wedging of the spine. This may produce angular kyphotic or scoliotic deformities. The local abscess may expand and track distally.
The spinal cord may be compromised extrinsically or intrinsically, and weakness of the limbs or paraplegia may ensue. Extrinsic causes include caseous abscesses, granulation tissue and fluid, sequestered bone or disc material, and spinal angulation leading to kinking of the cord over an internal gibbus. Intrinsic causes include the spread of tuberculous inflammation through the cord and meninges.
Initial investigation should include radiographs of the chest, culture of urine and any sputum, Mantoux testing, brucellosis complement fixation testing and, in the case of the lumbar spine at least, an intravenous pyelogram (IVP) (renal spread being not uncommon). CT and MRI scans of the spine are also invaluable in demonstrating the extent of bone and soft tissue involvement.
The clinical and radiological features of tuberculosis of the spine are mimicked in the early stages by other infections (especially those due to Staphylococcus aureus), and the only certain method of establishing the diagnosis in the majority of cases seen at this stage is by obtaining specimens for histological and bacteriological examination. CT-guided needle aspiration biopsy may be employed if this facility is available. Again, as the abscess is small at first and the early removal of necrotic bone and pus is generally of value from the point of view of accelerating healing, many surgeons combine these procedures. In the later stages, where there is gross bone destruction, minimal new bone formation and the formation of large abscesses, the diagnosis is seldom in doubt.
The aim of treatment is to overcome the infection, eliminate abscesses and sequestra, and promote sound fusion in the affected spinal segment to prevent any recrudescence. The mainstay of treatment is the use of the antituberculous drugs, although the emergence of resistant strains is causing problems. Sensitivity testing is advisable, and drugs should not be used in isolation. Drug therapy for periods up to 2 years was formerly advised, but it has been shown that regimens employing a combination of rifampicin and isoniazid for 6 months only seem equally effective. This is of particular importance where compliance is low. It has been noted that the addition of streptomycin to the drug regimen, bed rest, or a plaster cast do not seem to affect the outcome.
Conservative treatment alone leads to a comparatively low fusion rate, and in about 70% of adult cases there is a deterioration in the kyphosis. In those parts of the world where resources are good, there is at present a trend to early surgical intervention to achieve or accelerate the healing process and assist fusion by early drainage of abscesses and bone grafting. Where paraplegia is due to intrinsic causes, it may resolve following antituberculous therapy, but in many cases the causes are extrinsic, and surgery is indicated to decompress the cord. An MRI scan may give valuable assistance in selecting cases and delineating the scope of the surgery required. If adequately dealt with in the early stages (i.e. within 6–9 months of the onset of paraplegia) complete cure is often achieved. In paraplegia of late onset, where the cord is often acutely angled over an internal gibbus, surgical intervention should always be carried out, but the prognosis here is less good.
Pyogenic Osteitis of the Spine
Pyogenic osteitis of the spine is relatively uncommon. In the early stages of the disease differentiation from tuberculosis of the spine is often extremely difficult, so that the diagnosis may not be clearly established unless material is provided for bacteriological examination. Specimens may be obtained by needle biopsy with the use of an image intensifier, or by exploration. At a later stage (and many cases may delay in their presentation) exuberant new bone formation in the region of the lesion may favour this diagnosis. The presenting features are of pain and stiffness in the back, often insidious in onset, but sometimes occurring quite rapidly. Nearly all cases resolve with prolonged treatment with the appropriate antibiotic (the majority are due to a staphylococcal infection, but Salmonella typhi (syn. Bacillus typhosus) and other organisms are sometimes causal).
Metastatic Lesions of the Spine
Metastatic disease of the spine is seen particularly in the elderly and may be complicated by paraplegia. Back pain at night, pain unaffected by rest or activity, fatigue and weight loss are common features. The diagnosis is made on the radiographic findings. Treatment of the uncomplicated lesion is dependent on the nature of the primary tumour; in some cases deep X-ray therapy and supportive measures may help the local lesion and give relief of pain. Where paraplegia is present, decompression should be undertaken unless the case is terminal. In the patient with some pre-existing cardiovascular disease the possibility of an abdominal aneurysm should be considered; or if the pain is severe at night and there is weight loss, a further search for evidence of malignancy should be made. Primary tumours of the spine are rare; the common types are mentioned in Chapter 3.
Spondylolysis, Spondylolisthesis
In the erect position there is a tendency for the body of the fifth lumbar vertebra (carrying the weight of the trunk) to slide forwards on the corresponding surface of the sacrum, as the plane of the L5–S1 disc is not horizontal but slopes downwards anteriorly. This movement is usually prevented by the downward-projecting inferior articular processes of the fifth lumbar vertebra impinging on the corresponding upward-projecting articular processes of the sacrum. This mechanism may fail if there is a fracture or defect in the part of the fifth lumbar vertebra lying immediately anterior to its inferior articular process. A defect in this region, if unaccompanied by any significant forward movement of the vertebral body, is known as spondylolysis. The defect may be unilateral or bilateral. When forward slip occurs, the condition is known as spondylolisthesis. Less commonly, the fourth lumbar vertebra may be involved, the slip occurring between L4 and L5.
Both congenital and developmental factors have been recognised in the causation of the condition. There is a higher incidence in the families of those affected (30–70%, with dominant transmission), in certain Inuit tribes (where it reaches 54%), and among the Japanese. The lowest incidence is in black females (1.1%), and in white males it is 6.1%. Defects are rare at birth and before the age of 5, but the incidence in the population goes on increasing up to the end of the fourth decade. Fractures due to trauma or fatigue are thought to be the most likely cause, and this explains the high incidence amongst gymnasts, weightlifters, labourers, loggers and backpackers. It may be associated with sacral spina bifida and Scheuermann’s disease.
Both spondylolysis and spondylolisthesis give rise to low back pain which radiates into the buttocks. In adolescents, the majority of whom are active in sports, resolution of symptoms may be achieved in 80% of cases by the avoidance of sports and the use of a corset support. This may lead to the healing of hairline fractures, or to the spine stabilising as a result of degenerative changes occurring at the level of the slip. In more severe cases, where there is significant forward slip, local spinal fusion is the treatment of choice. This may be performed with or without reduction of the deformity.
A number of patients may suffer from neurological disturbances in the lower limbs, either initially or as an uncommon complication of a local fusion. In the cauda equina syndrome there is usually low back pain with radiation into the buttocks, spinal stiffness, hamstring spasm, gait abnormalities, and disturbance of bladder and bowel control. This may be due to an associated disc protrusion, or be caused by the cauda equina and roots of the lumbosacral plexus being stretched over the prominent upper edge of the fifth lumbar vertebra or the sacrum. These complications should be dealt with by an immediate decompression procedure.
Osteoarthritis (Osteoarthrosis)
Primary osteoarthritis of the spine is extremely common, especially in the elderly, and is often asymptomatic. In the majority of cases there are no obvious causes, apart from those associated with the degenerative processes of age. Sometimes obesity and excessive use of the spine by manual workers may be factors. In secondary osteoarthritis, previous pathology in the spine accelerates normal wear and tear processes.
Occasionally osteoarthritis may be localised to one spinal level, at for example the site of a previous fracture or a prolapsed intervertebral disc. Often, however, many vertebral levels are affected, particularly where there is some alteration in the normal curves of the spine; for example, secondary osteoarthritic changes may occur in the lumbar spine when lumbar lordosis is increased as a sequel to Scheuermann’s disease of the thoracic spine.
Osteoarthritis of the spine may be accompanied by disc degeneration, anterior and posterior lipping of the vertebral bodies, narrowing and lipping of the facet joints, and sometimes abutment of the vertebral spines (kissing spines) as a result of disc degeneration bringing the vertebrae nearer together.
When osteoarthritis gives rise to symptoms, these are usually of pain and stiffness in the back; once other conditions have been eliminated, the radiological appearances are diagnostic. Treatment is by weight reduction where applicable, spinal exercises to improve the back musculature, and analgesics. Short-wave diathermy is sometimes helpful. In the commonest area, the lumbar spine, a corset support is a widely used and generally very helpful line of treatment. Only rarely is spinal fusion indicated, but this is sometimes considered in the younger patient suffering from secondary osteoarthritis localised to a single level of the spine.
Rheumatoid Arthritis
Rheumatoid arthritis may affect the spine; other peripheral sites are normally involved, so that the diagnosis is not normally difficult. Radiographs of the spine in rheumatoid arthritis generally show widespread osteoporosis, disc space narrowing, narrowing of the facet joints, and often reduction in the height of vertebral bodies. The treatment is that of generalised rheumatoid arthritis; locally, corset supports may give considerable relief of symptoms.
Spina Bifida
Spina bifida is a condition in which there is a congenital failure of fusion of the posterior elements of the spine, through which the contents of the spinal canal may herniate. The grosser forms in the newly born child present no difficulty in diagnosis. A number require and are amenable to immediate surgery, which may prevent early death from ascending meningitis and ameliorate the frequently concomitant neurological and hydrocephalic problems. The residual neurological defect may unfortunately be profound, and the selection of cases for surgery is specialised and to some extent controversial.
The older child or adult may present with spina bifida occulta, which is diagnosed by radiological examination, although it may be suspected by the presence of a hairy patch, naevus or fat pad, or dimpling of the skin at the site of the abnormality. Many cases are symptom free. In some the only manifestation may be the presence of pes cavus. In others there may be progressive bladder dysfunction, weakness and incoordination of the legs, or trophic changes in the feet.
Spinal Stenosis
In spinal stenosis there is a decrease in the sagittal diameter of the spinal canal which may cause compression of the cauda equina and associated nerve roots. There may be some narrowing of the nerve root tunnels.
Spinal stenosis may be congenital or acquired. Congenital spinal stenosis is common in achondroplasia or other short stature syndromes. Acquired spinal stenosis is seen most often as a result of degenerative changes in the spine. In women, the mean age of onset is 73; in men it usually appears earlier. Contributory factors include osteoarthritis of the lumbar spine, spondylolisthesis, Paget’s disease, previous fracture or spinal surgery.
The condition may give rise to vague backache and morning stiffness, relieved by rest and aggravated by activity. Occasionally there may be temporary motor paralysis or neurogenic claudication, where there are lower limb pains, cramps and paraesthesiae related to walking or exercise. There may be weakness or giving way of the legs. The claudication distance is variable, and pain may be rapidly relieved by forward flexion of the spine or by sitting. The patient may have no difficulty in cycling, or walking while leaning on a shopping trolley, where in both activities the spine is in a flexed postion; but he may be unable to tolerate walking upright. The sensory loss is segmental, and impulse symptoms are usually present. Clinically the straight leg-raising test is hardly ever affected, but motor disturbances and absence of the knee jerk are common. The ankle jerk and the plantar response are unaffected, and there is no clonus; if an abnormality is found in this respect, another neurological disorder or an abnormality in the thoracic or cervical spine should be sought. Note also that in claudication due to vascular insufficiency the claudication distance is constant, the peripheral pulses are usually absent, and the sensory loss generally of the stocking type.
The condition may be suspected on clinical grounds. Analysis of the dimensions of the pedicles and the spinal canal in the plain radiographs may be helpful in establishing the diagnosis, but CT and MRI scans reliably demonstrate the space available within the spinal canal for the neurological structures.
Mild cases may be treated with analgesics, NSAIDS, physiotherapy and exercise (e.g. use of a stationary bicycle with the spine in flexion), temporary use of a lumbar corset support, and epidural injections of steroids. If symptoms are marked and the patient is otherwise fit, gratifying relief is often achieved by a decompression procedure.
The Prolapsed Intervertebral Disc (PID)
In the commonest pattern of intervertebral disc prolapse, a tear in the annulus allows protrusion of the semiliquid nucleus pulposus. This may be limited by intact fibres at the periphery of the annulus (contained prolapse). In other cases extrusion of the nucleus is usually more extensive and the prolapsed material may be cut off from its source (sequestered disc prolapse).
Lumbar disc prolapses are by far the most common, and the diagnosis is usually made on the clinical evidence alone. Confirmation may be obtained by means of non-invasive procedures such as CT and MRI scans.
Discography often yields valuable information, as does radiculography. Nevertheless, it is most important to note that the investigative findings must be interpreted in conjunction with the history and clinical findings. (In a recent study of a control group completely free from symptoms, abnormalities were found in the MRI scans in 57%: 36% had evidence of disc prolapse, and 21% had spinal stenosis. In addition, among proven cases of disc prolapse the MRI scan is negative in 20% of cases, or shows incompatible abnormalities in 30%.)
The disc between L5 and S1 is most commonly involved, followed in order by L4–L5, and that between L3 and L4. In a typical case there is a history of a flexion injury which tears the annulus fibrosus, allowing the nucleus pulposus to herniate through. Back pain is produced by the annular tear and protective lumbar muscle spasm may contribute to it. Pain is felt in the lumbar region. There is usually tenderness between the spines at the affected level, and sometimes at the side over muscles in spasm, although this is a somewhat unreliable and controversial sign. Muscle spasm often leads to loss of the normal lumbar lordotic curve, to restriction of movements in the lumbar spine, and a protective scoliosis. The extruding nucleus frequently presses on a lumbar nerve root, giving rise to sciatic pain, paraesthesiae in the leg, and sometimes muscle weakness, sensory impairment, and diminution or abolition of the ankle jerk. At higher levels the knee jerk may be lost. The neurological disturbance is segmental in pattern, and is dependent on the side and level of the prolapse. Impulse symptoms are common. When the prolapse is large and central the cauda equina may be affected, producing bladder disturbance, diminished perineal sensation, and even paraplegia. Such an occurrence is a surgical emergency and immediate exploration imperative.
When a disc prolapse occurs in the adolescent there is striking restriction of movements in the lumbar spine. In the older patient, where degenerative changes have occurred in the annulus, symptoms may be produced by an extensive backward bulging of the disc without there being a frank localised annular tear.
Disc prolapses in the thoracic spine are rare and have a variety of presentations, often with a confusing clinical picture. There may be bandlike chest pain, scoliosis, bizarre neurological disturbances with peripheral temperature changes, altered reflexes, and weakness of the limbs. A number are misdiagnosed as multiple sclerosis or amyotrophic lateral sclerosis. They may be diagnosed by MRI scan, and treated by transthoracic excision.
In the long term, the extrusion of disc material from between the vertebral bodies leads to narrowing of the disc space. The facet joints are disturbed, and tend to develop secondary arthritic changes which decrease the mobility of the spine at that level, and themselves be a source of pain and sometimes nerve root irritation.
Occasionally, in the young in particular, the nucleus may herniate into the substance of the vertebral bodies, giving rise to mild backache without root symptoms. This pattern of herniation (Schmorl’s nodes) is diagnosed radiographically.
Apart from the large central prolapse all cases of acute disc prolapse are first treated by conservative methods. The present view is that prolonged periods of bed rest should be avoided, but an initial 2-week period of bed rest with the use of strong analgesics may be required. If the response is good the patient is then allowed up, although he is warned to avoid lifting and bending in case of recurrence. In some centres spinal extension exercises may be advocated at this stage. If the response has only been moderate, a number of surgeons nevertheless allow the patient to become ambulant wearing a corset back support. If there is no response to 2 weeks’ bed rest, the case must be carefully reassessed before this treatment is continued.
Where ultimately there is an unsatisfactory response, or where residual symptoms are severe, further investigation by CT or MRI scan, discography or myelography is usually undertaken, with a view to specific treatment of the lesion. The methods available include surgical excision by means of a laminectomy, microsurgery, percutaneous endoscopic surgery, or by chemonucleosis. The results of treatment, particularly as far as return to work is concerned, are surprisingly little affected by either the physical findings, the extent of the local pathology or the effects of surgery. (Social or work-related factors have the greatest influence on the results.)
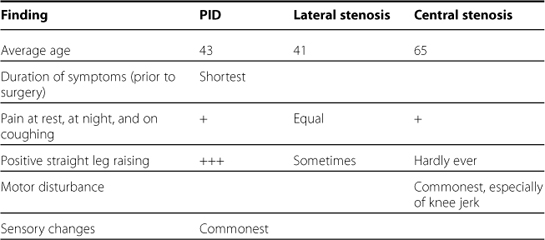
The following table (based on the findings of Jonson and Stomquist) may be helpful in differentiating between cases of disc prolapse and spinal stenosis.
Mechanical Back Pain
Although usually suspected following history taking, clinical examination and the study of appropriate radiographs, the diagnosis is made largely by a process of elimination: it is back pain which is not due to a prolapsed intervertebral disc or any other clearly defined pathology. The patient is usually in the 20–45-year age group, and complains of dull backache aggravated by activity. There is often a history of morning stiffness which is gradually relieved as the patient moves about. Physical signs are often slight, and extensive radiation of pain and positive neurological signs are not a feature.
Acute cases may be precipitated by a traumatic incident, such as the flawed lifting of a heavy weight, a fall, or a head-on impact pattern road traffic accident. There may be intense protective muscle spasm. As far as treatment is concerned, analgesics should be prescribed for a short period and prolonged bed rest should be avoided. An early return to work should be encouraged, even in the presence of some degree of residual pain. Physiotherapy should be started after a week if symptoms are still marked. In the majority of cases symptoms resolve completely over a 4–6-week period. In a number of cases, however, symptoms become prolonged, with the impatient sufferer often trying any of the large number of alternative medicine treatments now so widely available.
In chronic cases there is often a long history of intermittent low back pain over a number of years. The cause is often obscure, although degenerative changes in the spine are not uncommonly present. Resistance to treatment is a frequent problem, and many are ultimately referred to pain clinics. Sometimes a change of employment to work of a lighter character may have to be contemplated.
Coccydynia
In patients with this complaint of pain in the coccygeal area there is often a history of a fall in the seated position on to a hard surface; consequently, in a number of cases radiographs may reveal a fracture of the end piece of the sacrum, or show the coccyx to be subluxed into the anteverted position. Symptoms of pain on sitting and defecation are often protracted for 6–12 months, but tend to resolve spontaneously. It was formerly thought that if symptoms proved persistent either a disc lesion in the lumbar spine (with distal referral) or a functional problem was likely to be the problem, but this is now discounted.
In stubborn cases conservative treatment should invariably be first employed: 60% of cases respond to local injections of steroids, and 85% to the injection of a long-acting local anaesthetic followed by manipulation. If there is complete failure to respond to a substantial period of conservative treatment (this occurs in about 20% of cases), excision of the coccyx is reported as being successful in 80% of cases.
Commoner Causes of Back Complaints in the Various Age Groups
| Children |
Adolescents
Young adults
Middle-aged
Elderly
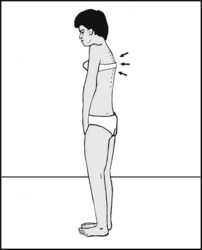
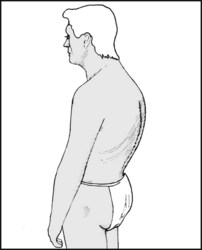
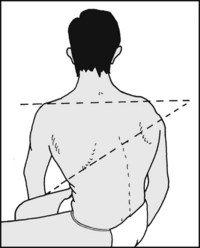
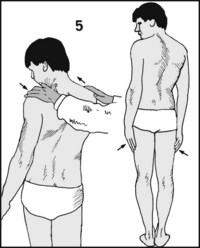
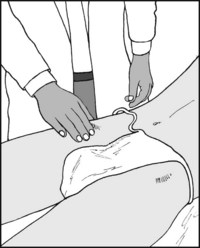
8.1. Inspection from the side (1):
Ask the patient to stand. Look at the spine from the side. Although normal posture is difficult to define, try to make an assessment of the thoracic curvature, noting whether the curve is quite regular and if it appears to be increased.

It is valuable to know whether the thoracic spine is mobile, especially if there is a kyphosis. Ask the patient to bend forward, carefully examining the flow of movement in the spine, and whether the curvature increases. As the range of flexion in the thoracic spine is small it may also help to check rotation, which is the main movement occurring in the thoracic spine (see later).

Now ask the patient to stand upright and brace back the shoulders to produce extension. An increased curvature (kyphosis) which is regular and mobile is found in postural kyphosis.
If a regular but fixed kyphosis is found, the commonest causes are senile kyphosis (sometimes with osteoporosis, osteomalacia or pathological fracture), Scheuermann’s disease and ankylosing spondylitis.
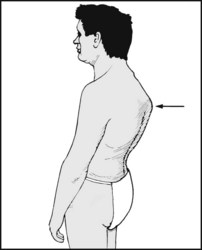
If there is an angular kyphosis, with a gibbus or prominent vertebral spine, the commonest causes are fracture (traumatic or pathological), tuberculosis of the spine, or a congenital vertebral abnormality.
Note the lumbar curvature. Flattening or reversal of the normal lumbar lordosis is a common finding in prolapsed intervertebral disc, osteoarthritis of the spine, infections of the vertebral bodies and ankylosing spondylitis. Flexion of the spine, hips and knees (simian stance) is suggestive of spinal stenosis.
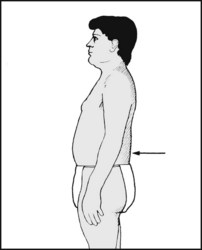
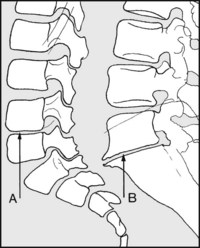
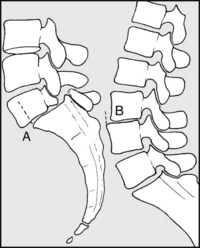
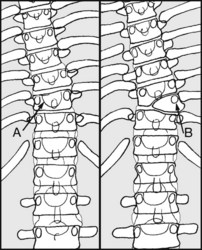
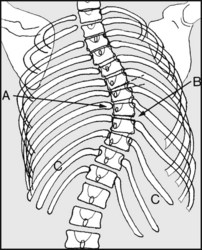
(A) An increase in the lumbar curvature may be normal (especially in women) or be found in association with the prominence of the spine of L5 and the sacrum (B) in spondylolisthesis. It may be secondary to an increased thoracic curvature, or to flexion deformity of the hip(s). Always screen test the hips.
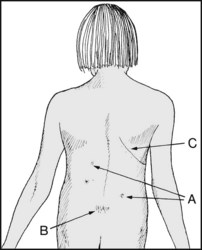
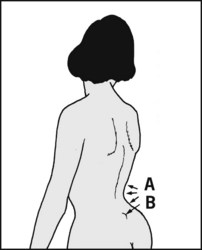
From behind: Note (A) café-au-lait spots, which may suggest neurofibromatosis and associated scoliosis; (B) a fat pad or hairy patch suggestive of spina bifida; (C) scarring suggestive of previous thoracotomy (and possible thoracogenic scoliosis) or spinal surgery.
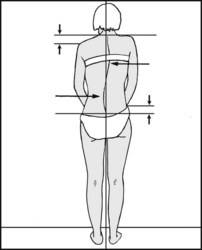
Note the presence of any lateral curvature (scoliosis). The commonest scoliosis is a protective scoliosis, or list, in the lumbar region secondary to a prolapsed intervertebral disc. Note whether the shoulders and hips are level.
In considering other causes of scoliosis, examine the spine with the patient sitting. Obliteration of an abnormal curve suggests that the scoliosis is mobile and may be secondary to shortening of a leg. Certainly the next step to take is to check and compare the leg lengths.
If, on sitting, the scoliosis persists, ask the patient to bend forward. If the curve disappears, this suggests that it is quite mobile and most likely to be postural in origin.
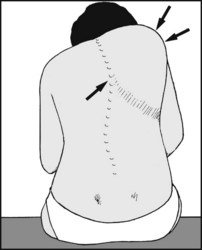
If the curvature remains, this suggests that the scoliosis is fixed (structural scoliosis). If a rib hump is present, this confirms the diagnosis. Note should be made of its severity. (Goniometers for measuring the angle of the hump are available.) Remember that syringomyelia is present in about a quarter of cases of juvenile idiopathic scoliosis, and an MRI scan is mandatory.
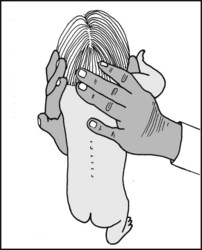
In the case of infantile scoliosis, assess the rigidity of a curvature by noting any alterations as the child is lifted by the armpits.
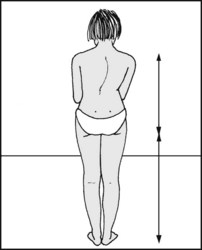
Note that in idiopathic scoliosis with double fixed (primary) curves the deformity may not be obvious. There will, however, be shortening of stature, with a trunk which is short in proportion to the limbs. (If desired, this may be assessed using the anthropometric tables of Aldegheri and Agostini, which give values for the ratio of sitting height to standing height in each sex at different ages.)
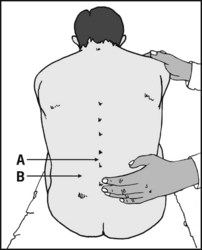
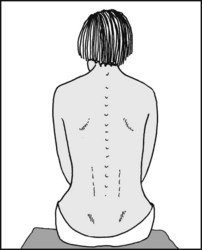
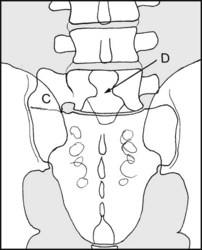
Ask the patient to lean forward if possible. Look for tenderness: (A), between the spines of the lumbar vertebrae and at the lumbosacral junction (common in prolapsed intervertebral disc, but thought difficult to explain and unreliable) and (B), over the lumbar muscles; this is especially likely to be found where there is protective muscle spasm in cases of PID and mechanical back pain.
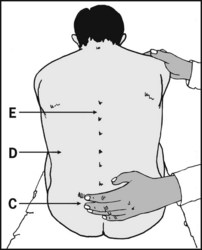
Tenderness over the sacroiliac joints (C) may also occur in cases of mechanical back pain and in sacroiliac joint infections. Re-examine with the patient prone. Renal tenderness (D) must be investigated fully. Look also for tenderness higher in the spine (E), e.g. from vertebral body infections.
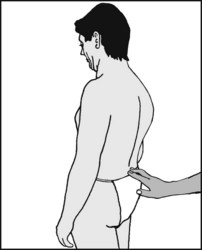
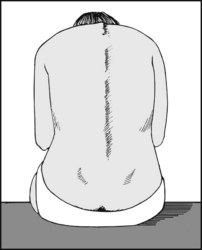
With the patient standing, slide the fingers down the lumbar spine on to the sacrum. A palpable step at the lumbosacral junction is a feature of spondylolisthesis. Note any other curve irregularity (e.g. gibbus). Note also any change in friction (due to alterations in sweating patterns), which may help in the localisation of any pathology.
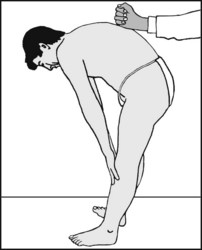
Ask the patient to bend forward. Lightly percuss the spine in an orderly progression from the root of the neck to the sacrum. Significant pain is a feature of tuberculous and other infections, trauma (especially fractures) and neoplasms. Otherwise a marked response may be a feature of a non-organically based complaint.
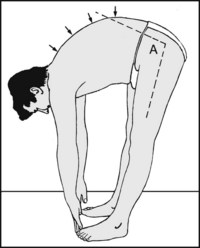
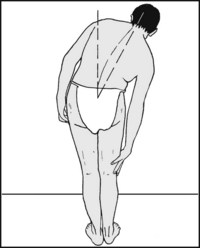
Ask the patient to attempt to touch his toes while you watch the spine closely for smoothness of movement and any areas of restriction. Note the importance of hip flexion (A), which can account for apparent motion in a rigid spine.
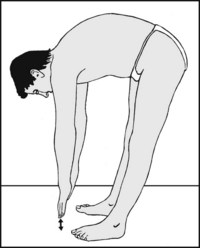
Flexion may be recorded in several ways, the commonest being to note the distance between the fingers and the ground, e.g. ‘the patient flexes to within 10 cm of the floor’. This is an indication of the summation of thoracic, lumbar and hip movements; it does not distinguish between them, and is under voluntary control.
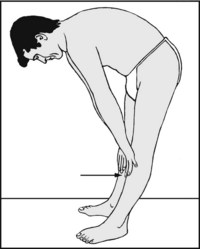
Flexion may also be recorded as: ‘the patient flexes so that the fingertips reach mid-tibia’, or some other appropriate level. The majority of normal patients can reach the floor or within 7 cm from it. (Actual maximum range flexion is approximately 45° thoracic, 60° lumbar.) Again, this does not indicate the relative contributions of the hips and spine.
When the spine flexes, the distance between each pair of vertebral spines increases. By measuring the spine when the patient is erect, and then when bent forward, any gain is clear evidence of spinal flexion. In practice this is used most frequently in assessing movements in the lumbar spine (where flexion is greatest and pathology more common).
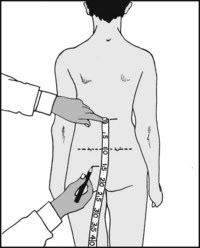
In Schober’s method a 10 cm length of lumbar spine is used as a base. Greater accuracy is claimed for the modified Schober’s method (most often used in the UK), where a 15 cm length of spine is employed. Begin by positioning a tape measure with the 10 cm mark level with the dimples of Venus (which mark the posterior superior iliac spines). Mark the skin at 0 and 15 cm.
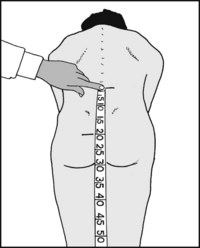
Anchor the top of the tape with a finger and ask the patient to flex as far forward as he can. Note where the 15 cm mark strikes the tape and work out the increment, which is entirely due to lumbar spine flexion. This is normally about 6–7 cm. Less than 5 cm is indicative of organic spinal pathology.
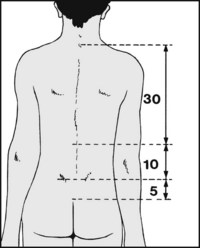
Flexion in the thoracic spine may be measured with the upper point 30 cm from the previous zero mark. Thoracic flexion is not great, and is normally in the order of 3 cm. NB: to exclude the possibility of overlay, repeat these measurements with the patient distracted, sitting up, and leaning forward on the examination couch. (Note that abdominal girth may increase after osteoporotic fractures of the lumbar spine.)

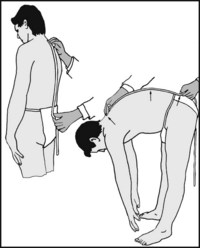
Ask the patient to arch his back, assisting him by steadying the pelvis and pulling back on the shoulder. Pain is common in prolapsed intervertebral disc and in spondylolysis. Accurate assessment with a goniometer is difficult. The maximum theoretical range is thoracic 25°; lumbar 35°; normal total range about 30°. The decrease in distance between L1 and S1 on extension may also be measured with a tape.
8.27. Movements: lateral flexion (1):
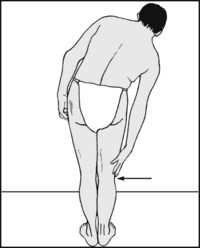
Ask the patient to slide the hands down the side of each leg in turn, and record the point reached, either in centimetres from the floor, or the position that the fingers reach on the legs.
8.28. Movements: lateral flexion (2):
Alternatively, measure the angle formed between a line drawn through T1, S1 and the vertical. The average range is 30° to either side, and the contributions of the thoracic and lumbar spine are usually equal.
The patient should be seated, and asked to twist round to each side. Rotation is measured between the plane of the shoulders and the pelvis. The normal maximum range is 40° and is almost entirely thoracic. (Lumbar contribution is 5° or less.) Some claim a more accurate assessment may be made if the test is carried out with the patient’s arms folded across the chest.
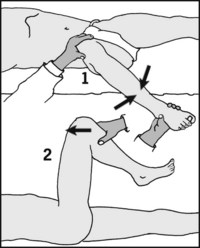
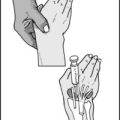
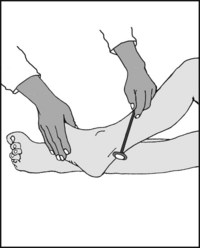
8.30. Suspected prolapsed intervertebral disc:
Always start by screening the hips. Osteoarthritis of the hip and prolapsed intervertebral disc are frequently confused. A full range of rotation in the hips, performed at 90° flexion (1) without pain at the extremes, is generally sufficient to exclude osteoarthritis as a significant cause for the patient’s complaints. Note that if there is complaint of pain on flexing the hip with the knee flexed (2) this negates a positive straight leg-raising test, and suggests osteoarthritis or overlay.

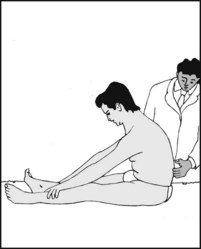
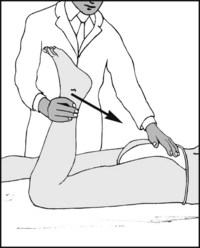
8.31. Suspected prolapsed intervertebral disc:
Straight leg-raising test (1): If the hips are normal, raise the leg from the couch while watching the patient’s face. Stop when the patient complains, and confirm that he is complaining of back or leg pain and not hamstring tightness (the test is negative if there is no pain). The production of paraesthesia or radiating root pains is highly significant, indicating nerve root irritation. Pain from S1 generally occurs before that from L5.

8.32. Straight leg raising (2):
Note the result (e.g. SLR (R) +ve at 60° or straight leg raising (R) full (no pain)). Note the site of pain: back pain suggests a central disc prolapse, leg pain a lateral protrusion. Distinguish and ignore hamstring tightness. Repeat on the good side. If well-leg raising produces pain and paraesthesia on the affected side, this is highly suggestive of a large prolapse close to the midline. Note that pain must be below the knee if the roots of the sciatic nerve are involved.

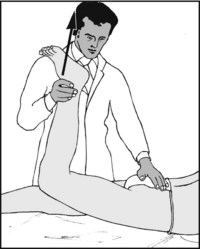
8.33. Straight leg raising (3):
Now lower the leg until pain disappears (1); then dorsiflex the foot (2). This increases tension on the nerve roots, generally aggravating any pain or paraesthesia (‘+ve sciatic stretch test’). Try this, and record the response. Alternatively, once the level of pain has been reached, flex the knee slightly (3) and apply firm pressure with the thumb in the popliteal fossa over the stretched tibial nerve (4): radiating pain and paraesthesia suggest nerve root irritation (bowstring test).
8.34. Straight leg raising (4):
If there is some doubt regarding the severity or genuineness of the patient’s complaints, ask him to sit up under the pretext of examining the back from behind. (Flexion of the spine may also be remeasured with the tape in this position.) The malingerer will have no difficulty, but the genuine patient will either flex the knees or fall back on the couch with pain (flip test).

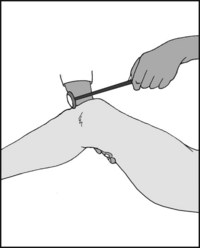
8.35. Straight leg raising (5):
Aird’s test: Alternatively, ask the patient to sit with the legs over the edge of the examination couch. Now try to lift the leg until the knee is fully extended, and note the response. If extension is achieved, this is equivalent to a straight leg raising of 90°, and suggests that there is not a sound organic basis for any positive straight leg raising obtained when the patient is supine.
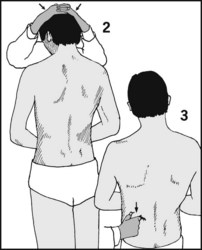
8.36. Suspected prolapsed intervertebral disc: Functional overlay, continued:
(2) Apply pressure to the head. Overlay is suggested if this aggravates the back pain. (3) Pinch the skin at the sides. Such superficial stimulation should not produce deep-seated back pain. (4) Any motor or sensory disturbance should be segmental and localised. Widespread weakness and/or stocking anaesthesia also suggest overlay (but do carry out a thorough neurological and circulatory examination).
8.37. Suspected prolapsed intervertebral disc: functional overlay contd.:
(5) Note the amount of rotation required to produce pain in the back. Now ask the patient to keep his hands firmly at his sides and repeat: the major part of the movement will now take place in the legs. Pain occurring with the same amount of apparent rotation again suggests overlay. In many centres, if three or more of the preceding tests are positive surgery is considered to be contraindicated.
8.38. Suspected prolapsed intervertebral disc: reverse Lasegue test (1):
The patient should be prone. Flex each knee in turn. This gives rise to pain in the appropriate distributions (by stretching of femoral nerve roots) in high lumbar disc lesions.
The pain produced in such a test, if positive, is normally aggravated by extension of the hip, and this should be noted. Attempt this with the knee flexed to 90° (illustrated) and also fully flexed. High disc lesions are rare compared with those affecting the L5–S1 and L4–L5 spaces. Note also that pain in the ipsilateral buttock or thigh on full knee flexion may occur in more distally situated disc prolapses.
8.40. Suspected prolapsed intervertebral disc (2):
Look for further evidence of neurological involvement. A reduced or absent tendon reflex is a highly significant finding accompanying positive straight-leg raising or positive reverse Lasegue tests, but in practice confirmatory findings of this nature may not be present. Although two spinal segments are involved in both the knee and ankle reflexes, it is common practice to assess the integrity of L4 by the presence of the knee jerk.
8.41. Suspected prolapsed intervertebral disc (3):
Similarly, S1 alone may be assigned to the ankle jerk. Absence of one or both ankle jerks is usually a significant clinical finding, and does not occur in normal individuals below the age of 30. Unilateral absence may be found in the absence of pathology in 3–5% of individuals in the 40–60 age group, and in 7–10% of those over 80. Absence of both reflexes increases to 80% in those aged 90–100.

8.42. Suspected prolapsed intervertebral disc (4):
Root pressure from a disc may affect myotomes and dermatomes in a rather selective fashion (see Ch. 2 on segmental innervation). Note the presence of any muscle wasting. Ask the patient to dorsiflex both feet. Now attempt to force them into plantarflexion against his resistance (L4,5).

8.43. Suspected prolapsed intervertebral disc (5):
Shift the grip to the great toes and test the power of dorsiflexion. Repeat with the lesser toes (L4,5). Note that many regard weakness of dorsiflexion of the great toe as a most sensitive test of the L5 root alone, a root where there is no appropriate tendon reflex available for assessment. Now test the power of plantarflexion of the great and lesser toes (S1,2).

8.44. Suspected prolapsed intervertebral disc (6):
Encircle the feet with the hands and test the power of the peronei against the patient’s resistance (L5, S1). Test the power of the quadriceps (L3,4) when a high disc lesion is suspected. Note that prolonged muscle weakness will be accompanied by muscle wasting. Look for this clinically, and if you suspect it compare the girths of both the calves.

8.45. Suspected prolapsed intervertebral disc (7):
Test sensation to pinprick in the dermatomes of the lower limb. Test perineal sensation in suspected central disc prolapse. Diminution of sensation at the side of the foot (S1) is one of the commonest findings (see also Ch. 2, Segmental and Peripheral Nerves of the Limbs). Note also that stocking anaesthesia may be found in diabetic neuropathy and peripheral vascular disease, and is not necessarily evidence of a nonorganic problem.
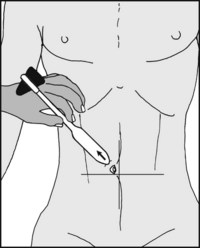
8.46. Suspected thoracic cord compression:
This may be crudely assessed by testing the abdominal reflexes. Use a blunt object such as the handle of a tendon hammer to stroke the skin in each paraumbilical skin quadrant. Failure of the umbilicus to twitch in the direction of the stimulated quadrant suggests cord compression on that side at the appropriate level. (The muscles of the upper quadrants are supplied by T7–10, and the lower by T10–L1.)
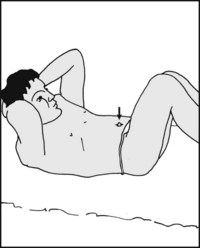
8.47. Suspected thoracic motor root dysfunction:
Beevor’s sign: The patient is asked to place his hands behind his head, flex his knees, and sit up. Movement of the umbilicus to one side (and up or down) suggests that the abdominal muscles on that side are unopposed, i.e. there is weakness on the opposite side. (See Frame 8.46 for the relevant muscle innervation.) This may result from nerve root compression by an osteophyte, from a local tumour, poliomyelitis or spinal dysraphism.
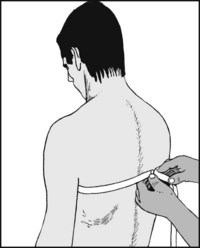
8.48. Suspected ankylosing spondylitis:
Check the patient’s chest expansion at the level of the fourth interspace. The normal range in an adult of average build is at least 6 cm. Less than 2.5 cm is regarded as highly suggestive of ankylosing spondylitis. In addition, look for evidence of iritis, which is often associated with this condition.

8.49. Suspected sacroiliac joint involvement (1):
Flex the hip and knee and forcibly adduct the hip. Pain may accompany this manoeuvre in early ankylosing spondylitis, tuberculosis and other infections, and Reiter’s syndrome, but many false positives do occur with this test.

8.50. Suspected sacroiliac joint involvement (2):
Note whether pain is produced by pelvic compression or by trying to ‘open out’ the pelvis with the thumbs hooked round the anterior spines. Alternatively, with the patient in the prone position, place the side of one hand over the sacrum and upper natal cleft; press down hard, using the other hand to assist. True sacroiliac pain may occur in women shortly before and after childbirth.

This is an essential part of the investigation of all cases of back pain. Rectal or vaginal examination may be required on the indication of the history and any other elements in the case. The sacrococcygeal joint may be examined by first grasping the coccyx between the index (in the rectum) and the thumb outside, and then gently moving the joint. In coccydynia, marked pain normally accompanies this manoeuvre.
The peripheral pulses and circulation should also be checked in all cases. Back and leg pain caused by arterial insufficiency is usually aggravated by activity, and absence of femoral pulsation is of particular significance.
Estimation of the sedimentation rate is a valuable screening test in the investigation of all spinal complaints. It is normal in prolapsed intervertebral disc, mechanical back pain, spinal stenosis and Scheuermann’s disease, but elevated in ankylosing spondylitis, many infections and neoplasms. It is best if 25 mm is taken as the upper limit of normal. False positives are not uncommon, but false negatives are rare.

An anteroposterior and lateral are the standard projections for both the lumbar and thoracic spine. Localised views of the lumbosacral junction are a useful addition. This is a typical example of a normal lateral radiograph of the lumbar spine. In filling out the request card, if a specific area is under suspicion state this if possible, so that the central ray of the projection can be appropriately positioned.

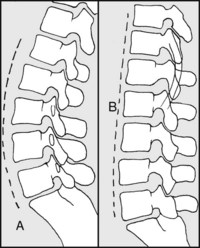
In the lateral, note first the lumbar curve: (A) typical normal; (B) loss of lordosis (most often seen in prolapsed intervertebral disc as a result of protective muscle spasm, but not confirmatory).
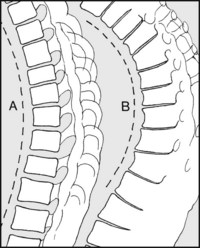
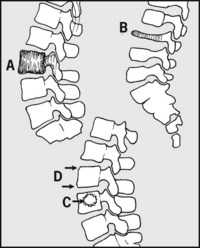
In the thoracic spine note (A) a typical normal curve; (B) an increased but regular curve typical of senile kyphosis. Scheuermann’s disease is another frequent cause of a regular dorsal kyphosis. Kyphosis may be measured on the radiographs with the technique for assessing scoliosis (see later). 45° is taken as the upper limit of normal.
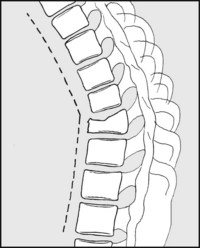
In both the lumbar and the thoracic spine note any sharp alteration in the curvature (angular kyphosis), found typically where there is pathology restricted to one or two vertebral bodies, e.g. from fractures, TB or other infections, tumour, osteoporosis and osteomalacia with local vertebral body collapse.
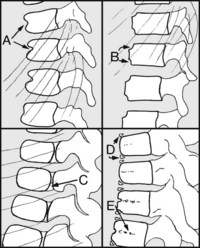
Now look at the shape of the bodies and the size of the discs. Compare with the bodies and disc spaces above and below. The following are normal in the child’s spine: (A) anterior clefts, (B) anterior notches, (C) incomplete fusion of elements, (D) epiphyses, (E) vascular tracks (which may persist).
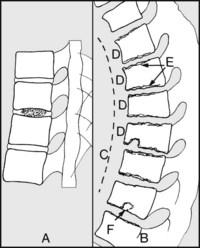
Note (A) disc calcification; (B) the typical appearance of Scheuermann’s disease, with (C) kyphosis, (D) anterior wedging of not less than 5° involving at least three sequential vertebrae, (E) ragged appearance of the epiphyses. Note (F) a central disc herniation (Schmorl’s node); this is not always associated with Scheuermann’s disease.
Note (A): disc narrowing at any level in the spine is the earliest evidence of tuberculosis and other infections; (B) Narrowing at L5–S1 and, less commonly, in the two spaces above occurs in long-standing disc lesions and is often associated with anterior lipping.
Note (A) increased density and the ‘picture-frame’ appearance of the vertebral bodies in Paget’s disease; (B) marked narrowing and increased density seen in Calvé’s disease (vertebra plana); (C) any space-occupying lesion in a vertebral body (usually due to tumour or infection (but note Schmorl’s nodes)); (D) corner vertebral erosions (Romanus lesions), seen in ankylosing spondylitis.
Note the relationship of each vertebra to its neighbour. In particular, note (A) spondylolisthesis (see also later); (B) retrospondylolisthesis (usually associated with disc degeneration).
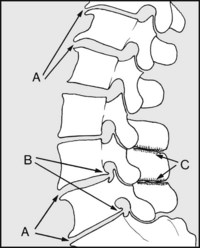
Lipping is seen in chronic disc lesions, mainly at L5–S1, but also at the other rarer disc prolapse sites. Note (A) anterior lipping; (B) posterior lipping. Lipping is also the main feature (at all levels) of osteoarthritis. Note (C) impingement of spinous processes (‘kissing spines’).


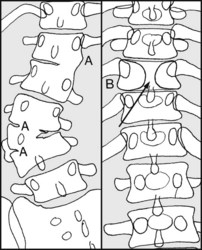
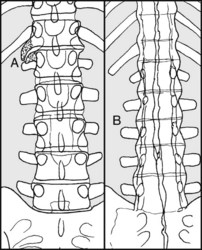
In the anteroposterior view note the presence of any congenital abnormalities, such as (A) congenital vertebral fusion, often associated with a congenital scoliosis; (B) anterior spina bifida, in which there is failure of fusion of the vertebral body elements (this is usually symptom free).
Note also any anomalies of the lumbosacral articulation, such as (C) partial sacralisation of the fifth lumbar vertebra, a possible cause of low back pain. Note also (D) the presence of (posterior) spina bifida.
Note (A) the presence of any localised lateral angulation of the spine due to lateral vertebral collapse, e.g. from fracture, infection, tumour, osteoporosis or other causes; (B) hemivertebra, a common cause of congenital scoliosis (note that, as illustrated, this is usually associated with an extra rib).
Look at the soft tissue shadows at the sides of the vertebrae, observing, for example, the fusiform increased density typical of a tuberculous abscess. Note disc obliteration and early lateral wedging.
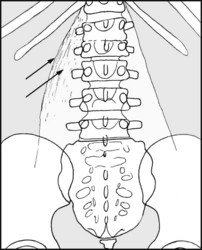
Examine the psoas shadows for symmetry. Lateral displacement of the edge of the shadow, and increased density within the main area occupied by psoas, suggests a psoas abscess, typically found in tuberculosis of the lumbar or lowermost thoracic spine.
Look for lateral lipping, (A); at D12–L1 it may be an early sign of ankylosing spondylitis, but there and elsewhere it usually indicates osteoarthritis. ‘Bamboo spine’ (B) is diagnostic of ankylosing spondylitis. Note any body and facet joint fusions and ligament calcification.
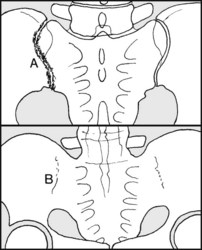
Look at the sacroiliac joints. (A) Unilateral involvement (sclerosis, cystic changes or obliteration) may occur in tuberculosis and other infections. Any asymmetry should be investigated by oblique projections and, if necessary, tomography or CT scans. Bilateral involvement (B) is common in ankylosing spondylitis, and should always be sought when this condition is suspected.

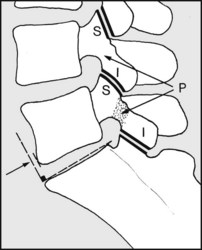
Look for evidence of spondylolisthesis. In the normal spine the pars interarticularis (P) lying between (S) the superior and (I) the inferior articular facets is intact, and a vertical raised from the anterior margin of the sacrum lies in front of L5.
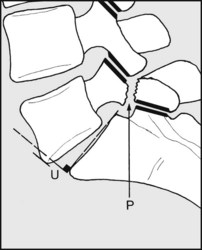
If spondylolisthesis is suspected, the lateral should always be taken with the patient standing. Note any defect (P) and any forward slip (U). The deformity may occur between L5 and S1, and much less frequently between L4/L5 or L3/L4.
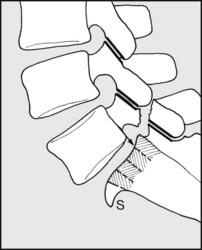
Note that (S) new bone formation (buttressing), if present, may make use of the anterior edge of the sacrum as a reference unreliable. Instead, note the relationship between the posterior edge of the slipping vertebra to the one below. The example shows a forward slip of 25%.

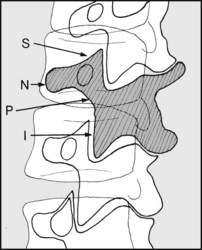
Oblique views are invaluable, provided they are taken in the plane of any defect. In interpreting these, identify the ‘Scotty dog’ shadows (shown dark grey and hatched). The nose (N) is formed by a transverse process; the ear (S) by a superior articular process; the front legs (I) by an inferior articular process; the neck (P) by the pars interarticularis.
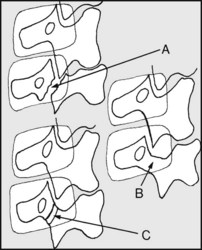
In spondylolisthesis (A) the ‘dog’ becomes decapitated owing to forward slip, and the inferior articular process of the vertebra above encroaches on the neck. In spondylolysis, where no slip has occurred, the neck (B) is elongated or (C) develops a collar. CT scans can also be of value provided the so-called gantry angle of the projection is at right angles to the plane of the table.
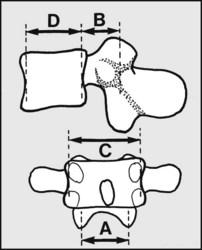
Where spinal stenosis is suspected, calculate the canal to body ratio, A×B:C×D, where A = interpedicular distance, B = spinal canal front-to-back (measured to the root of the spinous process), C = width of vertebral body, D = body, front-to-back. The normal range is from approximately 1 : 2–1 : 4.5. Values greater than 4.5 suggest spinal stenosis, but CT scans are of particular value in clarifying the site and extent of any narrowing.
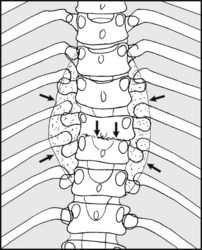
Note the presence of any structural scoliosis. This is associated with rotation of the vertebral spines towards the concavity (A), and narrowing of pedicles. On the convexity of the curve there is widening of disc spaces (B). In the thorax there is ribcage distortion (C). Identify the primary curves clinically, or by assessing absence of movement in lateral flexion radiographs.
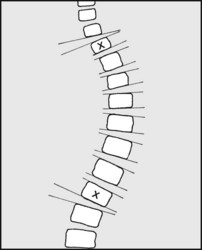
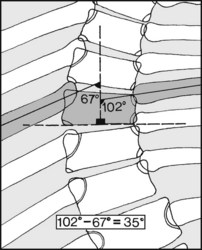
To assess the severity of a scoliotic curve, and to allow its progress to be monitored it is necessary to measure the deformity. The Cobb method is most popular, although it is difficult to obtain consistent results with it. First, find the upper and lower limits of the primary curve by drawing tangents to the bodies and noting where the disc spaces begin to widen on the concavity of the curve.
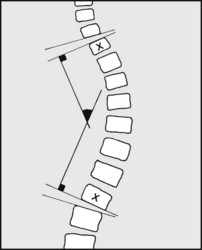
Now erect perpendiculars from the vertebrae that form the limits of the curve (marked ‘X’). Note the angle between them. This is a measure of the primary curve, and can be used for comparison with past and future radiographs. Kyphotic curves may be measured in a similar way. Any decision regarding treatment must take into account the clinical picture, and not rely on the radiographs alone.
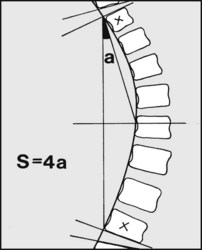
Capasso’s method of measuring scoliotic curves is said to be more sensitive and accurate. The magnitude of the scoliotic curve (S) in degrees is obtained by multiplying by 4 the angle (a) subtended by a line joining the ends of the curves, with one running from the centre of the curve to one end of the curve: i.e. S = 4a. Again, note that in any case of suspected idiopathic scoliosis an MRI scan is mandatory to exclude syringomyelia, which is said to occur in 25% of cases.
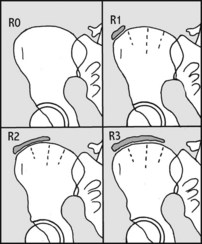
8.86. Assessing skeletal maturity (1):
Scoliotic curves deteriorate with growth, and the prognosis is often dependent on how much more the child has to grow. This may be judged by examining appropriate radiographs and assessing sexual maturity. Risser grading of skeletal maturity uses radiographs of the iliac crest and its apophysis (which ossifies from in front backwards). R0 = the ossification centre has not appeared; R1 = up to 25% is present; R2 = up to 50% is present; R3 = up to 75% is present.

8.87. Assessing skeletal maturity (2):
R4 = up to the whole of the apophysis is ossified. R5 = the apophysis has fused and all growth has ceased. In girls, Risser 1 and 5 commonly occur at ages  and
and  , and in boys at
, and in boys at  and
and  . It has been found that those having 5–19° or 20–29° curves at Risser 0 or 1 have respectively 22% and 68% chances of deteriorating 6° or more; while those at Risser 2–4 in the same range had only a 1.6% and 23% chance of deteriorating the same amount.
. It has been found that those having 5–19° or 20–29° curves at Risser 0 or 1 have respectively 22% and 68% chances of deteriorating 6° or more; while those at Risser 2–4 in the same range had only a 1.6% and 23% chance of deteriorating the same amount.
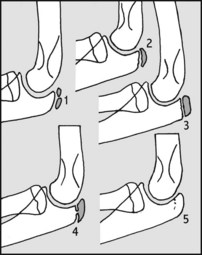
8.88. Assessing skeletal maturity (3).
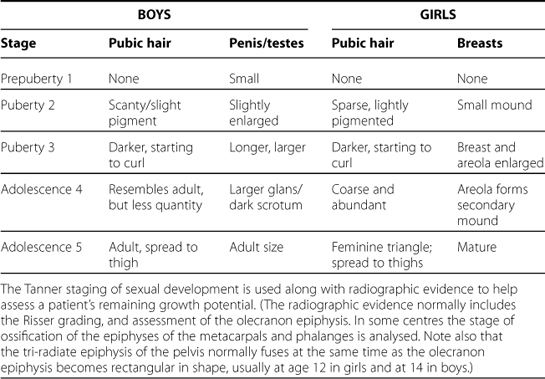
As the final growth spurt is well advanced before R1, a means of earlier staging is desirable, This may be achieved by examining ossification of the olecranon epiphysis. From its first appearance to fusion occurs over 6 monthly stages between the ages of 11 and 13 in girls, and 13 and 15 in boys. 1 = appearance of two centres; 2 = the epiphysis becomes half moon shaped; 3 = the epiphysis becomes square shaped; 4 = partial union; 5 = complete union.
In infantile scoliosis note the difference in rib angles at the apex of the curve by the shown construction. A difference of 20° or more must be regarded as indicating a potentially progressive scoliosis. An improvement over a 3-month period carries a good prognosis (Mehta). The best prognosis in infantile scoliosis is in males where the onset occurs in the first year of life and the rib–vertebral angle difference (RVAD) is less than 20°.
Other investigations in suspected PID:

8.91. Spinal radiographs: special features:
These three radiographs demonstrate anterior clefts, anterior notches, epiphyses and vascular tracks – normal features of the growing spine.

8.92. Spinal radiographs: examples of pathology (1):
The radiograph shows narrowing of a single disc space.
Diagnosis: in this case the diagnosis was of tuberculosis of the spine. In most cases of spinal infections loss of disc height is the earliest sign.

The vertebral bodies throughout the thoracic and lumbar spine are fused, with early bambooing of the spine. The facet joints and the sacroiliac joints are also fused. There is ossification of the interspinous ligaments.

In this radiograph of a girl of 10 there is complete flattening of a single vertebral body, with preservation of the disc spaces above and below.
Diagnosis: vertebra plana (Calvé’s disease) due to eosinophilic granuloma. Note also the vertebral notches.
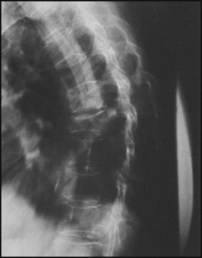
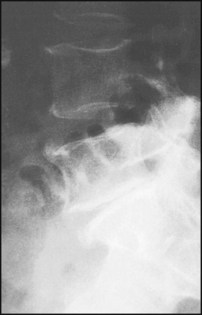
There is an angular kyphosis, with anterior wedging of D9.
Diagnosis: pathological fracture associated with osteomalacia. Similar appearances are found in the presence of spinal metastases.

The radiograph shows a thoracic scoliosis, convex to the patient’s right. There is vertebral rotation and asymmetry of the rib cage.
Diagnosis: idiopathic scoliosis, with fixed primary thoracic curve.
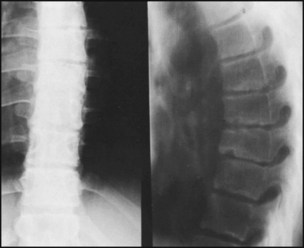
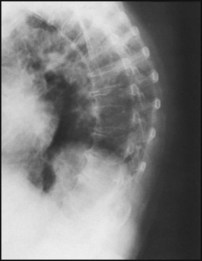
There is a regular kyphosis, with slight anterior wedging of the vertebral bodies, irregularity of the disc margins and central disc herniation (Schmorl’s nodes).
Diagnosis: the appearances are typical of Scheuermann’s disease. Clinically the kyphosis was obvious, and spinal movements were greatly reduced.

The radiograph is of an 8-year-old boy complaining of back pain, malaise, night sweats, loss of spinal movements, and pain on percussion over the spine. There is loss of a disc space, slight vertebral wedging, and a fusiform abscess shadow on both sides of the spine.
Diagnosis: the appearances are typical of tuberculosis of the spine.
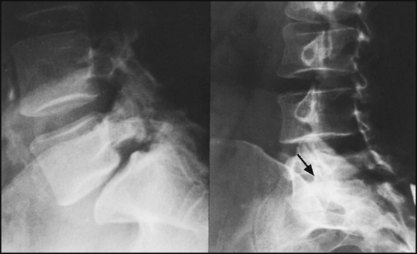
The lateral radiographs show that there is forward slip of L5 on S1 of a little less than 25%. There is an associated defect in the pars interarticularis of L5. In the oblique projection the ‘Scotty dog’ has been decapitated. The patient complained of low back and buttock pain.

There is increased density of the bony shadows in the region of the right sacroiliac joint, whose outline has become obscured. There was associated local pain, malaise and pyrexia. Attempts to spring the sacroiliac joints produced great pain.
Diagnosis: The appearances are typical of an infective (pyogenic) arthritis of the sacroiliac joint.
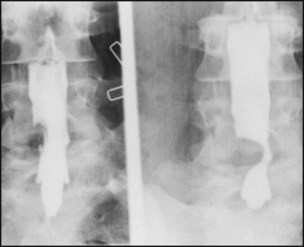
This is the myelogram of a patient complaining of back and right leg pain. There was weakness of dorsiflexion and eversion of the right foot, and there was some sensory impairment over the lateral aspect of the calf. The myelogram shows a well defined indentation of the contrast medium at the L4/5 level.
Diagnosis: prolapsed intervertebral disc. At operation the L5 root was found stretched over the prolapse.

There is calcification in an intervertebral disc with no significant narrowing of the corresponding disc space.
Diagnosis: This is an incidental finding, and is of no particular significance as a cause of low back pain.
There is narrowing of the L5–S1 disc space, with anterior lipping of the corresponding vertebrae.
Diagnosis: the appearances are typical of degenerative disc disease and lumbosacral osteoarthritis.

There is striking alteration of bone texture affecting a single vertebra.
Diagnosis: this ‘picture frame’ appearance is typical of Paget’s disease. At this site there would not necessarily be any associated symptoms.

There is a transitional vertebra, with the transverse process on one side articulating with both the sacrum and ilium.
Diagnosis: congenital abnormality of lumbosacral articulation. Some consider that this pattern of spinal anomaly, because it produces an asymmetrical distribution of local stresses, may be a cause of back pain.
The radiographs show a regular dorsal kyphosis associated with anterior vertebral lipping and a degree of osteoporosis.

The spinous process of L5 (and less obviously S1), along with associated posterior elements, is absent.
Diagnosis: spina bifida occulta. The only disturbance noted in the lower limbs was a bilateral pes cavus.

The radiographs shows a dorsal scoliosis associated with an anomaly of a vertebral body and an extra rib on the convexity of the curve.