Basic Sciences
I. Histologic Features of Bone
III. Conditions of Bone Mineralization, Bone Mineral Density, and Bone Viability
SECTION 3 NEUROMUSCULAR AND CONNECTIVE TISSUES
SECTION 4 CELLULAR AND MOLECULAR BIOLOGY, IMMUNOLOGY, AND GENETICS OF ORTHOPAEDICS
SECTION 5 ORTHOPAEDIC INFECTIONS AND MICROBIOLOGY
SECTION 6 PERIOPERATIVE PROBLEMS
SECTION 7 IMAGING AND SPECIAL STUDIES
section 1 Bone
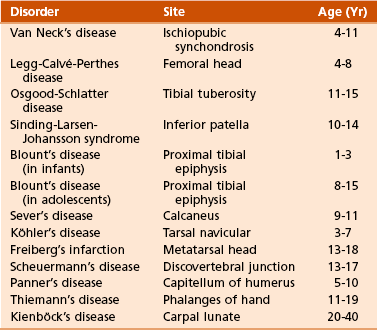
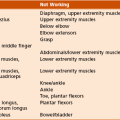
A Types (Figure 1-1; Table 1-1)
Table 1-1
Modified from Brinker MR, Miller MD: Fundamentals of orthopaedics, Philadelphia, 1999, WB Saunders, p 1.
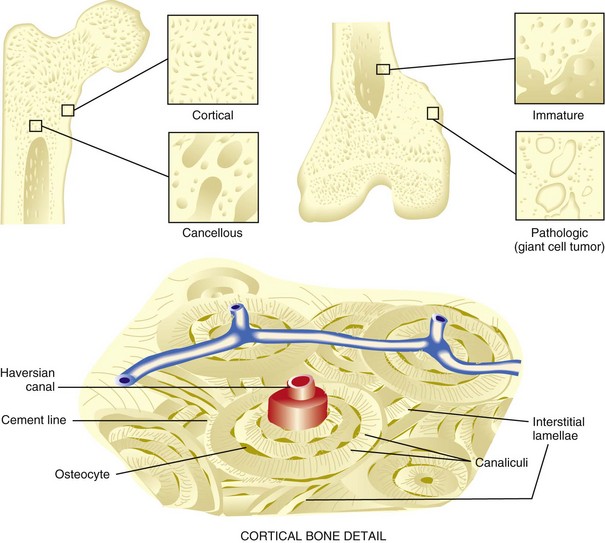
1. Normal bone: lamellar, either cortical or cancellous
2. Immature and pathologic bone: woven; more random, more osteocytes, increased turnover, weaker

 Constitutes 80% of the skeleton
Constitutes 80% of the skeleton
 Consists of tightly packed osteons or haversian systems
Consists of tightly packed osteons or haversian systems
 Connected by Haversian (or Volkmann’s) canals
Connected by Haversian (or Volkmann’s) canals
 Contains arterioles, venules, capillaries, nerves, possibly lymphatic channels
Contains arterioles, venules, capillaries, nerves, possibly lymphatic channels
 Interstitial lamellae: between osteons
Interstitial lamellae: between osteons



 Nutrition provided by intraosseous circulation
Nutrition provided by intraosseous circulation

 Characterized by slow turnover rate, higher Young’s modulus of elasticity, more stiffness
Characterized by slow turnover rate, higher Young’s modulus of elasticity, more stiffness


B Cellular biology (Figure 1-2)
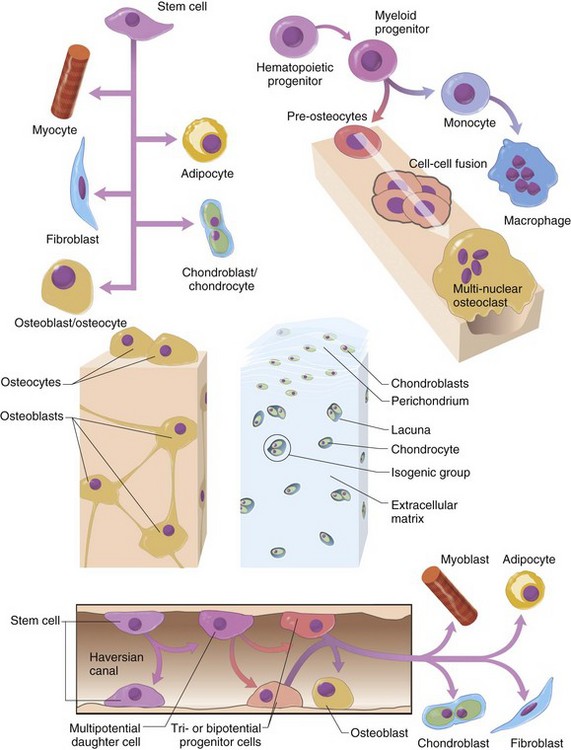
 Form bone by generating organic, nonmineralized matrix
Form bone by generating organic, nonmineralized matrix

 Derived from undifferentiated mesenchymal stem cells
Derived from undifferentiated mesenchymal stem cells
 Have more endoplasmic reticulum, Golgi apparatus, and mitochondria than do other cells (for synthesis and secretion of matrix)
Have more endoplasmic reticulum, Golgi apparatus, and mitochondria than do other cells (for synthesis and secretion of matrix)

 Bone surfaces lined by more differentiated, metabolically active cells
Bone surfaces lined by more differentiated, metabolically active cells
 “Entrapped cells”: less active cells in “resting regions”; maintain the ionic milieu of bone
“Entrapped cells”: less active cells in “resting regions”; maintain the ionic milieu of bone

 Osteoblast differentiation in vivo effected by the following:
Osteoblast differentiation in vivo effected by the following:



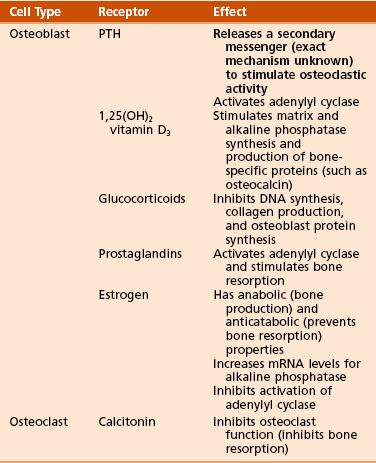
 Receptor-effector interactions in osteoblasts (Table 1-2)
Receptor-effector interactions in osteoblasts (Table 1-2)
 Osteoblasts produce the following:
Osteoblasts produce the following:





 Osteoblast activity stimulated by intermittent (pulsatile) exposure to parathyroid hormone (PTH)
Osteoblast activity stimulated by intermittent (pulsatile) exposure to parathyroid hormone (PTH)
 Osteoblast activity inhibited by tumor necrosis factor-α (TNF-α)
Osteoblast activity inhibited by tumor necrosis factor-α (TNF-α)




2. Osteocytes (see Figure 1-1)

 Constitute 90% of the cells in the mature skeleton
Constitute 90% of the cells in the mature skeleton


 Long interconnecting cytoplasmic processes projecting through the canaliculi
Long interconnecting cytoplasmic processes projecting through the canaliculi
 Less active in matrix production than are osteoblasts
Less active in matrix production than are osteoblasts
 Important for control of extracellular calcium and phosphorus concentration
Important for control of extracellular calcium and phosphorus concentration


 This activity occurs both normally and in certain conditions, including multiple myeloma and metastatic bone disease.
This activity occurs both normally and in certain conditions, including multiple myeloma and metastatic bone disease.
 Multinucleated, irregular giant cells
Multinucleated, irregular giant cells


 Possess a ruffled (“brush”) border and surrounding clear zone
Possess a ruffled (“brush”) border and surrounding clear zone

 Bone resorption occurs in depressions: Howship’s lacunae
Bone resorption occurs in depressions: Howship’s lacunae


 Osteoblasts (and tumor cells) express RANKL (Figure 1-3), which acts as follows:
Osteoblasts (and tumor cells) express RANKL (Figure 1-3), which acts as follows:
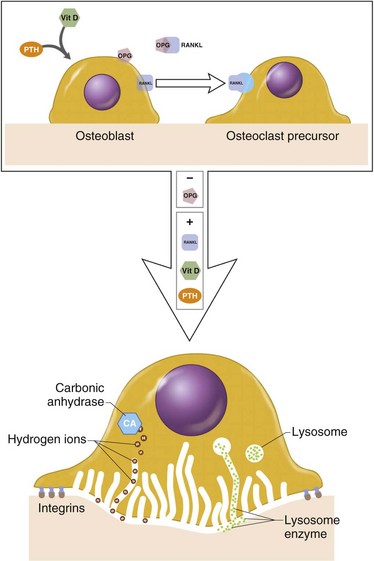




 Synthesize tartrate-resistant acid phosphate
Synthesize tartrate-resistant acid phosphate
 Bind to bone surfaces through cell attachment (anchoring) proteins
Bind to bone surfaces through cell attachment (anchoring) proteins


 Produce hydrogen ions through carbonic anhydrase
Produce hydrogen ions through carbonic anhydrase



 Have specific receptors for calcitonin
Have specific receptors for calcitonin


 Potent stimulator of osteoclast differentiation and bone resorption
Potent stimulator of osteoclast differentiation and bone resorption



 Inhibit osteoclastic bone resorption.
Inhibit osteoclastic bone resorption.

 Categorized into two classes on the basis of presence or absence of a nitrogen side group
Categorized into two classes on the basis of presence or absence of a nitrogen side group
 Nitrogen-containing bisphosphonates are up to 1000-fold more potent in their antiresorptive activity.
Nitrogen-containing bisphosphonates are up to 1000-fold more potent in their antiresorptive activity.
 Nitrogen-containing bisphosphonates
Nitrogen-containing bisphosphonates



 Non–nitrogen-containing bisphosphonates
Non–nitrogen-containing bisphosphonates

 Decreases skeletal events in multiple myeloma
Decreases skeletal events in multiple myeloma
 Associated with osteonecrosis of the jaw
Associated with osteonecrosis of the jaw















Table 1-3
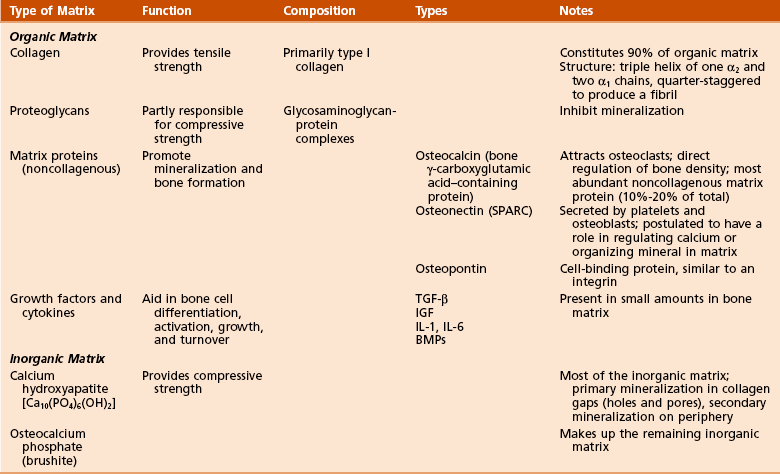
1. Organic components: 40% of the dry weight of bone
 Collagen (90% of organic component)
Collagen (90% of organic component)
 Collagen is primarily type I (mnemonic: “bone” contains the word “one”).
Collagen is primarily type I (mnemonic: “bone” contains the word “one”).
 Hole zones (gaps) exist within the collagen fibril between the ends of molecules.
Hole zones (gaps) exist within the collagen fibril between the ends of molecules.
 Pores exist between the sides of parallel molecules.
Pores exist between the sides of parallel molecules.
 Mineral deposition (calcification) occurs within the hole zones and pores (Figure 1-4).
Mineral deposition (calcification) occurs within the hole zones and pores (Figure 1-4).
 Cross-linking decreases collagen solubility and increases its tensile strength.
Cross-linking decreases collagen solubility and increases its tensile strength.

 Matrix proteins (noncollagenous)
Matrix proteins (noncollagenous)




2. Inorganic (mineral) components: 60% of the dry weight of bone


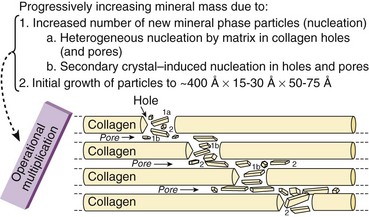
 Cortical and cancellous bone is continuously remodeled throughout life by osteoclastic and osteoblastic activity (Figure 1-5).
Cortical and cancellous bone is continuously remodeled throughout life by osteoclastic and osteoblastic activity (Figure 1-5).
 Wolff’s law: Remodeling occurs in response to mechanical stress.
Wolff’s law: Remodeling occurs in response to mechanical stress.


 Piezoelectric remodeling occurs in response to electrical charge.
Piezoelectric remodeling occurs in response to electrical charge.













 Bone receives 5% to 10% of the cardiac output.
Bone receives 5% to 10% of the cardiac output.

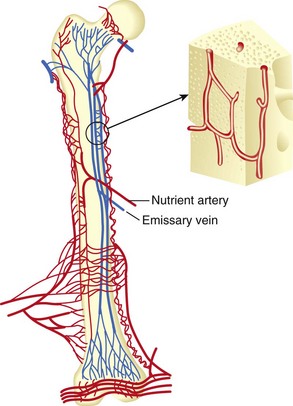
 Long bones receive blood from three sources (systems):
Long bones receive blood from three sources (systems):

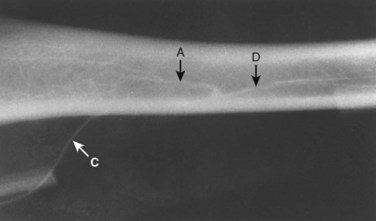
 Nutrient arteries branch from systemic arteries, enter the diaphyseal cortex through the nutrient foramen, enter the medullary canal, and branch into ascending and descending arteries (Figure 1-7).
Nutrient arteries branch from systemic arteries, enter the diaphyseal cortex through the nutrient foramen, enter the medullary canal, and branch into ascending and descending arteries (Figure 1-7).
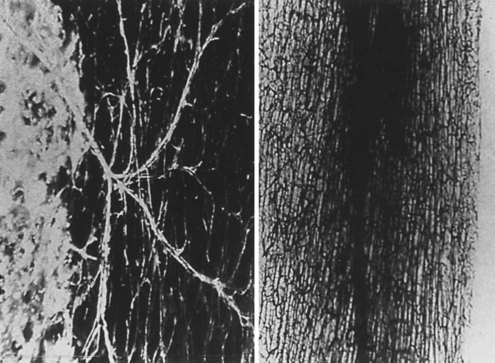
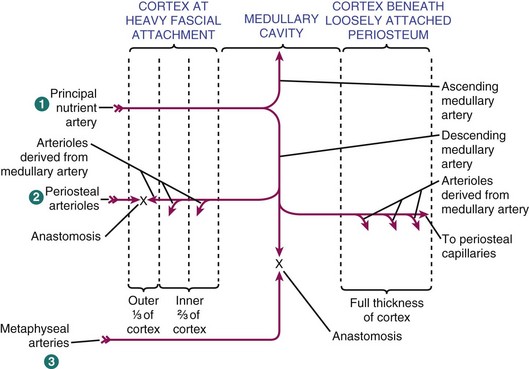
 Further branching into arterioles in the endosteal cortex enables blood supply to at least the inner two thirds of the mature diaphyseal cortex via the Haversian system (Figures 1-8 and 1-9).
Further branching into arterioles in the endosteal cortex enables blood supply to at least the inner two thirds of the mature diaphyseal cortex via the Haversian system (Figures 1-8 and 1-9).









































G Types of bone formation (Table 1-4)
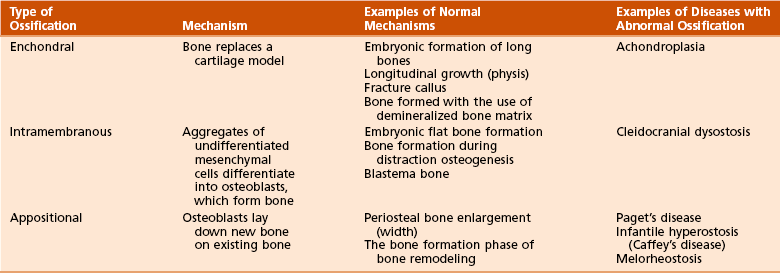
1. Enchondral bone formation and mineralization

 Undifferentiated cells secrete the cartilaginous matrix and differentiate into chondrocytes.
Undifferentiated cells secrete the cartilaginous matrix and differentiate into chondrocytes.
 The matrix mineralizes and is invaded by vascular buds that bring osteoprogenitor cells.
The matrix mineralizes and is invaded by vascular buds that bring osteoprogenitor cells.
 Osteoclasts resorb calcified cartilage, and osteoblasts form bone.
Osteoclasts resorb calcified cartilage, and osteoblasts form bone.
 Bone replaces the cartilage model; cartilage is not converted to bone.
Bone replaces the cartilage model; cartilage is not converted to bone.





 Embryonic formation of long bones (Figures 1-11 and 1-12)
Embryonic formation of long bones (Figures 1-11 and 1-12)
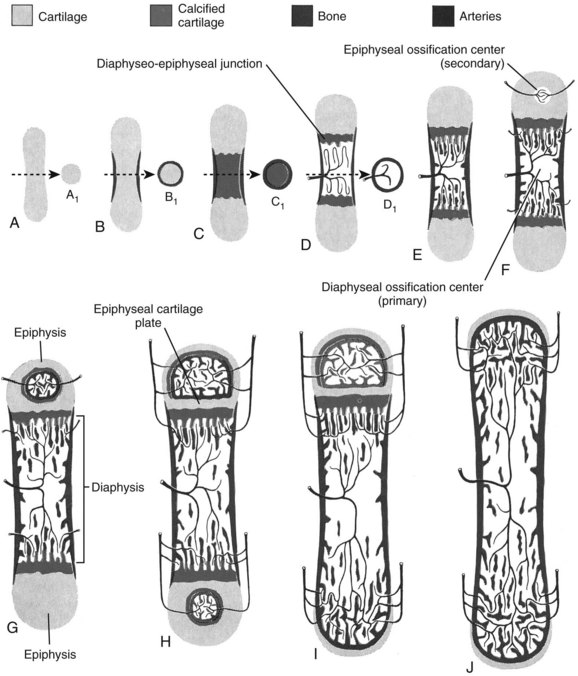
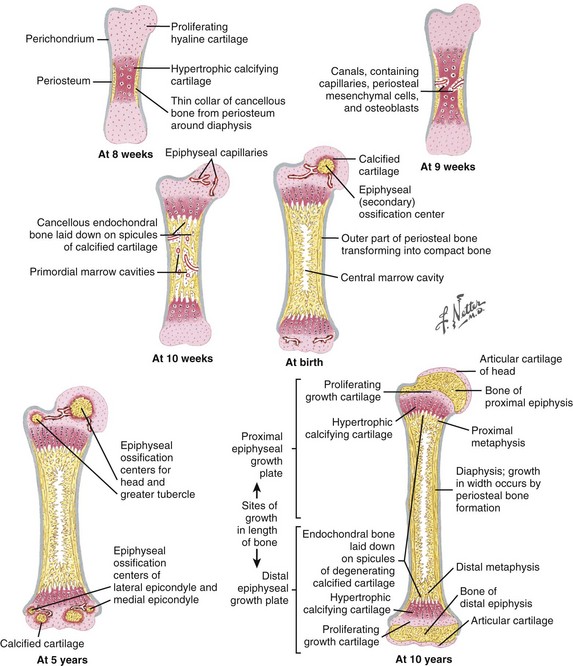
 These bones are formed from the mesenchymal anlage, at 6 weeks of gestation.
These bones are formed from the mesenchymal anlage, at 6 weeks of gestation.


 The cartilage model increases in size through appositional (width) and interstitial (length) growth.
The cartilage model increases in size through appositional (width) and interstitial (length) growth.


 Arterial supply is rich during development, with an epiphyseal artery (terminates in the proliferative zone), metaphyseal arteries, nutrient arteries, and perichondrial arteries (Figure 1-13).
Arterial supply is rich during development, with an epiphyseal artery (terminates in the proliferative zone), metaphyseal arteries, nutrient arteries, and perichondrial arteries (Figure 1-13).
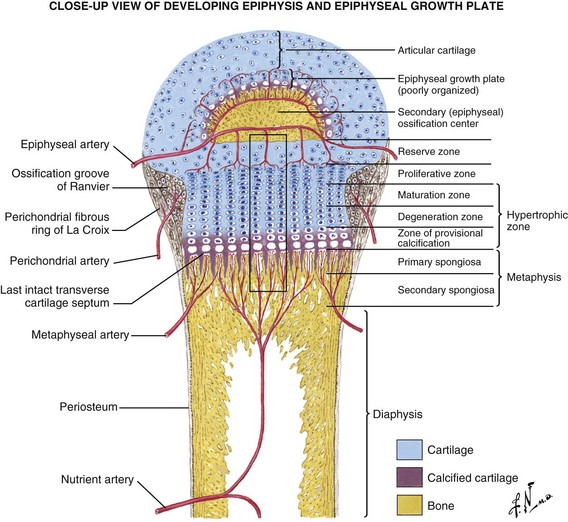


 Two growth plates exist in immature long bones: (1) horizontal (the physis) and (2) spherical (growth of the epiphysis).
Two growth plates exist in immature long bones: (1) horizontal (the physis) and (2) spherical (growth of the epiphysis).

 The perichondrial artery is the major source of nutrition of the growth plate.
The perichondrial artery is the major source of nutrition of the growth plate.

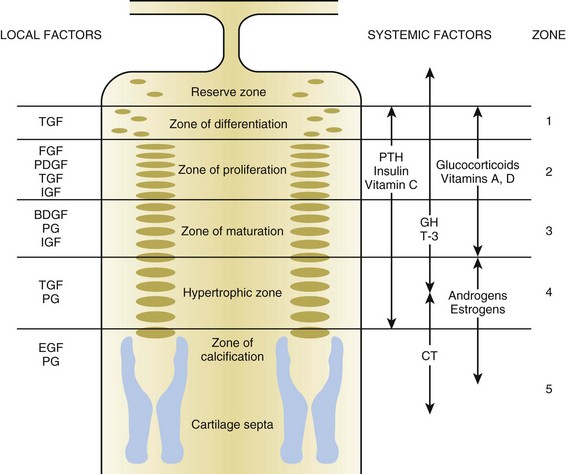
 Delineation of physeal cartilage zones is based on growth (see Figure 1-13) and function (Figures 1-14 and 1-15).
Delineation of physeal cartilage zones is based on growth (see Figure 1-13) and function (Figures 1-14 and 1-15).
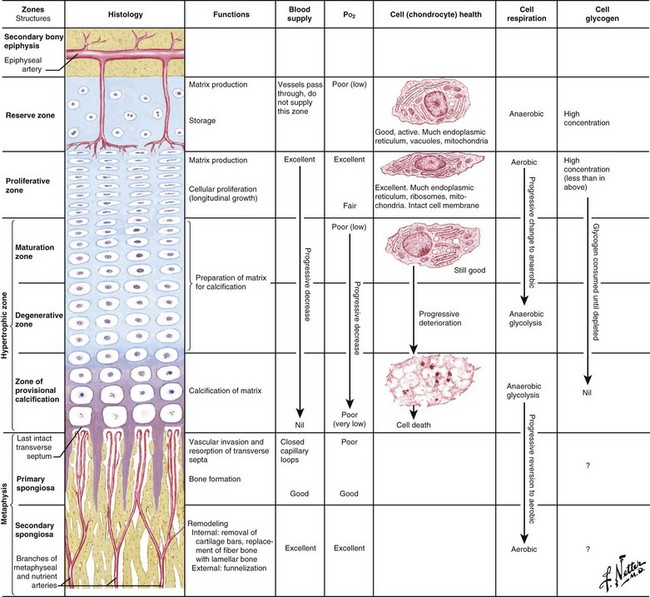


 Reserve zone: Cells store lipids, glycogen, and proteoglycan aggregates; decreased oxygen tension occurs in this zone.
Reserve zone: Cells store lipids, glycogen, and proteoglycan aggregates; decreased oxygen tension occurs in this zone.





 Normal matrix mineralization occurs in the lower hypertrophic zone: chondrocytes increase five times in size, accumulate calcium in their mitochondria, die, and release calcium from matrix vesicles.
Normal matrix mineralization occurs in the lower hypertrophic zone: chondrocytes increase five times in size, accumulate calcium in their mitochondria, die, and release calcium from matrix vesicles.

 Osteoblasts migrate from sinusoidal vessels and use cartilage as a scaffolding for bone formation.
Osteoblasts migrate from sinusoidal vessels and use cartilage as a scaffolding for bone formation.

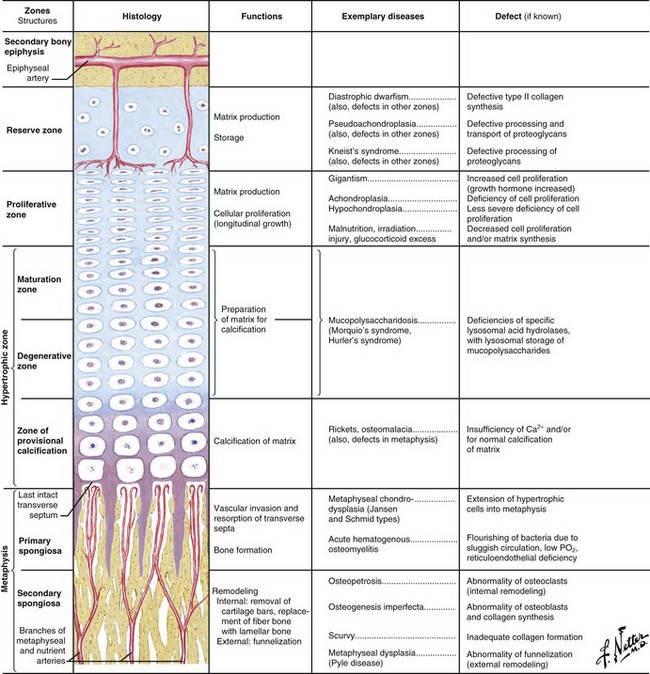
 This zone widens in rickets (see Figure 1-15), with little or no provisional calcification.
This zone widens in rickets (see Figure 1-15), with little or no provisional calcification.

 Mucopolysaccharide diseases (see Figure 1-15) affect this zone, leading to chondrocyte degeneration.
Mucopolysaccharide diseases (see Figure 1-15) affect this zone, leading to chondrocyte degeneration.
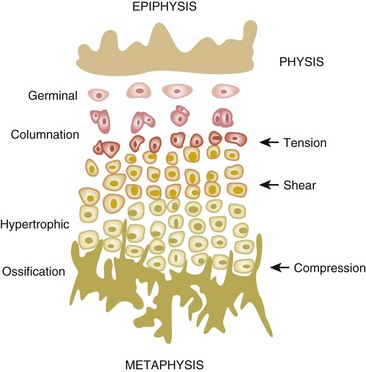
 Physeal fractures probably traverse several zones, depending on the type of loading (Figure 1-16).
Physeal fractures probably traverse several zones, depending on the type of loading (Figure 1-16).


 This is adjacent to the physis and expands with skeletal growth.
This is adjacent to the physis and expands with skeletal growth.
 Osteoblasts from osteoprogenitor cells align on cartilage bars produced by physeal expansion.
Osteoblasts from osteoprogenitor cells align on cartilage bars produced by physeal expansion.






 Collagen hole zones are seeded with calcium hydroxyapatite crystals through branching and accretion (crystal growth).
Collagen hole zones are seeded with calcium hydroxyapatite crystals through branching and accretion (crystal growth).
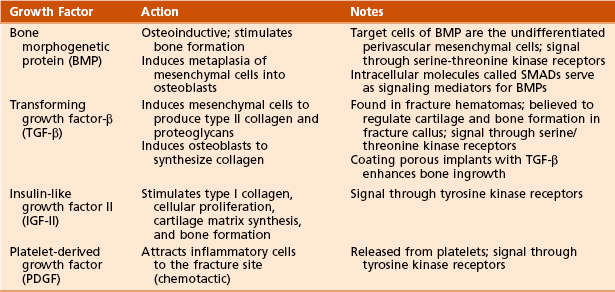
 Hormones and growth factors (Figure 1-17; Table 1-5)
Hormones and growth factors (Figure 1-17; Table 1-5)
Table 1-5
Effects of Hormones and Growth Factors on the Growth Plate
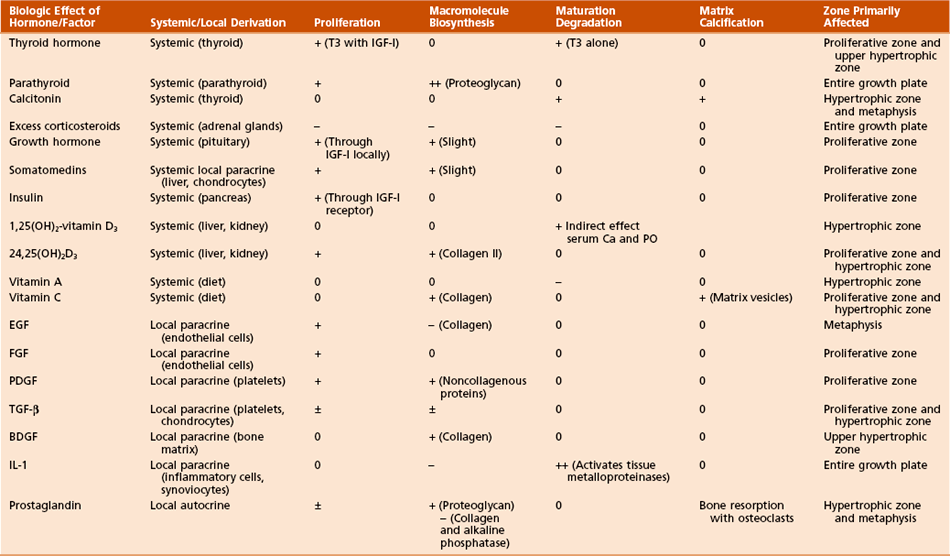
From Simon SR, editor: Orthopaedic basic science, ed 2, Rosemont, Ill, 1994, American Academy of Orthopaedic Surgeons, p 196.










1. A Continuum: inflammation to repair (soft callus followed by hard callus) ending in remodeling
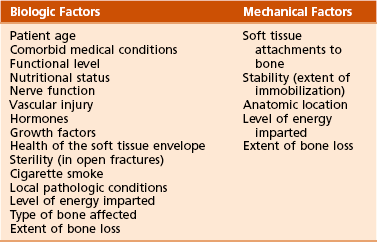
2. Blood supply (bone blood flow): the most important factor

 Bleeding creates a hematoma, which provides hematopoietic cells capable of secreting growth factors.
Bleeding creates a hematoma, which provides hematopoietic cells capable of secreting growth factors.

 Osteoblasts from surrounding osteogenic precursor cells and fibroblasts proliferate.
Osteoblasts from surrounding osteogenic precursor cells and fibroblasts proliferate.

 Primary callus response within 2 weeks.
Primary callus response within 2 weeks.
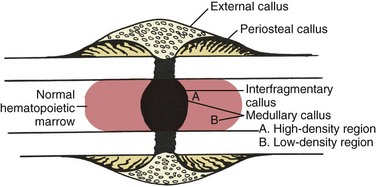
 For bone ends not in continuity, bridging (soft) callus occurs.
For bone ends not in continuity, bridging (soft) callus occurs.
 Soft callus is later replaced through enchondral ossification by woven bone (hard callus).
Soft callus is later replaced through enchondral ossification by woven bone (hard callus).
 Medullary callus supplements the bridging callus, forming more slowly and later (Figure 1-18).
Medullary callus supplements the bridging callus, forming more slowly and later (Figure 1-18).

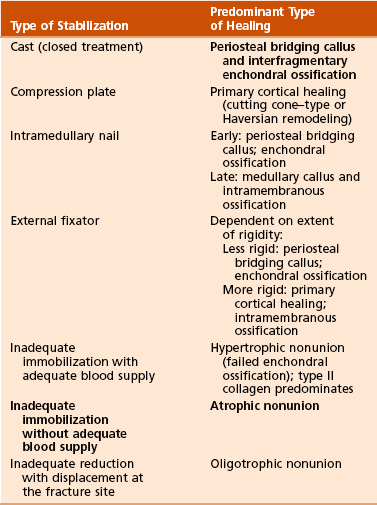











4. Biochemistry of fracture healing (Table 1-8)
Table 1-8
Biochemical Steps of Fracture Healing
| Step | Collagen Type |
| Mesenchymal | I, II, III, V |
| Chondroid | II, IX |
| Chondroid-osteoid | I, II, X |
| Osteogenic | I |
5. Growth factors of bone (Table 1-9)



6. Endocrine effects on fracture healing (Table 1-10)
Table 1-10
Endocrine Effects on Fracture Healing
| Hormone | Effect | Mechanism |
| Cortisone | − | Decreased callus proliferation |
| Calcitonin | +? | Unknown |
| TH, PTH | + | Bone remodeling |
| Growth hormone | + | Increased callus volume |

 Increases time to fracture healing
Increases time to fracture healing
 Increases nonunion risk (particularly in the tibia)
Increases nonunion risk (particularly in the tibia)
 Decreases fracture callus strength
Decreases fracture callus strength
 Increases pseudarthrosis risk after lumbar fusion up to 500%
Increases pseudarthrosis risk after lumbar fusion up to 500%
9. Nonsteroidal anti-inflammatory drugs (NSAIDs)



11. Ultrasonography and fracture healing
 Low-intensity pulsed ultrasonography accelerates fracture healing and increases the mechanical strength of callus.
Low-intensity pulsed ultrasonography accelerates fracture healing and increases the mechanical strength of callus.
 A cellular response to the mechanical energy of ultrasonography has been postulated.
A cellular response to the mechanical energy of ultrasonography has been postulated.
12. Effect of radiation on bone
 High-dose irradiation causes long-term changes within the haversian system and decreases cellularity.
High-dose irradiation causes long-term changes within the haversian system and decreases cellularity.
 Protein malnutrition results in negative effects in fracture healing:
Protein malnutrition results in negative effects in fracture healing:
















Table 1-11
Types of Bone Grafts and Bone Graft Properties
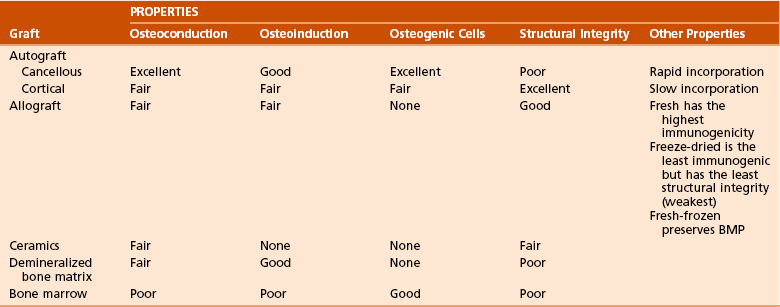
BMP, bone morphogenetic protein.
Modified from Brinker MR, Miller MD: Fundamentals of orthopaedics, Philadelphia, 1999, WB Saunders, p 7.
 Osteoconductive matrix: acts as a scaffold or framework for bone growth
Osteoconductive matrix: acts as a scaffold or framework for bone growth
 Osteoinductive factors: growth factors (BMP) that stimulate bone formation
Osteoinductive factors: growth factors (BMP) that stimulate bone formation
 Osteogenic cells: primitive mesenchymal cells, osteoblasts, and osteocytes
Osteogenic cells: primitive mesenchymal cells, osteoblasts, and osteocytes

 Autografts (from same person) or allografts (from another person)
Autografts (from same person) or allografts (from another person)

 Cortical bone: slower to turn over; used for structural defects
Cortical bone: slower to turn over; used for structural defects
 Osteoarticular (osteochondral) allograft used for tumor surgery
Osteoarticular (osteochondral) allograft used for tumor surgery







 Fresh: increased immunogenicity
Fresh: increased immunogenicity
 Fresh-frozen: less immunogenic than fresh; BMP preserved
Fresh-frozen: less immunogenic than fresh; BMP preserved



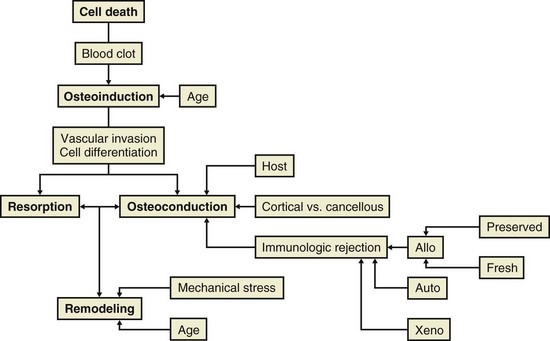
 Allograft bone possesses a spectrum of potential antigens, primarily from cell surface glycoproteins.
Allograft bone possesses a spectrum of potential antigens, primarily from cell surface glycoproteins.
 Classes I and II cellular antigens in allograft are recognized by T lymphocytes in the host.
Classes I and II cellular antigens in allograft are recognized by T lymphocytes in the host.
 Primary mechanism of rejection is cellular, as opposed to humoral.
Primary mechanism of rejection is cellular, as opposed to humoral.



 Extracellular matrix components that contribute to antigenicity are as follows:
Extracellular matrix components that contribute to antigenicity are as follows:



4. Five Stages of graft healing (Urist) (Table 1-12)
Table 1-12
| Stage | Activity |
| 1: Inflammation | Chemotaxis stimulated by necrotic debris |
| 2: Osteoblast differentiation | From precursors |
| 3: Osteoinduction | Osteoblast and osteoclast function |
| 4: Osteoconduction | New bone forming over scaffold |
| 5: Remodeling | Process continues for years |


 Slower incorporation: remodels existing haversian systems through resorption (weakens the graft) and then deposits new bone (restores strength)
Slower incorporation: remodels existing haversian systems through resorption (weakens the graft) and then deposits new bone (restores strength)
 Resorption confined to osteon borders; interstitial lamellae are preserved
Resorption confined to osteon borders; interstitial lamellae are preserved

 Of massive grafts, 25% eventually sustain insufficiency fracture
Of massive grafts, 25% eventually sustain insufficiency fracture
















C Distraction osteogenesis (Figure 1-20)
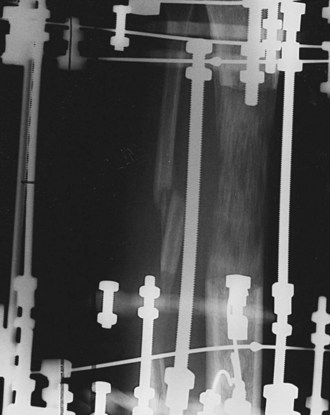
1. Definition: distraction-stimulated formation of bone




 Under optimal stability, intramembranous ossification occurs.
Under optimal stability, intramembranous ossification occurs.
 Under instability, bone forms through enchondral ossification.
Under instability, bone forms through enchondral ossification.





4. Optimal conditions during distraction osteogenesis:
 Low-energy corticotomy/osteotomy
Low-energy corticotomy/osteotomy
 Minimal soft tissue stripping at the corticotomy site (preserves blood supply)
Minimal soft tissue stripping at the corticotomy site (preserves blood supply)
 Stable external fixation and elimination of torsion, shear, and bending moments
Stable external fixation and elimination of torsion, shear, and bending moments
 Latency period (no lengthening) 5 to 7 days
Latency period (no lengthening) 5 to 7 days
 Distraction: 0.25 mm three or four times per day (0.75 to 1.0 mm per day)
Distraction: 0.25 mm three or four times per day (0.75 to 1.0 mm per day)
 Neutral fixation interval (no distraction) during consolidation
Neutral fixation interval (no distraction) during consolidation
 Normal physiologic use of the extremity, including weight bearing
Normal physiologic use of the extremity, including weight bearing
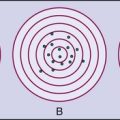
1. Ectopic bone forms in soft tissues.


2. Traumatic brain injury increases risk of heterotopic ossification.
 Recurrence after resection is likely if neurologic compromise is severe.
Recurrence after resection is likely if neurologic compromise is severe.
 The timing of surgery for heterotopic ossification after traumatic brain injury is important:
The timing of surgery for heterotopic ossification after traumatic brain injury is important:


3. Heterotopic ossification may be resected after total hip arthroplasty (THA).
 Resection should be delayed for 6 months or longer after THA.
Resection should be delayed for 6 months or longer after THA.
 Adjuvant radiation therapy may prevent recurrence of heterotopic ossification.
Adjuvant radiation therapy may prevent recurrence of heterotopic ossification.


4. Preoperative radiation (600 to 800 rad) may be used in treatment.


5. When oral bisphosphonate therapy is discontinued, heterotopic ossification may occur.


III CONDITIONS OF BONE MINERALIZATION, BONE MINERAL DENSITY, AND BONE VIABILITY
 Important in muscle and nerve function, clotting, and many other areas
Important in muscle and nerve function, clotting, and many other areas
 >99% of the body’s calcium is stored in bones.
>99% of the body’s calcium is stored in bones.
 Plasma calcium is about equally free and bound (usually to albumin).
Plasma calcium is about equally free and bound (usually to albumin).
 Approximately 400 mg of calcium is released from bone daily.
Approximately 400 mg of calcium is released from bone daily.
 Absorbed in the duodenum by active transport
Absorbed in the duodenum by active transport


 Absorbed in the jejunum by passive diffusion
Absorbed in the jejunum by passive diffusion
 The kidney reabsorbs 98% of calcium (60% in the proximal tubule).
The kidney reabsorbs 98% of calcium (60% in the proximal tubule).

 The primary homeostatic regulators of serum calcium are PTH and 1,25(OH)2-vitamin D3
The primary homeostatic regulators of serum calcium are PTH and 1,25(OH)2-vitamin D3
 Dietary requirement of elemental calcium:
Dietary requirement of elemental calcium:
 Approximately 600 mg/day for children
Approximately 600 mg/day for children
 Approximately 1300 mg/day for adolescents and young adults (ages 10 to 25 years)
Approximately 1300 mg/day for adolescents and young adults (ages 10 to 25 years)
 750 mg/day for adults (ages 25 to 65 years)
750 mg/day for adults (ages 25 to 65 years)
 1500 mg/day for pregnant women
1500 mg/day for pregnant women
 2000 mg/day for lactating women
2000 mg/day for lactating women
 1500 mg/day for postmenopausal women and for patients with a healing fracture in a long bone
1500 mg/day for postmenopausal women and for patients with a healing fracture in a long bone

 A key component of bone mineral
A key component of bone mineral


 Also important in enzyme systems and molecular interactions
Also important in enzyme systems and molecular interactions





 PTH is an 84–amino acid peptide.
PTH is an 84–amino acid peptide.
 It is synthesized in and secreted from the chief cells of the (four) parathyroid glands.
It is synthesized in and secreted from the chief cells of the (four) parathyroid glands.
 The N-terminal fragment 1-34 is the active portion.
The N-terminal fragment 1-34 is the active portion.
 Teriparatide, the synthetic form of recombinant human PTH, contains this active sequence.
Teriparatide, the synthetic form of recombinant human PTH, contains this active sequence.
 The effect of PTH is mediated by the cAMP second-messenger mechanism.
The effect of PTH is mediated by the cAMP second-messenger mechanism.
 PTH helps regulate plasma calcium.
PTH helps regulate plasma calcium.
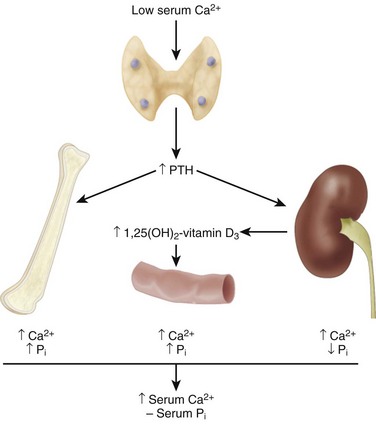
 Decreased calcium levels in the extracellular fluid stimulate β2 receptors to release PTH, which acts at the intestines, kidneys, and bones (Table 1-13).
Decreased calcium levels in the extracellular fluid stimulate β2 receptors to release PTH, which acts at the intestines, kidneys, and bones (Table 1-13).
Table 1-13
Regulation of Calcium and Phosphate Metabolism
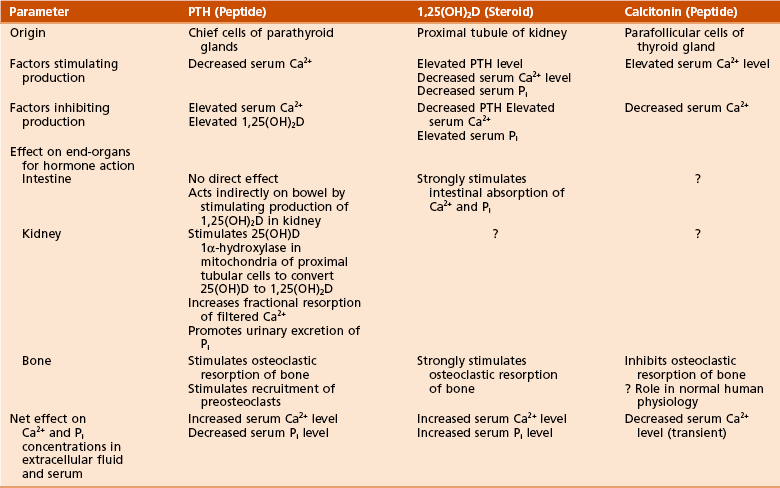
Adapted from Netter FH: CIBA collection of medical illustrations, vol 8: Musculoskeletal system, part I: Anatomy, physiology and developmental disorders, Basel, Switzerland, 1987, CIBA, p 179.
 PTH directly activates osteoblasts.
PTH directly activates osteoblasts.
 PTH modulates renal phosphate filtration.
PTH modulates renal phosphate filtration.
 PTH may accentuate bone loss in elderly persons.
PTH may accentuate bone loss in elderly persons.
 PTH-related protein and its receptor have been implicated in metaphyseal dysplasia.
PTH-related protein and its receptor have been implicated in metaphyseal dysplasia.


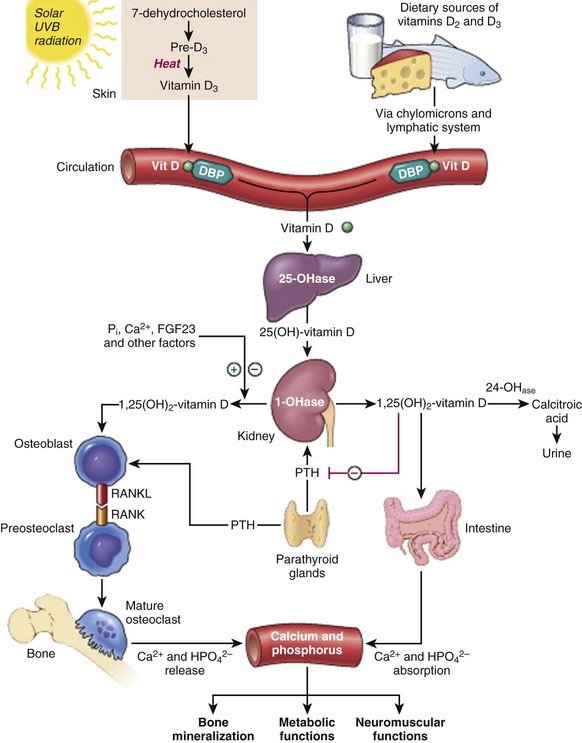



 1,25(OH)2-vitamin D3 works at the intestines, kidneys, and bones (see Table 1-13).
1,25(OH)2-vitamin D3 works at the intestines, kidneys, and bones (see Table 1-13).

 A 32–amino acid peptide hormone
A 32–amino acid peptide hormone

 Has a limited role in calcium regulation (see Table 1-13)
Has a limited role in calcium regulation (see Table 1-13)
 Increased extracellular calcium levels cause secretion of calcitonin
Increased extracellular calcium levels cause secretion of calcitonin






6. Other hormones affecting bone metabolism

 Estrogen prevents bone loss by inhibiting bone resorption.
Estrogen prevents bone loss by inhibiting bone resorption.

 Because bone formation and resorption are coupled, estrogen therapy also decreases bone formation.
Because bone formation and resorption are coupled, estrogen therapy also decreases bone formation.





















 Calcium and phosphate metabolism
Calcium and phosphate metabolism

 Feedback mechanisms: important in the regulation of plasma levels of calcium and phosphate
Feedback mechanisms: important in the regulation of plasma levels of calcium and phosphate



 After peak, bone loss occurs at a rate of 0.3% to 0.5% per year
After peak, bone loss occurs at a rate of 0.3% to 0.5% per year
 Rate of bone loss is 2% to 3% per year in untreated women during the sixth through tenth years after menopause.
Rate of bone loss is 2% to 3% per year in untreated women during the sixth through tenth years after menopause.





 Occurs at the onset of menopause, when both bone formation and resorption are accelerated
Occurs at the onset of menopause, when both bone formation and resorption are accelerated
 A net negative change in calcium balance: menopause decreases intestinal absorption and increases urinary excretion of calcium
A net negative change in calcium balance: menopause decreases intestinal absorption and increases urinary excretion of calcium
 Both urinary hydroxyproline and pyridinoline cross-links are elevated when bone resorption occurs.
Both urinary hydroxyproline and pyridinoline cross-links are elevated when bone resorption occurs.
 Serum alkaline phosphatase level is elevated when bone formation is increased.
Serum alkaline phosphatase level is elevated when bone formation is increased.
 Estrogen therapy is recommended for patients at high risk for osteoporosis.
Estrogen therapy is recommended for patients at high risk for osteoporosis.



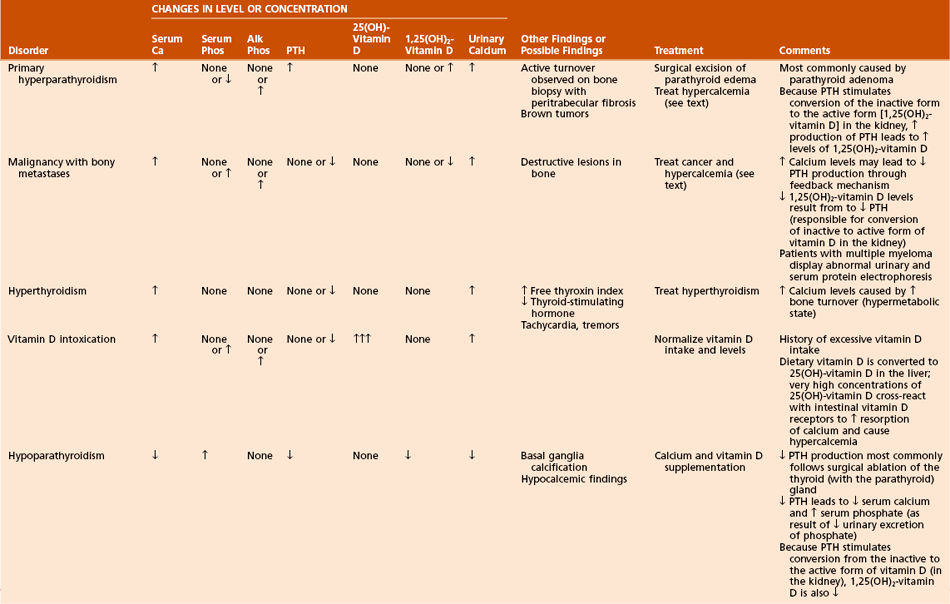
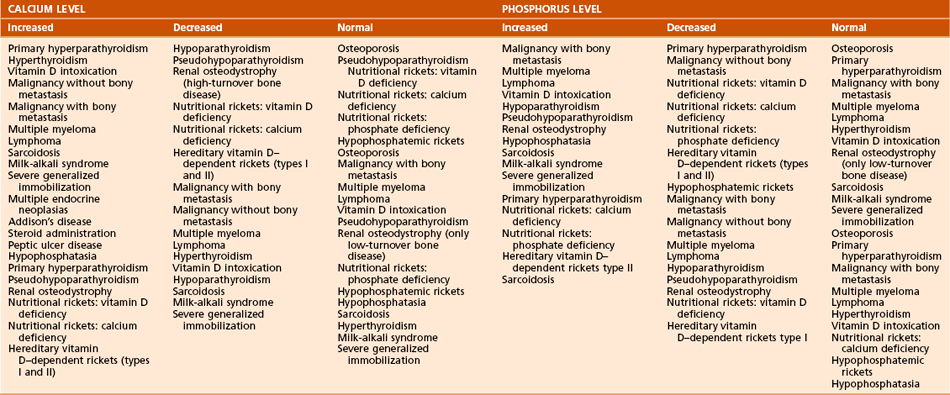
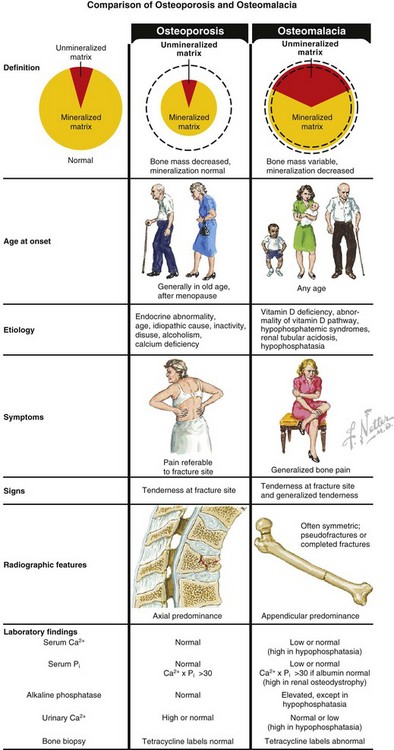
B Conditions of bone mineralization (Tables 1-14 through 1-16)
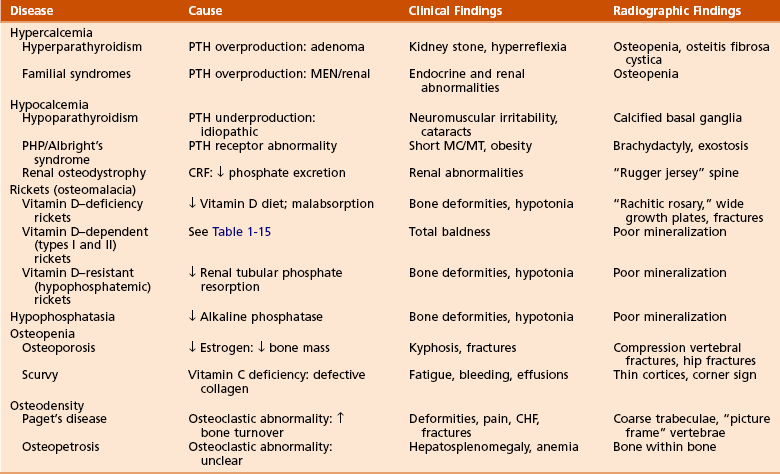
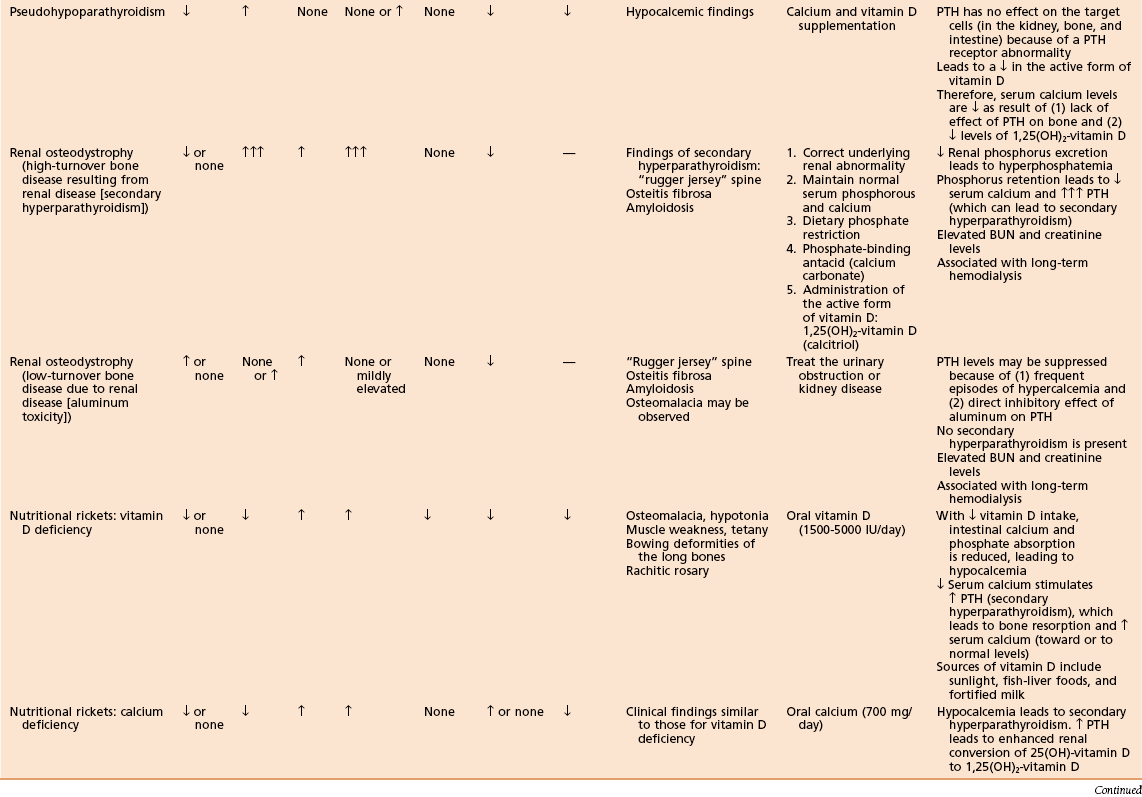
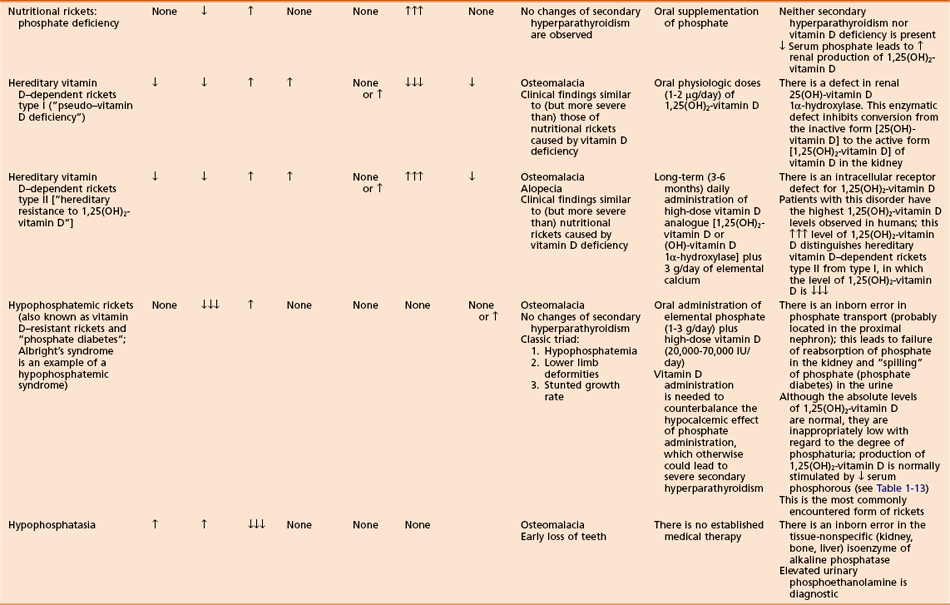
Table 1-15
Laboratory Findings and Clinical Data Regarding Patients with Various Metabolic Bone Diseases
 Can manifest in a number of ways:
Can manifest in a number of ways:



 Excessive bony resorption with or without fibrotic tissue replacement (osteitis fibrosa cystica)
Excessive bony resorption with or without fibrotic tissue replacement (osteitis fibrosa cystica)
 Central nervous system (CNS) effects (confusion, stupor, weakness)
Central nervous system (CNS) effects (confusion, stupor, weakness)

 Can also cause anorexia, nausea, vomiting, dehydration, and muscle weakness
Can also cause anorexia, nausea, vomiting, dehydration, and muscle weakness

 Overproduction of PTH, usually a result of a parathyroid adenoma
Overproduction of PTH, usually a result of a parathyroid adenoma










 Osteitis fibrosa cystica (fibrous replacement of marrow)
Osteitis fibrosa cystica (fibrous replacement of marrow)
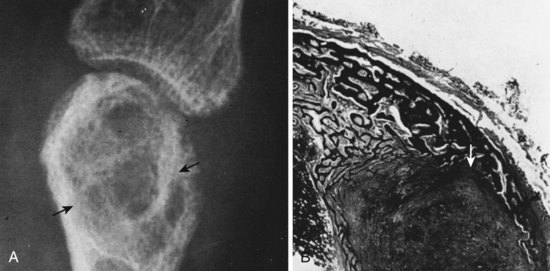
 “Brown tumors” (Figure 1-23): increased giant cells, extravasation of RBCs, hemosiderin staining, fibrous tissue hemosiderin
“Brown tumors” (Figure 1-23): increased giant cells, extravasation of RBCs, hemosiderin staining, fibrous tissue hemosiderin




















 Can be life-threatening, commonly associated with muscle weakness
Can be life-threatening, commonly associated with muscle weakness
 Initial treatment should include hydration with normal saline (reverses dehydration).
Initial treatment should include hydration with normal saline (reverses dehydration).


 PTH-related protein secretion (lung carcinoma)
PTH-related protein secretion (lung carcinoma)
 Lytic bone metastases and lesions (such as multiple myeloma)
Lytic bone metastases and lesions (such as multiple myeloma)
















 Results from low levels of PTH or vitamin D3
Results from low levels of PTH or vitamin D3


 Decreased PTH level causes decrease in plasma calcium level and increase in plasma phosphate level.
Decreased PTH level causes decrease in plasma calcium level and increase in plasma phosphate level.





 Skull radiographs may show basal ganglia calcification.
Skull radiographs may show basal ganglia calcification.
 Iatrogenic hypoparathyroidism most commonly follows thyroidectomy.
Iatrogenic hypoparathyroidism most commonly follows thyroidectomy.
 Pseudohypoparathyroidism (PHP)
Pseudohypoparathyroidism (PHP)



 PTH action is blocked by an abnormality at the receptor, by the cAMP system, or by a lack of required cofactors (e.g., Mg2+).
PTH action is blocked by an abnormality at the receptor, by the cAMP system, or by a lack of required cofactors (e.g., Mg2+).









 Renal osteodystrophy (Figure 1-25)
Renal osteodystrophy (Figure 1-25)
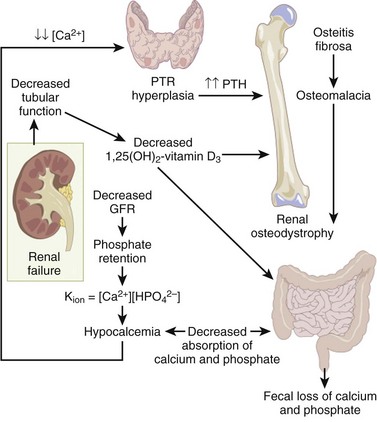
 A spectrum of bone mineral metabolism disorders in chronic renal disease
A spectrum of bone mineral metabolism disorders in chronic renal disease
 Renal disease impairs excretion and compromises mineral homeostasis.
Renal disease impairs excretion and compromises mineral homeostasis.
 This process leads to abnormalities in bone mineral metabolism.
This process leads to abnormalities in bone mineral metabolism.
 High-turnover renal bone disease
High-turnover renal bone disease
 Chronically elevated serum PTH level leads to secondary hyperparathyroidism (hyperplasia of the chief cells of the parathyroid gland).
Chronically elevated serum PTH level leads to secondary hyperparathyroidism (hyperplasia of the chief cells of the parathyroid gland).

 Diminished renal phosphorus excretion; phosphorus retention promotes PTH secretion by three mechanisms:
Diminished renal phosphorus excretion; phosphorus retention promotes PTH secretion by three mechanisms:
 Hyperphosphatemia lowers serum calcium, stimulating PTH.
Hyperphosphatemia lowers serum calcium, stimulating PTH.
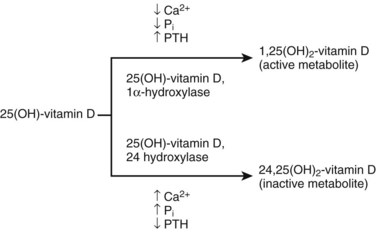
 Phosphorus impairs renal 1α-hydroxylase activity, impairing production of 1,25(OH)2-vitamin D3.
Phosphorus impairs renal 1α-hydroxylase activity, impairing production of 1,25(OH)2-vitamin D3.
 Phosphorus retention may directly increase the synthesis of PTH.
Phosphorus retention may directly increase the synthesis of PTH.

 Impaired renal calcitriol [1,25(OH)2-vitamin D3]
Impaired renal calcitriol [1,25(OH)2-vitamin D3]
 Alterations in the control of PTH gene transcription secretion
Alterations in the control of PTH gene transcription secretion

 Low-turnover renal bone disease (adynamic lesion of bone and osteomalacia)
Low-turnover renal bone disease (adynamic lesion of bone and osteomalacia)
 Secondary hyperparathyroidism is not characteristic with this condition.
Secondary hyperparathyroidism is not characteristic with this condition.










 β2-microglobulin may accumulate with chronic dialysis, leading to amyloidosis
β2-microglobulin may accumulate with chronic dialysis, leading to amyloidosis
 Amyloidosis may be associated with carpal tunnel syndrome, arthropathy, and pathologic fractures.
Amyloidosis may be associated with carpal tunnel syndrome, arthropathy, and pathologic fractures.
 In amyloidosis, Congo red stain causes material to turn pink.
In amyloidosis, Congo red stain causes material to turn pink.






 Rickets (osteomalacia in adults; Box 1-1)
Rickets (osteomalacia in adults; Box 1-1)
 Failure of mineralization, leading to changes in the physis in the zone of provisional calcification (increased width and disorientation) and bone (cortical thinning, bowing)
Failure of mineralization, leading to changes in the physis in the zone of provisional calcification (increased width and disorientation) and bone (cortical thinning, bowing)
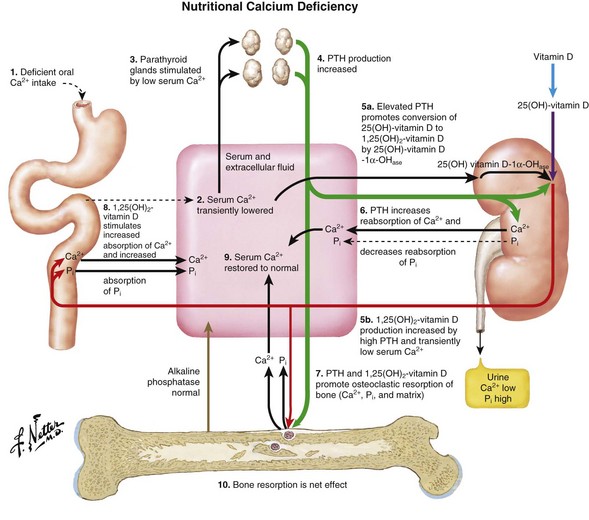
 Nutritional rickets (see Table 1-15)
Nutritional rickets (see Table 1-15)

 Rare after addition of vitamin D to milk, except in the following populations:
Rare after addition of vitamin D to milk, except in the following populations:





 Decreased intestinal absorption of calcium and phosphate leads to secondary hyperparathyroidism
Decreased intestinal absorption of calcium and phosphate leads to secondary hyperparathyroidism

 Low-normal calcium level (maintained by high PTH level)
Low-normal calcium level (maintained by high PTH level)
 Low phosphate level (excreted because of the effect of PTH)
Low phosphate level (excreted because of the effect of PTH)





 Enlargement of the costochondral junction (“rachitic rosary”)
Enlargement of the costochondral junction (“rachitic rosary”)



 Pathologic fractures (Looser’s zones: pseudofracture on the compression side of bone)
Pathologic fractures (Looser’s zones: pseudofracture on the compression side of bone)








 In affected children, height is commonly below the fifth percentile for age.
In affected children, height is commonly below the fifth percentile for age.
 Treatment with vitamin D (5000 IU daily) resolves most deformities.
Treatment with vitamin D (5000 IU daily) resolves most deformities.


 Hereditary vitamin D–dependent rickets
Hereditary vitamin D–dependent rickets
 Rare disorders with features similar to vitamin D deficiency (nutritional) rickets, except that symptoms may be worse and patients may have total baldness
Rare disorders with features similar to vitamin D deficiency (nutritional) rickets, except that symptoms may be worse and patients may have total baldness




 Familial hypophosphatemic rickets (vitamin D–resistant rickets or “phosphate diabetes”)
Familial hypophosphatemic rickets (vitamin D–resistant rickets or “phosphate diabetes”)















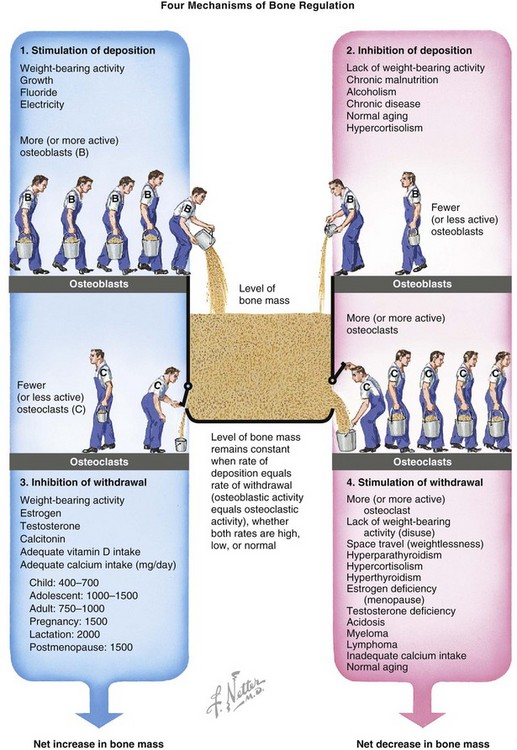
3. Conditions of bone mineral density
 Bone mass is regulated by relative rates of deposition and withdrawal (Figure 1-29).
Bone mass is regulated by relative rates of deposition and withdrawal (Figure 1-29).

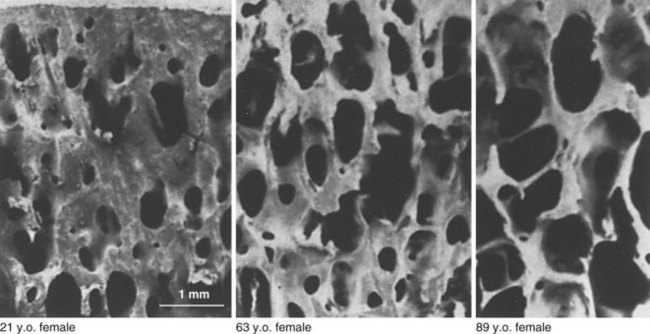
 Age-related decrease in bone mass
Age-related decrease in bone mass

 A quantitative, not qualitative, defect
A quantitative, not qualitative, defect

 World Health Organization’s definition
World Health Organization’s definition
 Lumbar (L2 to L4) density is 2.5 or more standard deviations less than mean peak bone mass of a healthy 25-year-old (T-score).
Lumbar (L2 to L4) density is 2.5 or more standard deviations less than mean peak bone mass of a healthy 25-year-old (T-score).

 Responsible for more than 1 million fractures/year
Responsible for more than 1 million fractures/year
 Fractures of the vertebral body are most common.
Fractures of the vertebral body are most common.


 Vertebral compression fracture is associated with increased mortality rate.
Vertebral compression fracture is associated with increased mortality rate.

 Lifetime risk of fracture in white women after 50 years of age: 75%
Lifetime risk of fracture in white women after 50 years of age: 75%


 Cancellous bone is most affected.
Cancellous bone is most affected.





 Type I osteoporosis (postmenopausal)
Type I osteoporosis (postmenopausal)


 Type II osteoporosis (age-related)
Type II osteoporosis (age-related)
 In patients older than 75 years
In patients older than 75 years
 Affects both trabecular and cortical bone
Affects both trabecular and cortical bone



 Obtained to rule out secondary causes of low bone mass
Obtained to rule out secondary causes of low bone mass
 Vitamin D deficiency, hyperthyroidism, hyperparathyroidism, Cushing’s syndrome, hematologic disorders, malignancy
Vitamin D deficiency, hyperthyroidism, hyperparathyroidism, Cushing’s syndrome, hematologic disorders, malignancy

 Results of these studies are usually unremarkable in osteoporosis.
Results of these studies are usually unremarkable in osteoporosis.
 Plain radiographs not helpful unless bone loss exceeds 30%
Plain radiographs not helpful unless bone loss exceeds 30%

 Single-photon (appendicular) absorptiometry
Single-photon (appendicular) absorptiometry
 Double-photon (axial) absorptiometry
Double-photon (axial) absorptiometry



















 Other drugs, such as intramuscular calcitonin, may be helpful.
Other drugs, such as intramuscular calcitonin, may be helpful.



 Prophylaxis for patients at risk for osteoporosis:
Prophylaxis for patients at risk for osteoporosis:
 Diet with adequate calcium intake
Diet with adequate calcium intake
 Weight-bearing exercise program
Weight-bearing exercise program
 Estrogen therapy evaluation at menopause
Estrogen therapy evaluation at menopause
 Idiopathic transient osteoporosis of the hip
Idiopathic transient osteoporosis of the hip
 Uncommon; diagnosis of exclusion
Uncommon; diagnosis of exclusion
 Most common during the third trimester of pregnancy in women but can occur in men
Most common during the third trimester of pregnancy in women but can occur in men
 Groin pain, limited range of motion (ROM), and localized osteopenia without a history of trauma
Groin pain, limited range of motion (ROM), and localized osteopenia without a history of trauma
 Treatment: analgesics and limited weight bearing
Treatment: analgesics and limited weight bearing
 Generally self-limiting and tends to resolve spontaneously after 6 to 8 months
Generally self-limiting and tends to resolve spontaneously after 6 to 8 months























 Biopsy (transiliac); required for diagnosis
Biopsy (transiliac); required for diagnosis

 Femoral neck fractures are common
Femoral neck fractures are common



 Vitamin C (ascorbic acid) deficiency
Vitamin C (ascorbic acid) deficiency
 Produces a decrease in chondroitin sulfate synthesis
Produces a decrease in chondroitin sulfate synthesis
 Leads to defective collagen growth and repair
Leads to defective collagen growth and repair
 Also leads to impaired intracellular hydroxylation of collagen peptides
Also leads to impaired intracellular hydroxylation of collagen peptides
























 Osteopetrosis (marble bone disease)
Osteopetrosis (marble bone disease)
 Osteopetrosis is the term for a group of bone disorders.
Osteopetrosis is the term for a group of bone disorders.

 It may result from an abnormality of the immune system (thymic defect).
It may result from an abnormality of the immune system (thymic defect).
 Osteoclasts lack the normal ruffled border and clear zone.
Osteoclasts lack the normal ruffled border and clear zone.
 Marrow spaces fill with necrotic calcified cartilage.
Marrow spaces fill with necrotic calcified cartilage.
 The cartilage may be trapped within the osteoid.
The cartilage may be trapped within the osteoid.
 Empty lacunae and plugging of haversian canals are also observed.
Empty lacunae and plugging of haversian canals are also observed.
 One of these disorders is infantile autosomal recessive (“malignant”) osteopetrosis.
One of these disorders is infantile autosomal recessive (“malignant”) osteopetrosis.

 “Bone within a bone” appearance on radiographs
“Bone within a bone” appearance on radiographs


 Can lead to death during infancy
Can lead to death during infancy
 Bone marrow transplantation (e.g., osteoclast precursors) can be lifesaving during childhood
Bone marrow transplantation (e.g., osteoclast precursors) can be lifesaving during childhood
 High doses of calcitriol with or without steroids may also be helpful
High doses of calcitriol with or without steroids may also be helpful
 Another disorder is autosomal dominant “tarda” (benign) osteopetrosis (Albers-Schönberg disease).
Another disorder is autosomal dominant “tarda” (benign) osteopetrosis (Albers-Schönberg disease).



















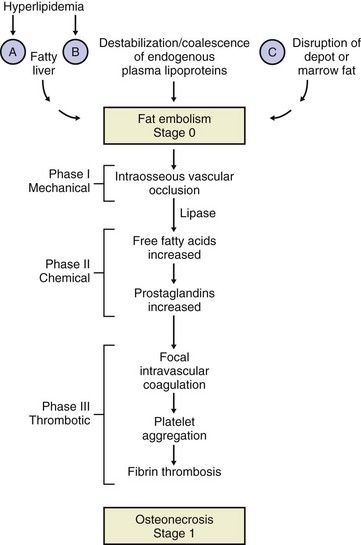
D Conditions of bone viability
 Death of bony tissue from causes other than infection
Death of bony tissue from causes other than infection





 Commonly affects the hip joint
Commonly affects the hip joint

 Associated with the following conditions:
Associated with the following conditions:








 Vascular insults and other factors may also be significant.
Vascular insults and other factors may also be significant.
 Idiopathic (or spontaneous) osteonecrosis is diagnosed when no other cause can be identified.
Idiopathic (or spontaneous) osteonecrosis is diagnosed when no other cause can be identified.
 Chandler’s disease: osteonecrosis of the femoral head in adults
Chandler’s disease: osteonecrosis of the femoral head in adults
 Medial femoral condyle osteonecrosis: most common in women older than 60 years
Medial femoral condyle osteonecrosis: most common in women older than 60 years
 Idiopathic, alcohol, and dysbaric forms of osteonecrosis are associated with multiple insults.
Idiopathic, alcohol, and dysbaric forms of osteonecrosis are associated with multiple insults.



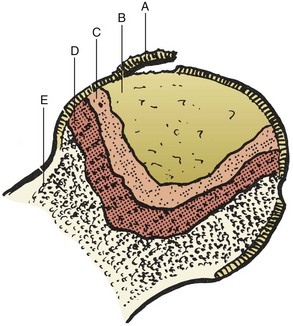
 Grossly necrotic bone, fibrous tissue, and subchondral collapse may be observed (Figures 1-36 and 1-37).
Grossly necrotic bone, fibrous tissue, and subchondral collapse may be observed (Figures 1-36 and 1-37).









 A careful history (to discern risk factors) and physical examination (e.g., to discern decreased ROM, limp) should precede additional studies.
A careful history (to discern risk factors) and physical examination (e.g., to discern decreased ROM, limp) should precede additional studies.

 The process is bilateral in the hip in 50% of cases of idiopathic osteonecrosis and up to 80% of cases of steroid-induced osteonecrosis.
The process is bilateral in the hip in 50% of cases of idiopathic osteonecrosis and up to 80% of cases of steroid-induced osteonecrosis.