Spine
A Anatomy (see Chapter 2, Anatomy)
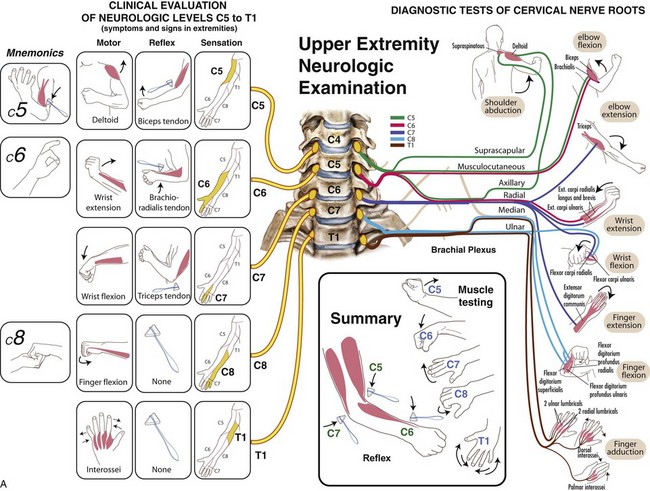
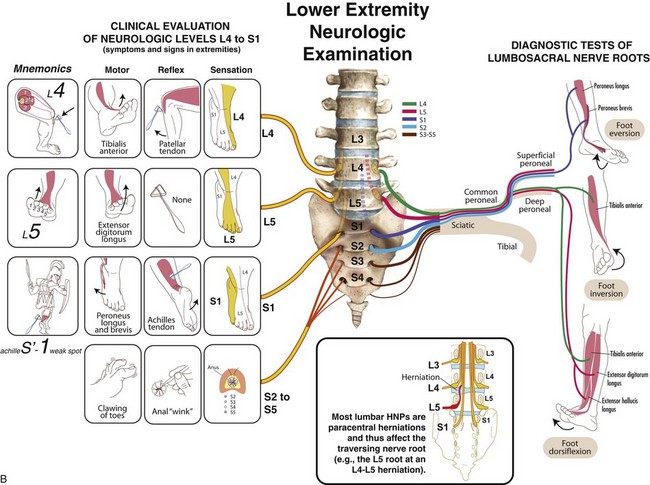
B History and physical examination (Table 8-1; Figure 8-1)
Table 8-1
Examination of Patients with Disorders of the Spine
| Component | Features |
| Inspection | Overall alignment in sagittal and coronal planes (sciatic scoliosis) |
| Gait | Wide-based (myelopathy), forward-leaning (stenosis), antalgic |
| Palpation | Localized posterior swelling (trauma), acute gibbus deformity, tenderness |
| Range of motion | Flexion/extension, lateral bend, full versus limited |
| Neurologic function | Motor, sensory, reflexes, assessment of long-tract signs (see also Table 8-7) |
| Special tests | Straight-leg raise, Spurling test, Waddell signs of inorganic pathology |

1. Localized pain (tumor, infection)
2. Mechanical pain (instability, discogenic disease)
3. Radicular pain (herniated nucleus pulposus [HNP], stenosis), night pain (tumor)
4. Systemic symptoms such as fever or unexplained weight loss (infection, tumor)
5. The physical examination must evaluate both the spine and the neurologic function of the extremities (Table 8-2).


6. Localized hip and shoulder pathology may simulate spine disease and must also be evaluated.
1. Plain radiographs should be obtained 4 to 6 weeks after onset of symptoms; add flexion-extension views for suspected instability.
2. Magnetic resonance imaging (MRI) is excellent for further imaging of HNP, stenosis, soft tissue, tumor, and infection.
3. Computed tomography (CT) with fine cuts ± myelographic dye is used to examine bony anatomy after previous surgery and the quality of fusion.
4. Bone scan is helpful in evaluating metastatic disease and may be negative with multiple myeloma.
5. Laboratory evaluation consists of C-reactive protein and erythrocyte sedimentation rate for infection, metabolic screening, serum/urine protein electrophoresis for myeloma, and a complete blood cell count (there is often a high-normal white blood cell count with infection or anemia with myeloma).
D Workup of back pain—Complaint of back pain is second only to upper respiratory tract infection as a cause of office visits, with 60% to 80% lifetime prevalence. Standard workup begins with a history (most important) and progresses to physical examination (see Table 8-1). Radiographic and laboratory studies rarely help in acute cases. The following considerations in the evaluation of back pain are important:
 Children may be affected by congenital or, more often, developmental disorders or infection.
Children may be affected by congenital or, more often, developmental disorders or infection.
 Young adults are more likely to suffer from disc disease, spondylolisthesis, or acute fractures.
Young adults are more likely to suffer from disc disease, spondylolisthesis, or acute fractures.

2. Radicular signs and symptoms
 Often associated with disc herniation or spinal stenosis
Often associated with disc herniation or spinal stenosis

 Herpes zoster is a rare cause of lumbar radiculopathy, with pain preceding the skin eruption.
Herpes zoster is a rare cause of lumbar radiculopathy, with pain preceding the skin eruption.
3. Systemic symptoms—Careful history-taking can help guide diagnosis of systemic conditions with associated spine pathology.









 Infection (confirmed by laboratory studies)
Infection (confirmed by laboratory studies)

 Chronic back pain is often refractory to localized treatment in many patients with fibromyalgia.
Chronic back pain is often refractory to localized treatment in many patients with fibromyalgia.






4. Sources of referred back pain










5. Psychogenic pain—may play important role in some patients with chronic low back disorders









A Cervical spondylosis—Chronic disc degeneration and associated facet arthropathy result in three clinical entities:
 Discogenic neck pain (axial pain)
Discogenic neck pain (axial pain)
 Radiculopathy (root compromise)
Radiculopathy (root compromise)
 Myelopathy (cord compression) and combinations of these conditions
Myelopathy (cord compression) and combinations of these conditions








2. Pathoanatomy—Cervical spondylosis involves the intervertebral disc and four other articulations (Figure 8-2):
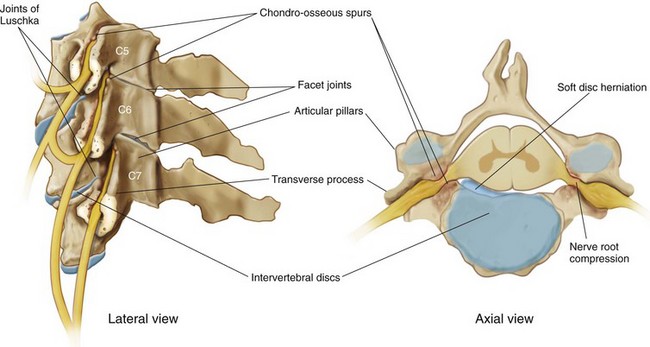
 Two uncovertebral joints (of Luschka)
Two uncovertebral joints (of Luschka)

 Cord compromise as canal diameter decreases
Cord compromise as canal diameter decreases






 Usually posterolateral, between the posterior edge of the uncinate process and the lateral edge of the posterior longitudinal ligament, it may result in acute radiculopathy.
Usually posterolateral, between the posterior edge of the uncinate process and the lateral edge of the posterior longitudinal ligament, it may result in acute radiculopathy.


 Ossification of the posterior longitudinal ligament
Ossification of the posterior longitudinal ligament



 Neck flexion results in slight increase in canal diameter and relief of cord compression.
Neck flexion results in slight increase in canal diameter and relief of cord compression.
3. Signs and symptoms—Degenerative discogenic neck pain may present as the insidious onset of neck pain without neurologic signs or symptoms, exacerbated by excess vertebral motion.


 Can involve one or multiple roots
Can involve one or multiple roots
 Neck, shoulder, and arm pain; paresthesias; and numbness
Neck, shoulder, and arm pain; paresthesias; and numbness
 Overlapping findings because of intraneural intersegmental connections of sensory nerve roots
Overlapping findings because of intraneural intersegmental connections of sensory nerve roots

 Relief of radicular pain with shoulder abduction is suggestive of a cervical etiology.
Relief of radicular pain with shoulder abduction is suggestive of a cervical etiology.
 Caudal nerve root at a given level is usually affected (see Table 8-2).
Caudal nerve root at a given level is usually affected (see Table 8-2).













4. Physical examination findings





















 Effectively demonstrates neural compressive pathology
Effectively demonstrates neural compressive pathology











 Nonsteroidal anti-inflammatory drugs (NSAIDs)
Nonsteroidal anti-inflammatory drugs (NSAIDs)
 Extraforaminal cervical nerve blocks
Extraforaminal cervical nerve blocks


 Temporary collar immobilization
Temporary collar immobilization

 Pain clinic modalities are helpful in most cases of discogenic neck pain and radiculopathy
Pain clinic modalities are helpful in most cases of discogenic neck pain and radiculopathy







 Combined anterior (cervical) Smith-Robinson discectomy and fusion (ACDF)
Combined anterior (cervical) Smith-Robinson discectomy and fusion (ACDF)
 Involves excision of osteophytes and corpectomy with a strut graft fusion with or without instrumentation
Involves excision of osteophytes and corpectomy with a strut graft fusion with or without instrumentation


















 Used for multilevel spondylosis and myelopathy and ossification of posterior longitudinal ligament (OPLL)
Used for multilevel spondylosis and myelopathy and ossification of posterior longitudinal ligament (OPLL)
 Allows for more extensive decompression
Allows for more extensive decompression
 Lower incidence of instability compared with multilevel laminectomies
Lower incidence of instability compared with multilevel laminectomies
 Contraindicated in setting of fixed kyphosis
Contraindicated in setting of fixed kyphosis










1. Congenital versus acquired (traumatic, degenerative)
2. Absolute stenosis (anteroposterior canal diameter <10 mm)
3. Relative stenosis (anteroposterior canal diameter 10 to 13 mm)
4. Pavlov (Torg) ratio (canal/vertebral body width) should be 1.0.
 Ratio of less than 0.80 or a sagittal diameter of less than 13 mm is considered a significant risk factor for later neurologic involvement.
Ratio of less than 0.80 or a sagittal diameter of less than 13 mm is considered a significant risk factor for later neurologic involvement.
5. Minor trauma such as hyperextension may lead to a central cord syndrome, even without overt skeletal injury.
6. Surgery may serve a prophylactic function but is usually reserved for patients who develop myelopathy or radiculopathy.
 Cervical spine involvement is common in rheumatoid arthritis (occurring in up to 90% of patients) and is more common with long-standing disease and multiple joint involvement.
Cervical spine involvement is common in rheumatoid arthritis (occurring in up to 90% of patients) and is more common with long-standing disease and multiple joint involvement.






 Neurologic impairment with rheumatoid arthritis has been classified by Ranawat (Table 8-3).
Neurologic impairment with rheumatoid arthritis has been classified by Ranawat (Table 8-3).
Table 8-3
Ranawat Classification of Neurologic Impairment in Rheumatoid Arthritis
| Grade | Characteristics |
| I | Subjective paresthesias, pain |
| II | Subjective weakness; upper motor neuron findings |
| III | Objective weakness; upper motor neuron findings |
| IIIA | Ambulatory |
| IIIB | Nonambulatory |

 Look for subtle signs of neurologic involvement.
Look for subtle signs of neurologic involvement.
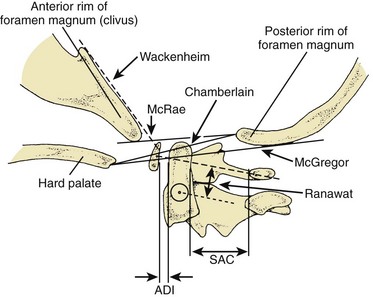
 Assess the radiographic markers for impending neural compression (Figure 8-3).
Assess the radiographic markers for impending neural compression (Figure 8-3).




 Indications for surgical stabilization:
Indications for surgical stabilization:






 Patients with rheumatoid arthritis should have flexion/extension films before elective surgery.
Patients with rheumatoid arthritis should have flexion/extension films before elective surgery.
2. Atlantoaxial subluxation—occurs in 50% to 80% of cases of rheumatoid arthritis and is often the result of pannus formation at synovial joints between the dens and the ring of C1, resulting in destruction of transverse ligament, dens, or both

 Anterior subluxation of C1 on C2 is the most common finding, but posterior and lateral subluxation can also occur.
Anterior subluxation of C1 on C2 is the most common finding, but posterior and lateral subluxation can also occur.
 Findings on examination may include limitation of motion, upper motor neuron signs, and weakness.
Findings on examination may include limitation of motion, upper motor neuron signs, and weakness.





 Transarticular screw fixation (Magerl) across C1-C2 eliminates the need for halo immobilization associated with wiring alone.
Transarticular screw fixation (Magerl) across C1-C2 eliminates the need for halo immobilization associated with wiring alone.

 Nonreducible atlantoaxial subluxation
Nonreducible atlantoaxial subluxation


 Anterior cord compression because of pannus often resolves after posterior spinal fusion.
Anterior cord compression because of pannus often resolves after posterior spinal fusion.
 Odontoidectomy should be reserved as a secondary procedure.
Odontoidectomy should be reserved as a secondary procedure.
 Surgery is less successful in Ranawat grade IIIB patients but should be considered.
Surgery is less successful in Ranawat grade IIIB patients but should be considered.



3. Cranial settling (basilar invagination)
 The second most common manifestation of rheumatoid arthritis in cervical spine
The second most common manifestation of rheumatoid arthritis in cervical spine
 Forty percent of patients with rheumatoid arthritis
Forty percent of patients with rheumatoid arthritis
 Cranial migration of the dens from erosion and bone loss between the occiput and C1-C2
Cranial migration of the dens from erosion and bone loss between the occiput and C1-C2
 Often seen in combination with fixed atlantoaxial subluxation
Often seen in combination with fixed atlantoaxial subluxation
 Measurements are shown in Figure 8-3.
Measurements are shown in Figure 8-3.



 Cervicomedullary angle less than 135 degrees (on MRI) suggests impending neurologic impairment.
Cervicomedullary angle less than 135 degrees (on MRI) suggests impending neurologic impairment.

 Transoral or retropharyngeal dens resection for brainstem compression
Transoral or retropharyngeal dens resection for brainstem compression


 Occurs in 20% of cases of rheumatoid arthritis
Occurs in 20% of cases of rheumatoid arthritis
 Seen in combination with upper cervical spine instability
Seen in combination with upper cervical spine instability







D Cervical spine and cord injuries—See Chapter 11, Trauma, for classification and treatment of cervical spine injuries.








 Spinal shock usually involves a 24- to 72-hour period of paralysis, hypotonia, and areflexia.
Spinal shock usually involves a 24- to 72-hour period of paralysis, hypotonia, and areflexia.

 Injuries below the thoracolumbar level (conus or cauda equina) may permanently interrupt the bulbocavernosus reflex.
Injuries below the thoracolumbar level (conus or cauda equina) may permanently interrupt the bulbocavernosus reflex.

 In complete injuries, further neurologic improvement is minimal.
In complete injuries, further neurologic improvement is minimal.







3. Physical and neurologic examination

 Facial injuries, hypotension, and localized tenderness or spasm should be investigated.
Facial injuries, hypotension, and localized tenderness or spasm should be investigated.
 Careful neurologic examination to document the lowest remaining functional level and to assess the patient for the possibility of sacral sparing (sparing of posterior column function, indicating an incomplete spinal cord injury) is essential (see Figure 8-1).
Careful neurologic examination to document the lowest remaining functional level and to assess the patient for the possibility of sacral sparing (sparing of posterior column function, indicating an incomplete spinal cord injury) is essential (see Figure 8-1).


 Complete cervical spine series (C1-T1)
Complete cervical spine series (C1-T1)








 Oblique views to investigate facet subluxation, dislocations, or fractures
Oblique views to investigate facet subluxation, dislocations, or fractures












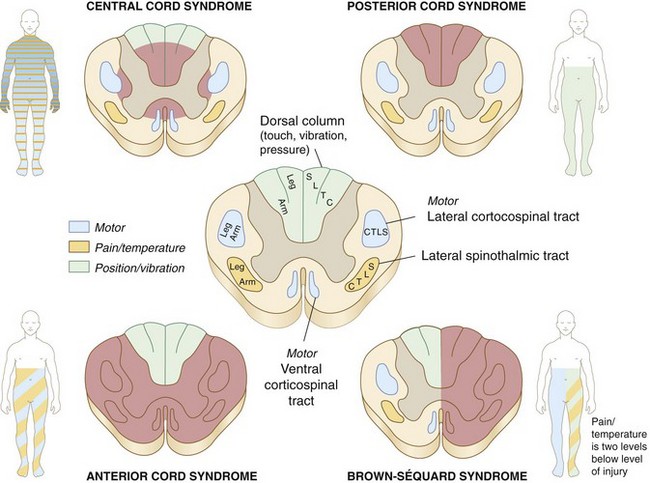
Figure 8-4 Incomplete spinal cord injury syndromes.
Incomplete spinal cord injury syndromes.







 Defined as some sparing of distal motor or sensory function
Defined as some sparing of distal motor or sensory function
 Three important generalizations regarding prognosis:
Three important generalizations regarding prognosis:



 Anatomic classification of incomplete spinal cord injury (Table 8-4)
Anatomic classification of incomplete spinal cord injury (Table 8-4)

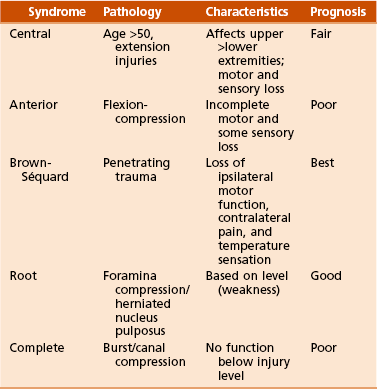


 Presents as upper greater than lower extremity motor and sensory loss
Presents as upper greater than lower extremity motor and sensory loss
 Often seen in patients with preexisting cervical spondylosis who sustain a hyperextension injury
Often seen in patients with preexisting cervical spondylosis who sustain a hyperextension injury
 Cord is compressed anteriorly by osteophytes and posteriorly by the infolded ligamentum flavum.
Cord is compressed anteriorly by osteophytes and posteriorly by the infolded ligamentum flavum.




 The second most common incomplete cord injury
The second most common incomplete cord injury
 Damage is primarily in the anterior two thirds of the cord.
Damage is primarily in the anterior two thirds of the cord.
 Posterior columns spared (proprioception and vibratory sensation)
Posterior columns spared (proprioception and vibratory sensation)
 Patients demonstrate greater motor loss in the legs than the arms.
Patients demonstrate greater motor loss in the legs than the arms.
 CT may demonstrate bony fragments compressing the anterior cord.
CT may demonstrate bony fragments compressing the anterior cord.












6. Treatment—See Chapter 11, Trauma.




















 Used acutely to realign the spine in the presence of a displaced fracture with or without neurologic injury
Used acutely to realign the spine in the presence of a displaced fracture with or without neurologic injury











 Potentially negative outcomes are numerous and include neurologic injury, nonunion, and malunion.
Potentially negative outcomes are numerous and include neurologic injury, nonunion, and malunion.

 Associated with greater than 3.5 mm of subluxation and greater than 11 degrees of difference in angulation between adjacent motion segments
Associated with greater than 3.5 mm of subluxation and greater than 11 degrees of difference in angulation between adjacent motion segments










8. Prognosis—The Frankel classification is useful when assessing functional recovery from spinal cord injury (Table 8-5).
Table 8-5
Frankel Classification of Cervical Spine Injuries
| Frankel Grade | Function |
| A | Complete paralysis |
| B | Sensory function only below injury level |
| C | Incomplete motor function (grades 1-2 of 5) below injury level |
| D | Fair to good (useful) motor function (grades 3-4 of 5) below injury level |
| E | Normal function (grade 5 of 5) |
E Sports-related cervical spine injuries
 Commonly associated with stretching of the upper brachial plexus by bending the neck away from the depressed shoulder or neck extension toward the painful shoulder in the setting of foraminal stenosis (root irritation)
Commonly associated with stretching of the upper brachial plexus by bending the neck away from the depressed shoulder or neck extension toward the painful shoulder in the setting of foraminal stenosis (root irritation)
 Symptoms include burning dysesthesia and weakness in the involved extremity.
Symptoms include burning dysesthesia and weakness in the involved extremity.


 Usually seen after axial load injury (spearing) but may also be seen after forced hyperextension or hyperflexion
Usually seen after axial load injury (spearing) but may also be seen after forced hyperextension or hyperflexion
 Presents as bilateral burning paresthesia and weakness or paralysis
Presents as bilateral burning paresthesia and weakness or paralysis






 The third and fourth cervical levels are the most commonly affected.
The third and fourth cervical levels are the most commonly affected.
 It has no definitive association with future permanent neurologic injury.
It has no definitive association with future permanent neurologic injury.











A Differential diagnosis—The physical examination, imaging studies, and laboratory tests assist with the differential diagnosis (Table 8-6).
Table 8-6
Differential Diagnosis of Disorders in the Lumbar Spine
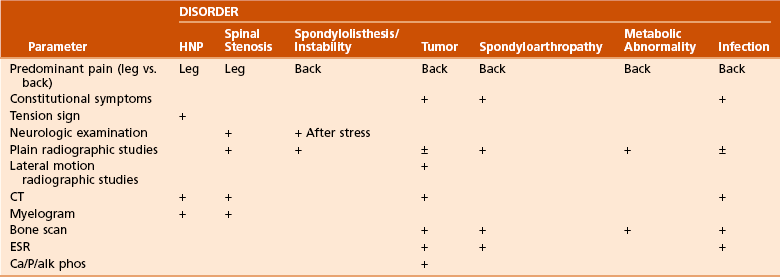
Modified from Weinstein JN, Wiesel SW: The lumbar spine, Philadelphia, 1990, WB Saunders, 1990, p 360.
B Herniated nucleus pulposus (HNP)

 Aging results in loss of water content
Aging results in loss of water content

 Myxomatous changes, resulting in herniation of nuclear material
Myxomatous changes, resulting in herniation of nuclear material

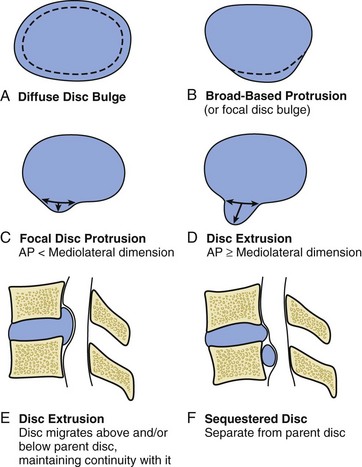
Figure 8-5 Types of disc herniation.





 Relatively uncommon (1% of all surgical HNPs)
Relatively uncommon (1% of all surgical HNPs)
 Typically involves the middle to lower thoracic levels
Typically involves the middle to lower thoracic levels


 Thoracic HNP can be divided into central, posterolateral, and lateral herniations.
Thoracic HNP can be divided into central, posterolateral, and lateral herniations.
 Underlying Scheuermann disease may predispose patients to develop HNP.
Underlying Scheuermann disease may predispose patients to develop HNP.

 Presents as the onset of back or chest pain
Presents as the onset of back or chest pain
 May include radicular symptoms
May include radicular symptoms














 Immobilization, analgesics, and nerve blocks are sometimes helpful for radiculopathy.
Immobilization, analgesics, and nerve blocks are sometimes helpful for radiculopathy.

 Usually performed through an anterior transthoracic approach for midline or central HNP (including anterior discectomy and hemicorpectomy as needed)
Usually performed through an anterior transthoracic approach for midline or central HNP (including anterior discectomy and hemicorpectomy as needed)
 Transpedicular approach for lateral HNP
Transpedicular approach for lateral HNP
 Indicated in the presence of myelopathy or persistent, unremitting radicular pain
Indicated in the presence of myelopathy or persistent, unremitting radicular pain



 Introduction—A major cause of morbidity with a major financial impact in the United States, this disc disease:
Introduction—A major cause of morbidity with a major financial impact in the United States, this disc disease:
 Usually involves the L4 to L5 disc (the “backache disc”), followed closely by L5 to S1.
Usually involves the L4 to L5 disc (the “backache disc”), followed closely by L5 to S1.


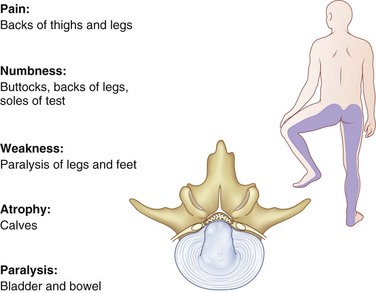
 Central prolapse is often associated with back pain only; however, acute insults may precipitate a cauda equina compression syndrome (Figure 8-7).
Central prolapse is often associated with back pain only; however, acute insults may precipitate a cauda equina compression syndrome (Figure 8-7).





 History of an acute injury or precipitating event should be investigated.
History of an acute injury or precipitating event should be investigated.
 Location of symptoms (especially pain radiating to the extremity)
Location of symptoms (especially pain radiating to the extremity)
 Character of pain—referred pain in mesodermal tissues of the same embryologic origin
Character of pain—referred pain in mesodermal tissues of the same embryologic origin







 Complete review of symptoms (including psychiatric history)
Complete review of symptoms (including psychiatric history)
 The finding of an “inverted-V” triad of hysteria, hypochondriasis, and depression on the Minnesota Multiphasic Personality Inventory has been identified as a significant adverse risk factor for lumbar disc surgery.
The finding of an “inverted-V” triad of hysteria, hypochondriasis, and depression on the Minnesota Multiphasic Personality Inventory has been identified as a significant adverse risk factor for lumbar disc surgery.
 Psychosocial evaluation, pain drawings, and psychological testing are helpful in some cases.
Psychosocial evaluation, pain drawings, and psychological testing are helpful in some cases.



 Physical examination should include:
Physical examination should include:
 Observation (change in posture, gait)
Observation (change in posture, gait)
 Palpation of the posterior spine (spasm, localized tenderness)
Palpation of the posterior spine (spasm, localized tenderness)
 Measurement of range of motion (decreased flexion)
Measurement of range of motion (decreased flexion)

 Vascular evaluation (distal pulses)
Vascular evaluation (distal pulses)
 Abdominal (bruits and pulsatile masses) and rectal examination
Abdominal (bruits and pulsatile masses) and rectal examination
 Neurologic evaluation (see Figure 8-1)
Neurologic evaluation (see Figure 8-1)
 Tension signs such as straight-leg raising or the bowstring sign (L4-L5 or L5-S1) and the femoral nerve stretch test (L2-L3 or L3-L4) are critical findings that suggest HNP and are important when discectomy is considered.
Tension signs such as straight-leg raising or the bowstring sign (L4-L5 or L5-S1) and the femoral nerve stretch test (L2-L3 or L3-L4) are critical findings that suggest HNP and are important when discectomy is considered.

 A large central disc herniation at one level may impinge on more than one nerve root.
A large central disc herniation at one level may impinge on more than one nerve root.



 Inappropriate signs and symptoms (Waddell) are also important to note.
Inappropriate signs and symptoms (Waddell) are also important to note.













 Indicated before proceeding with special tests to rule out other disorders, such as isthmic defects.
Indicated before proceeding with special tests to rule out other disorders, such as isthmic defects.



 These are effective when used as confirmatory studies.
These are effective when used as confirmatory studies.

 Imaging of neural compression may be improved if combined with myelography.
Imaging of neural compression may be improved if combined with myelography.










 More than half of the patients who seek treatment for low back pain recover in 1 week, and 90% recover within 1 to 3 months.
More than half of the patients who seek treatment for low back pain recover in 1 week, and 90% recover within 1 to 3 months.
 Half of the patients with sciatica recover in 1 month.
Half of the patients with sciatica recover in 1 month.

 Instruction should include avoiding rotation and flexion to avoid the increased disc pressure associated with these activities.
Instruction should include avoiding rotation and flexion to avoid the increased disc pressure associated with these activities.
 Progressive ambulation is successful in returning most patients to their normal function.
Progressive ambulation is successful in returning most patients to their normal function.



 This treatment is followed by back rehabilitation and a fitness program.
This treatment is followed by back rehabilitation and a fitness program.









 Patients with positive study results, neurologic findings, tension signs, and predominantly sciatic symptoms without mitigating psychosocial factors are the best candidates for surgical discectomy.
Patients with positive study results, neurologic findings, tension signs, and predominantly sciatic symptoms without mitigating psychosocial factors are the best candidates for surgical discectomy.
 Standard partial laminotomy and discectomy are the most commonly performed surgical procedures.
Standard partial laminotomy and discectomy are the most commonly performed surgical procedures.


 At 2-year follow-up there were no significant differences in primary outcome measures for operative compared with nonoperative groups.
At 2-year follow-up there were no significant differences in primary outcome measures for operative compared with nonoperative groups.


 Trends favoring surgical intervention in primary outcome measures
Trends favoring surgical intervention in primary outcome measures
 Statistically significant improvement in secondary outcome measures for surgical intervention
Statistically significant improvement in secondary outcome measures for surgical intervention











 Complications—fortunately rare, but can be devastating
Complications—fortunately rare, but can be devastating
 Vascular injury—may occur during attempts at disc removal if curets are allowed to penetrate the anterior longitudinal ligament
Vascular injury—may occur during attempts at disc removal if curets are allowed to penetrate the anterior longitudinal ligament
 Intraoperative pulsatile bleeding due to deep penetration is treated with rapid wound closure, intravenous administration of fluids and blood, repositioning the patient, and a transabdominal approach to find and stop the source of bleeding.
Intraoperative pulsatile bleeding due to deep penetration is treated with rapid wound closure, intravenous administration of fluids and blood, repositioning the patient, and a transabdominal approach to find and stop the source of bleeding.


 Nerve root injury—more common with anomalous nerve roots
Nerve root injury—more common with anomalous nerve roots
 Failed back syndrome—often the result of poor patient selection; other causes include:
Failed back syndrome—often the result of poor patient selection; other causes include:
 Recurrent herniation (usually acute recurrence of signs/symptoms after a 6- to 12-month pain-free interval)
Recurrent herniation (usually acute recurrence of signs/symptoms after a 6- to 12-month pain-free interval)







 Primary repair necessary to avoid the development of a pseudomeningocele or spinal fluid fistula
Primary repair necessary to avoid the development of a pseudomeningocele or spinal fluid fistula
 More common during revision surgery
More common during revision surgery
 Fibrin adhesive sealant may be a useful adjunct for effecting dural closure.
Fibrin adhesive sealant may be a useful adjunct for effecting dural closure.

 If tear is adequately repaired, clinical outcomes are generally unaffected.
If tear is adequately repaired, clinical outcomes are generally unaffected.
 Wound infection (approximately 1% in open discectomy)
Wound infection (approximately 1% in open discectomy)

 Discitis (3-6 weeks postoperatively, with rapid onset of severe back pain)
Discitis (3-6 weeks postoperatively, with rapid onset of severe back pain)



 Cauda equina syndrome—secondary to extruded disc, surgical trauma, and hematoma
Cauda equina syndrome—secondary to extruded disc, surgical trauma, and hematoma



 Back pain greater than leg pain
Back pain greater than leg pain



 MRI reveals decreased signal intensity in the disc space on T2 weighting (dark disc).
MRI reveals decreased signal intensity in the disc space on T2 weighting (dark disc).






 If extended nonoperative treatment has failed and the patient has a positive MRI and discogram, interbody fusion can be performed from either an anterior or a retroperitoneal approach or through a posterior midline (posterior lumbar) or posterior transforaminal lumbar interbody fusion approach.
If extended nonoperative treatment has failed and the patient has a positive MRI and discogram, interbody fusion can be performed from either an anterior or a retroperitoneal approach or through a posterior midline (posterior lumbar) or posterior transforaminal lumbar interbody fusion approach.


 This may be effective in early conditions (<50% loss of disc height) but not in more advanced disease
This may be effective in early conditions (<50% loss of disc height) but not in more advanced disease





D Lumbar segmental instability—present when normal loads produce abnormal spinal motion
 The most common symptom is mechanical back pain, although “dynamic” stenosis can occur, leading to radicular symptoms.
The most common symptom is mechanical back pain, although “dynamic” stenosis can occur, leading to radicular symptoms.

 Degenerative lumbar disc disease is indicated by disc space narrowing.
Degenerative lumbar disc disease is indicated by disc space narrowing.

 Continuing degeneration or facet subluxation may then lead to instability.
Continuing degeneration or facet subluxation may then lead to instability.





 Surgical treatment options do not have clearly defined indications, but posterolateral fusion is the standard treatment.
Surgical treatment options do not have clearly defined indications, but posterolateral fusion is the standard treatment.
 The use of pedicle screw instrumentation is well established, with fusion rates approaching 90% in nonsmokers for one- or two-level fusions.
The use of pedicle screw instrumentation is well established, with fusion rates approaching 90% in nonsmokers for one- or two-level fusions.


 Adjacent-level degeneration can occur in these patients.
Adjacent-level degeneration can occur in these patients.
 In large studies, the rates of symptomatic degeneration at an adjacent spinal level are 15% at 5 years and about 40% at 10 years, with no correlation with the number of levels fused or preoperative degeneration.
In large studies, the rates of symptomatic degeneration at an adjacent spinal level are 15% at 5 years and about 40% at 10 years, with no correlation with the number of levels fused or preoperative degeneration.







 The use of alendronate has been shown to decrease spinal fusion rates in animal models
The use of alendronate has been shown to decrease spinal fusion rates in animal models

E Spinal stenosis (Figure 8-8)
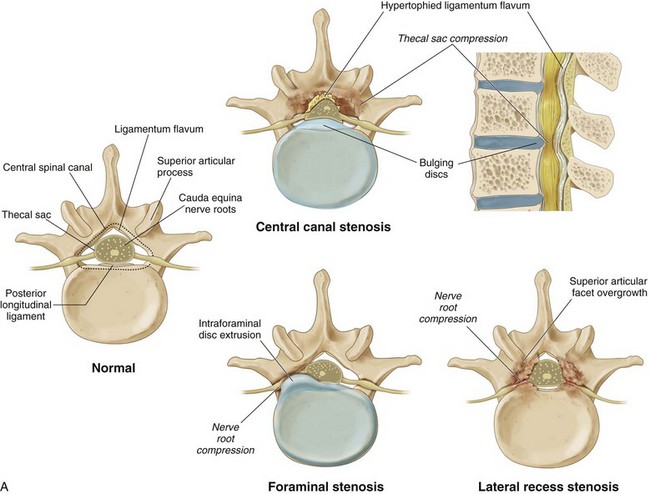
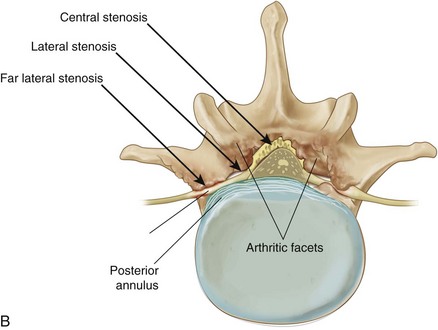
1. Introduction—Spinal stenosis is narrowing of the spinal canal or neural foramina, producing nerve root compression, root ischemia, and a variable syndrome of back and leg pain.
 Central stenosis—thecal sac compression
Central stenosis—thecal sac compression
 The central canal is defined as the space posterior to the posterior longitudinal ligament, anterior to the ligamentum flavum and laminae, and bordered laterally by the medial border of the superior articular process.
The central canal is defined as the space posterior to the posterior longitudinal ligament, anterior to the ligamentum flavum and laminae, and bordered laterally by the medial border of the superior articular process.



 It affects an older population more than lateral recess stenosis does.
It affects an older population more than lateral recess stenosis does.
 Lateral recess stenosis—nerve root compression
Lateral recess stenosis—nerve root compression
 The lateral recess is defined by the superior articular facet posteriorly, the thecal sac medially, the pedicle laterally, and the posterolateral vertebral body anteriorly.
The lateral recess is defined by the superior articular facet posteriorly, the thecal sac medially, the pedicle laterally, and the posterolateral vertebral body anteriorly.

 Foraminal stenosis—nerve root compression
Foraminal stenosis—nerve root compression
 The intervertebral foramen is bordered superiorly and inferiorly by the adjacent level pedicles, posteriorly by the facet joint and lateral extensions of the ligamentum flavum, and anteriorly by the adjacent vertebral bodies and disc.
The intervertebral foramen is bordered superiorly and inferiorly by the adjacent level pedicles, posteriorly by the facet joint and lateral extensions of the ligamentum flavum, and anteriorly by the adjacent vertebral bodies and disc.
 Normal foraminal height is 20 to 30 mm; superior width is 8 to 10 mm.
Normal foraminal height is 20 to 30 mm; superior width is 8 to 10 mm.


 Etiology—congenital versus acquired
Etiology—congenital versus acquired











 Patient history and physical examination
Patient history and physical examination
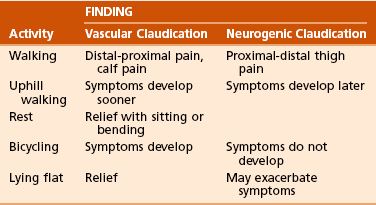
 Symptoms include insidious pain and paresthesias with ambulation or prolonged standing and are relieved by sitting or with flexion of the spine.
Symptoms include insidious pain and paresthesias with ambulation or prolonged standing and are relieved by sitting or with flexion of the spine.
















 Imaging—Further workup may include:
Imaging—Further workup may include:

 Interspace narrowing due to disc degeneration
Interspace narrowing due to disc degeneration

 Flattening of the lordotic curve
Flattening of the lordotic curve
 Subluxation and degenerative changes of the facet joints may also be seen.
Subluxation and degenerative changes of the facet joints may also be seen.







 Electromyography/nerve conduction velocity testing may be used.
Electromyography/nerve conduction velocity testing may be used.





























 Impingement of nerve roots lateral to the thecal sac as they pass through the lateral recess and into the neural foramen
Impingement of nerve roots lateral to the thecal sac as they pass through the lateral recess and into the neural foramen
 Associated with facet joint arthropathy (superior articular process enlargement) and disc disease (Figure 8-8, B)
Associated with facet joint arthropathy (superior articular process enlargement) and disc disease (Figure 8-8, B)















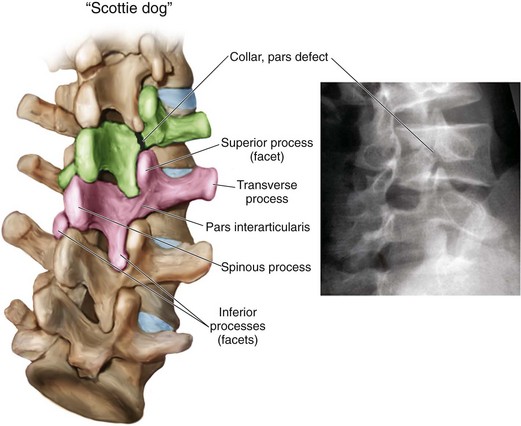
F Spondylolysis and spondylolisthesis
1. Spondylolysis—defect in the pars interarticularis
 One of the most common causes of low back pain in children and adolescents
One of the most common causes of low back pain in children and adolescents
















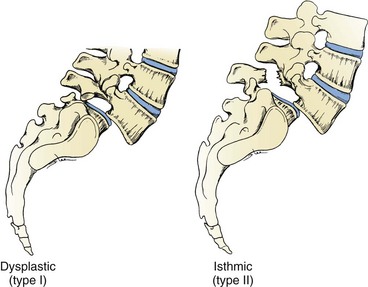
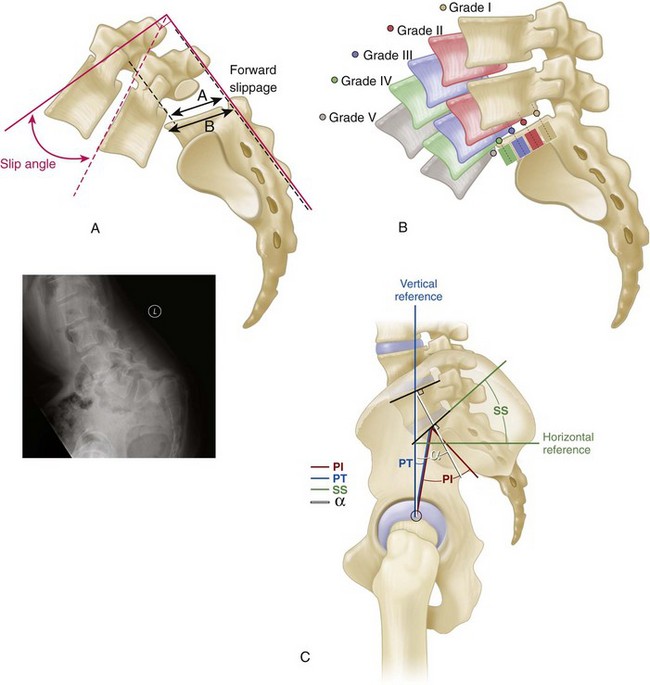
2. Spondylolisthesis—forward slippage of one vertebra on another
 Etiology—six types (Newman, Wiltse, McNab) (Table 8-9; Figures 8-9 and 8-10)
Etiology—six types (Newman, Wiltse, McNab) (Table 8-9; Figures 8-9 and 8-10)
Table 8-9
| Type | Age | Pathology/Other |
| I—Dysplastic | Child | Congenital dysplasia of S1 superior facet |
| II—Isthmic* | 5-50 yr | Predisposition leading to elongation/fracture of pars (L5-S1) |
| III—Degenerative | >40 yr | Facet arthrosis leading to subluxation (L4-L5) |
| IV—Traumatic | Any age | Acute fracture other than pars |
| V—Pathologic | Any age | Incompetence of bony elements |
| VI—Postsurgical | Adult | Excessive resection of neural arches/facets |

 Severity—five grades according to severity (Meyerding); the severity of the slip is based on the amount or degree (compared with S1 width) (Figure 8-11)
Severity—five grades according to severity (Meyerding); the severity of the slip is based on the amount or degree (compared with S1 width) (Figure 8-11)













3. Childhood spondylolisthesis


 Patients with a greater than 25% slip, or with L4-L5 or L3-L4 spondylolisthesis have a higher risk of low back pain than the general population.
Patients with a greater than 25% slip, or with L4-L5 or L3-L4 spondylolisthesis have a higher risk of low back pain than the general population.






 Usually at L5-S1 and typically grade II
Usually at L5-S1 and typically grade II
 Occurs most often in whites, boys, and children who participate in hyperextension activities
Occurs most often in whites, boys, and children who participate in hyperextension activities


 It is thought to result from shear stress at the pars interarticularis and to be associated with repetitive hyperextension.
It is thought to result from shear stress at the pars interarticularis and to be associated with repetitive hyperextension.




 Usually responds to nonoperative treatment consisting of activity modification and exercise
Usually responds to nonoperative treatment consisting of activity modification and exercise
 Adolescents with a grade I slip may return to normal activities, including contact sports, once asymptomatic.
Adolescents with a grade I slip may return to normal activities, including contact sports, once asymptomatic.











 High-grade disease (grades III through V)
High-grade disease (grades III through V)
 These commonly cause neurologic abnormalities.
These commonly cause neurologic abnormalities.

 Prophylactic fusion is recommended in growing children with slippage of more than 50%.
Prophylactic fusion is recommended in growing children with slippage of more than 50%.









4. Degenerative spondylolisthesis

 More common in African Americans, persons with diabetes and women older than age 40
More common in African Americans, persons with diabetes and women older than age 40



 Results in central and lateral recess stenosis with L5 radiculopathy owing to root compression in the lateral recess between the hypertrophic and subluxated inferior facet of L4 and the posterosuperior body of L5
Results in central and lateral recess stenosis with L5 radiculopathy owing to root compression in the lateral recess between the hypertrophic and subluxated inferior facet of L4 and the posterosuperior body of L5


























 Most common site for vertebral column injuries
Most common site for vertebral column injuries
 Although the classification and treatment of these injuries is included in Chapter 11, Trauma, some points need to be emphasized here.
Although the classification and treatment of these injuries is included in Chapter 11, Trauma, some points need to be emphasized here.

 The upper thoracic spine (T1 to T10) is stabilized by the ribs and the facet orientation as well as the sternum and is less susceptible to trauma.
The upper thoracic spine (T1 to T10) is stabilized by the ribs and the facet orientation as well as the sternum and is less susceptible to trauma.









2. Stable versus unstable injuries
 The three-column system (Denis) has been proposed for evaluating spinal injuries and determining which are stable and which unstable.
The three-column system (Denis) has been proposed for evaluating spinal injuries and determining which are stable and which unstable.
 Anterior column—anterior longitudinal ligament and the anterior two thirds of the annulus and vertebral body
Anterior column—anterior longitudinal ligament and the anterior two thirds of the annulus and vertebral body
 Middle column—posterior third of the body and annulus and the posterior longitudinal ligament
Middle column—posterior third of the body and annulus and the posterior longitudinal ligament
 Posterior column—the pedicles, facets, spinous processes, and posterior ligamentous complex
Posterior column—the pedicles, facets, spinous processes, and posterior ligamentous complex









 Fractures with less than 20 to 30 degrees of kyphosis, less than 50% loss of vertebral height, an intact posterior ligamentous column, and no neurologic compromise are usually treated nonoperatively.
Fractures with less than 20 to 30 degrees of kyphosis, less than 50% loss of vertebral height, an intact posterior ligamentous column, and no neurologic compromise are usually treated nonoperatively.
 Thoracolumbar orthosis or casting with serial radiographs to confirm maintenance of acceptable alignment
Thoracolumbar orthosis or casting with serial radiographs to confirm maintenance of acceptable alignment
 Stable burst fractures are best treated nonoperatively.
Stable burst fractures are best treated nonoperatively.

 Rehabilitation after spinal cord injury is discussed more fully in Chapter 10, Rehabilitation: Gait, Amputations, Prostheses, Orthoses, and Neurologic Injury.
Rehabilitation after spinal cord injury is discussed more fully in Chapter 10, Rehabilitation: Gait, Amputations, Prostheses, Orthoses, and Neurologic Injury.









 Respiratory failure is a significant problem for the multiply injured patient with a thoracolumbar fracture.
Respiratory failure is a significant problem for the multiply injured patient with a thoracolumbar fracture.


 Long-term complications of a thoracolumbar fracture, treated with or without surgery, are:
Long-term complications of a thoracolumbar fracture, treated with or without surgery, are:







H Other thoracolumbar disorders
1. Destructive spondyloarthropathy
 Seen in hemodialysis patients with chronic renal failure
Seen in hemodialysis patients with chronic renal failure
 Typically involves three adjacent vertebrae and two intervening discs
Typically involves three adjacent vertebrae and two intervening discs
 Changes include subluxation, degeneration, and narrowing of the disc height.
Changes include subluxation, degeneration, and narrowing of the disc height.
 Although the process may resemble infection, it probably represents crystal or amyloid deposition.
Although the process may resemble infection, it probably represents crystal or amyloid deposition.
2. Diffuse idiopathic skeletal hyperostosis (DISH)—also known as Forestier disease (Figure 8-12)
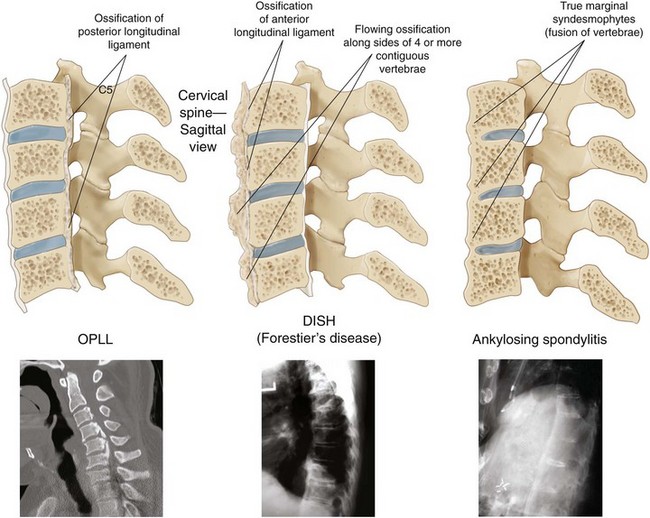

 DISH is defined by the presence of nonmarginal syndesmophytes (differentiated from ankylosing spondylitis, which has marginal syndesmophytes) at three successive levels.
DISH is defined by the presence of nonmarginal syndesmophytes (differentiated from ankylosing spondylitis, which has marginal syndesmophytes) at three successive levels.
 Syndesmophytes are vertical outgrowths that extend across the disc space and represent calcification of the anulus fibrosus and anterior and posterior longitudinal ligaments.
Syndesmophytes are vertical outgrowths that extend across the disc space and represent calcification of the anulus fibrosus and anterior and posterior longitudinal ligaments.

 DISH is associated with chronic low back pain and is more common in patients with diabetes and gout.
DISH is associated with chronic low back pain and is more common in patients with diabetes and gout.
 The prevalence of DISH has been found to be as high as 28% in autopsy specimens.
The prevalence of DISH has been found to be as high as 28% in autopsy specimens.

3. Ankylosing spondylitis (see Figure 8-12)
 95% of patients with ankylosing spondylitis are positive for human leukocyte antigen–B27 (HLA-B27)
95% of patients with ankylosing spondylitis are positive for human leukocyte antigen–B27 (HLA-B27)


 Bamboo spine is the descriptive term applied to multiple vertebral levels ankylosed by marginal syndesmophytes.
Bamboo spine is the descriptive term applied to multiple vertebral levels ankylosed by marginal syndesmophytes.
 May result in fixed kyphotic deformities leading to sagittal imbalance
May result in fixed kyphotic deformities leading to sagittal imbalance
 Extension osteotomy and fusion of the lumbar spine with compression instrumentation can successfully balance the head over the sacrum.
Extension osteotomy and fusion of the lumbar spine with compression instrumentation can successfully balance the head over the sacrum.
 Assessment of the patient for hip flexion contractures or cervicothoracic kyphosis is mandatory.
Assessment of the patient for hip flexion contractures or cervicothoracic kyphosis is mandatory.
 The cervical spine may be corrected by a C7 to T1 osteotomy and fusion under local anesthesia.
The cervical spine may be corrected by a C7 to T1 osteotomy and fusion under local anesthesia.






 Usually defined as scoliosis in patients older than age 20, it is more symptomatic than its childhood counterpart (see Chapter 3, Pediatric Orthopaedics).
Usually defined as scoliosis in patients older than age 20, it is more symptomatic than its childhood counterpart (see Chapter 3, Pediatric Orthopaedics).









 Association between pain and scoliosis in the adult is controversial.
Association between pain and scoliosis in the adult is controversial.
 Progression of symptoms to side of curve convexity indicates poor prognosis.
Progression of symptoms to side of curve convexity indicates poor prognosis.
 Lumbar stenosis, in particular in the concavity of the curve
Lumbar stenosis, in particular in the concavity of the curve
 Cosmetic deformity may be present.
Cosmetic deformity may be present.

 Myelography with CT or MRI is useful for the evaluation of nerve root compression in stenosis.
Myelography with CT or MRI is useful for the evaluation of nerve root compression in stenosis.
 MRI, facet injections, and/or discography may be used to evaluate symptoms in the lumbar spine.
MRI, facet injections, and/or discography may be used to evaluate symptoms in the lumbar spine.

 There is no demonstrated association between curve progression and pregnancy.
There is no demonstrated association between curve progression and pregnancy.




 Uncertain correlation between adult scoliosis and back pain makes conservative management essential.
Uncertain correlation between adult scoliosis and back pain makes conservative management essential.



 Young adults (<30 years) with curves of greater than 50 to 60 degrees
Young adults (<30 years) with curves of greater than 50 to 60 degrees
 Older patients with refractory pain
Older patients with refractory pain
 Sagittal plane imbalance is a strong predictor of disability.
Sagittal plane imbalance is a strong predictor of disability.


















 Nonsurgically treated adults with late-onset idiopathic scoliosis are highly productive at 50-year follow-up, with a slightly increased risk of shortness of breath with activity and chief complaints of back pain and poor cosmesis.
Nonsurgically treated adults with late-onset idiopathic scoliosis are highly productive at 50-year follow-up, with a slightly increased risk of shortness of breath with activity and chief complaints of back pain and poor cosmesis.
 Operative risk for these patients is high (up to a 25% complication rate in older patients).
Operative risk for these patients is high (up to a 25% complication rate in older patients).














2. Nontraumatic adult kyphosis
 Severe idiopathic or congenital kyphosis may be a source of back pain in the adult, particularly when it is present in the thoracolumbar or lumbar spine.
Severe idiopathic or congenital kyphosis may be a source of back pain in the adult, particularly when it is present in the thoracolumbar or lumbar spine.


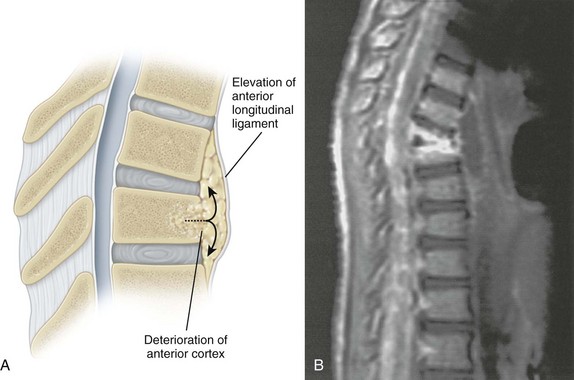
 Present after fractures of the thoracolumbar spine treated without surgery, particularly in setting of posterior ligamentous complex injury
Present after fractures of the thoracolumbar spine treated without surgery, particularly in setting of posterior ligamentous complex injury










 An underlying malignancy as a cause of the osteopenia should be considered; evaluation with MRI is sensitive for determining the presence of tumor.
An underlying malignancy as a cause of the osteopenia should be considered; evaluation with MRI is sensitive for determining the presence of tumor.

 Surgical attempts at correction and stabilization are marked by a high complication rate.
Surgical attempts at correction and stabilization are marked by a high complication rate.
 Vertebroplasty and kyphoplasty
Vertebroplasty and kyphoplasty
 Percutaneous techniques designed to relieve pain and correct deformity (kyphoplasty)
Percutaneous techniques designed to relieve pain and correct deformity (kyphoplasty)
 Indicated for subacute injuries, although precise indications are poorly defined
Indicated for subacute injuries, although precise indications are poorly defined


 Kyphoplasty has also been proposed to correct deformity.
Kyphoplasty has also been proposed to correct deformity.
 Improvement in pain and quality of life has been questioned in recent studies.
Improvement in pain and quality of life has been questioned in recent studies.






















V TUMORS AND INFECTIONS OF THE SPINE
A Introduction—The spine is a frequent site of metastasis, and certain tumors with a predilection for the spine have unique manifestations in vertebrae.
1. Tumors of the vertebral body







2. Tumors of the posterior elements include















B Metastasis—the most common tumors of the spine, spreading to the vertebral body first and later to the pedicles









 A poor prognosis is associated with neurologic dysfunction, proximal lesions, long duration of symptoms, and rapid growth of the metastasis.
A poor prognosis is associated with neurologic dysfunction, proximal lesions, long duration of symptoms, and rapid growth of the metastasis.

 Radiation therapy and chemotherapy have traditionally been the mainstays of treatment unless the tumor is destabilizing and progressive or causes spinal cord or cauda equina dysfunction.
Radiation therapy and chemotherapy have traditionally been the mainstays of treatment unless the tumor is destabilizing and progressive or causes spinal cord or cauda equina dysfunction.







 Progressive neurologic dysfunction that is unresponsive to radiation therapy
Progressive neurologic dysfunction that is unresponsive to radiation therapy
 Persistent pain despite radiation therapy
Persistent pain despite radiation therapy





 Vertebroplasty is gaining favor in cases of metastatic disease of the spine (myeloma, breast) without instability or neurologic compromise and represents a minimally invasive alternative to open surgery.
Vertebroplasty is gaining favor in cases of metastatic disease of the spine (myeloma, breast) without instability or neurologic compromise and represents a minimally invasive alternative to open surgery.




 Bone grafting is preferred if life expectancy is more than 6 months.
Bone grafting is preferred if life expectancy is more than 6 months.
 Metastatic renal cell carcinoma requires preoperative arteriography and embolism.
Metastatic renal cell carcinoma requires preoperative arteriography and embolism.
1. Osteoid osteoma and osteoblastoma



























 Usually seen in children younger than age 10 years
Usually seen in children younger than age 10 years
 More common in the thoracic spine
More common in the thoracic spine
 May present with progressive back pain
May present with progressive back pain

 Biopsy may be required for diagnosis unless the radiographic picture is classic.
Biopsy may be required for diagnosis unless the radiographic picture is classic.

 Symptoms are usually self-limiting.
Symptoms are usually self-limiting.
 Chemotherapy is useful for the systemic form.
Chemotherapy is useful for the systemic form.
 Bracing may be indicated in children to prevent progressive kyphosis.
Bracing may be indicated in children to prevent progressive kyphosis.
 Low-dose radiation therapy may be indicated in the presence of neurologic deficits.
Low-dose radiation therapy may be indicated in the presence of neurologic deficits.
 At least 50% reconstitution of vertebral height may be expected.
At least 50% reconstitution of vertebral height may be expected.







6. Plasmacytoma/multiple myeloma










 Slow-growing lytic lesion in the midline of the anterior sacrum or the base of the skull
Slow-growing lytic lesion in the midline of the anterior sacrum or the base of the skull
 It may occur in other vertebrae (cervical spine most common).
It may occur in other vertebrae (cervical spine most common).
 Patients with these tumors may present with intra-abdominal complaints and a presacral mass.
Patients with these tumors may present with intra-abdominal complaints and a presacral mass.







 Arises in the posterior elements and is frequently seen in the cervical spine
Arises in the posterior elements and is frequently seen in the cervical spine
 Treatment is by excision, which may be necessary to rule out sarcomatous changes.
Treatment is by excision, which may be necessary to rule out sarcomatous changes.






























2. Pyogenic vertebral osteomyelitis

 Seen with increasing frequency but still associated with a significant (6- to 12-week) delay in diagnosis
Seen with increasing frequency but still associated with a significant (6- to 12-week) delay in diagnosis

 Patient history and physical examination
Patient history and physical examination



 Organism usually hematogenous (S. aureus, 50%-75% of cases)
Organism usually hematogenous (S. aureus, 50%-75% of cases)
 Fungal spondylitis can be seen in patients with immunologic compromise.
Fungal spondylitis can be seen in patients with immunologic compromise.





 Paraspinous soft tissue swelling (loss of a psoas shadow)
Paraspinous soft tissue swelling (loss of a psoas shadow)
 Erosion of the vertebral end plates
Erosion of the vertebral end plates
 Disc destruction (disc space preserved in metastatic disease)
Disc destruction (disc space preserved in metastatic disease)




 Tissue diagnosis via blood cultures or aspirate of the infection is mandatory.
Tissue diagnosis via blood cultures or aspirate of the infection is mandatory.










 Back pain is the most common presenting symptom, followed by neurologic deficit and fever. Nevertheless, diagnosis is delayed in half of patients
Back pain is the most common presenting symptom, followed by neurologic deficit and fever. Nevertheless, diagnosis is delayed in half of patients
 Risk factors include intravenous drug abuse, diabetes and multiple medical problems.
Risk factors include intravenous drug abuse, diabetes and multiple medical problems.
 Erythrocyte sedimentation rate and C-reactive protein values are elevated.
Erythrocyte sedimentation rate and C-reactive protein values are elevated.







4. Spinal tuberculosis (Figure 8-13)






 On early plain radiographs, anterior vertebral body destruction, with preservation of the disc, distinguishes tuberculosis from pyogenic infection.
On early plain radiographs, anterior vertebral body destruction, with preservation of the disc, distinguishes tuberculosis from pyogenic infection.

 Severe kyphosis, sinus formation, and (Pott) paraplegia are late sequelae.
Severe kyphosis, sinus formation, and (Pott) paraplegia are late sequelae.


 Chemotherapy is the mainstay of treatment.
Chemotherapy is the mainstay of treatment.






 Advantages include less progressive kyphosis, earlier healing, and a decrease in sinus formation.
Advantages include less progressive kyphosis, earlier healing, and a decrease in sinus formation.
 Adjuvant chemotherapy beginning 10 days before surgery is recommended.
Adjuvant chemotherapy beginning 10 days before surgery is recommended.