Hand, Upper Extremity, and Microvascular Surgery
III. Carpal Fractures and Instability
IV. Metacarpal and Phalangeal Injuries
V. Tendon Injuries and Overuse Syndromes
VI. Distal Radioulnar Joint, Triangular Fibrocartilage Complex, and Wrist Arthroscopy
VII. Nail and Fingertip Injuries
VIII. Soft Tissue Coverage and Microsurgery
XI. Nerve Injuries and Tendon Transfers
XIII. Idiopathic Osteonecrosis of the Carpus
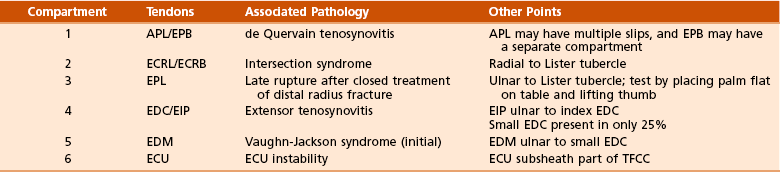
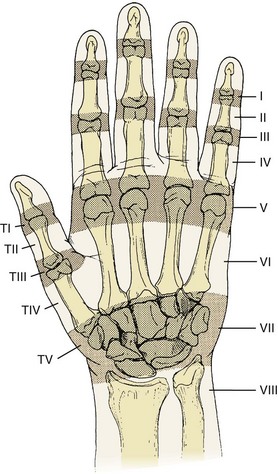
1. Extensor (dorsal) compartments of the wrist (Figure 7-1 and Table 7-1)

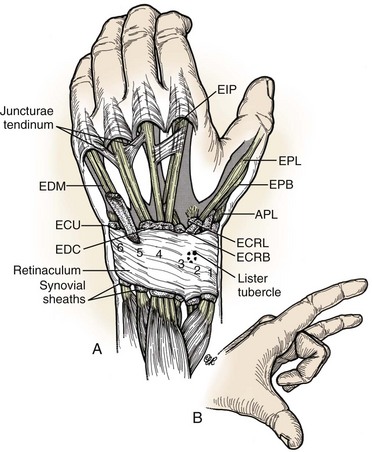
2. Extensor retinaculum—prevents tendon bowstringing at wrist
3. Juncturae tendinum—extensor tendon interconnections in hand that may mask proximal tendon lacerations
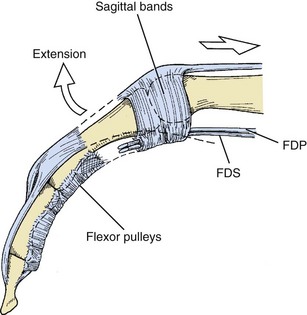
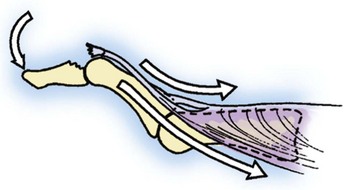
4. Sagittal bands—aid in metacarpophalangeal (MCP) joint extension, centralize the extensor mechanism, and attach to the volar plate (Figure 7-2)
5. Central slip—inserts on base of middle phalanx (P2), aids in proximal interphalangeal (PIP) joint extension (Figure 7-3)
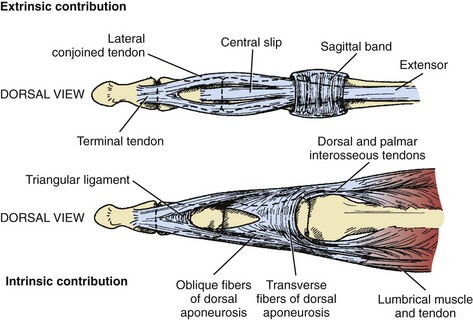
6. Extensor mechanism receives contributions from the intrinsic muscles—interossei and lumbricals (see Figures 7-3 and 7-4)
7. Lateral bands—receive contributions from common extensor and intrinsics, converge to form terminal extensor tendon, which inserts on base of distal phalanx (P3) (see Figures 7-3 and 7-4)
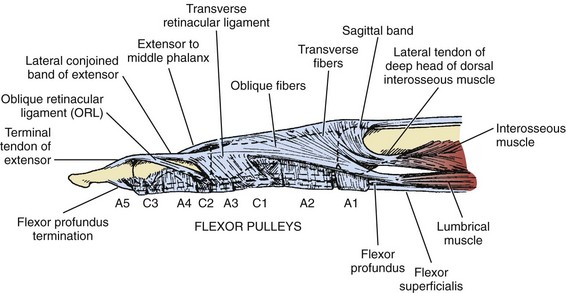
8. Transverse retinacular ligament—prevents dorsal subluxation of lateral bands (see Figure 7-4)
9. Triangular ligament—prevents volar subluxation of lateral bands (see Figure 7-3)
10. Oblique retinacular ligament (ligament of Landsmeer)—helps to link PIP and distal interphalangeal (DIP) joint extension (see Figure 7-4)
11. Grayson/Cleland ligaments—volar and dorsal to digital neurovascular bundles, respectively (Grayson is ground; Cleland is ceiling)
1. Flexor digitorum profundus (FDP)—flexes the DIP joint, aids in PIP and MCP flexion, typically shares common muscle belly in forearm

2. Flexor digitorum superficialis (FDS)—flexes the PIP joint, aids in MCP flexion, individual muscle bellies in forearm

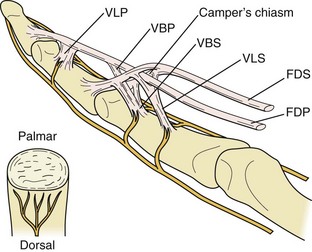
3. FDP tendon splits FDS at the Campers chiasm at level of proximal phalanx (P1) (Figure 7-5).
4. Flexor tendon sheath—encompasses tendons distal to MCP joint
5. Vascular supply to flexor tendons is twofold.



6. Each digit has five annular pulleys (A1 to A5) and three cruciate pulleys (C1 to C3).

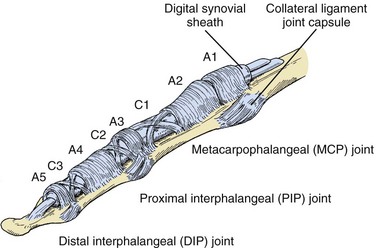

7. Thumb has two annular pulleys and an oblique pulley in between that prevents bowstringing.
8. Carpal tunnel contains median nerve and nine flexor tendons (one flexor pollicis longus [FPL], four FDS, and four FDP tendons).
 FPL tendon—most radial structure in carpal tunnel
FPL tendon—most radial structure in carpal tunnel
 Long and ring FDS tendons are volar to index and small FDS (Figure 7-7).
Long and ring FDS tendons are volar to index and small FDS (Figure 7-7).
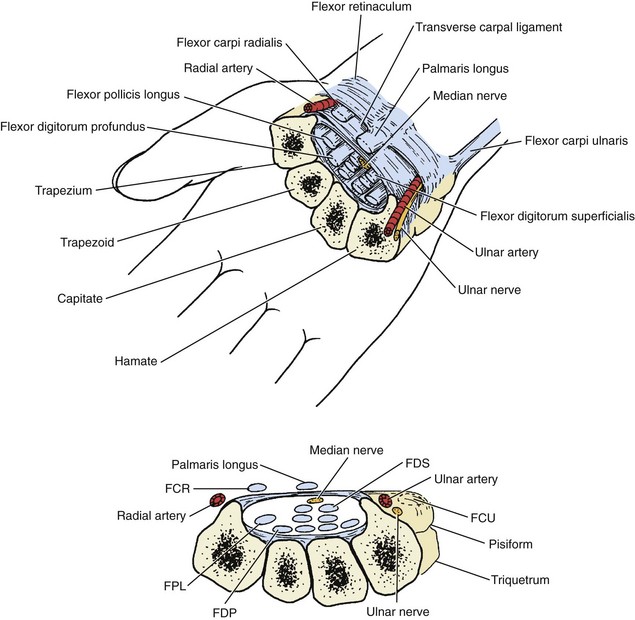

9. The Guyon canal (ulnar tunnel)—contains the ulnar nerve and artery

10. Linburg sign—interconnections between FPL and index FDP in forearm; unilateral in 25% to 30%, bilateral in 5% to 15%
11. Palmaris longus (PL) tendon—present 80% to 85% of the time, common source of autograft for upper extremity reconstructive procedures
12. Flexor carpi radialis (FCR)/flexor carpi ulnaris (FCU)—primary wrist flexors, insert on base of second metacarpal and pisiform, respectively
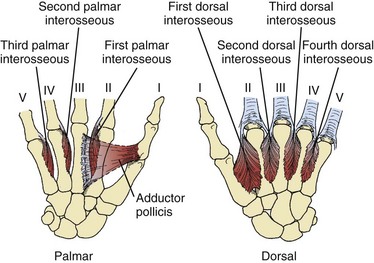
1. Four dorsal interosseous (digit abductors) and three palmar interosseous (digit adductor) muscles

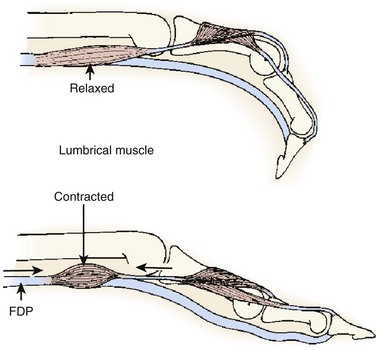
2. Lumbrical muscles originate on radial aspect of FDP tendons and pass volar to transverse metacarpal ligaments to insert on the radial aspect of the extensor hood lateral bands.
 Contribute to interphalangeal joint extension through radial lateral bands, relax extrinsic flexor system (Figure 7-9)
Contribute to interphalangeal joint extension through radial lateral bands, relax extrinsic flexor system (Figure 7-9)


3. Intrinsic tightness—PIP flexion less with MCP joints held in extension (intrinsics on stretch, extrinsics relaxed)
4. Extrinsic tightness—PIP flexion less with MCP joints held in flexion (extrinsics on stretch, intrinsics relaxed)
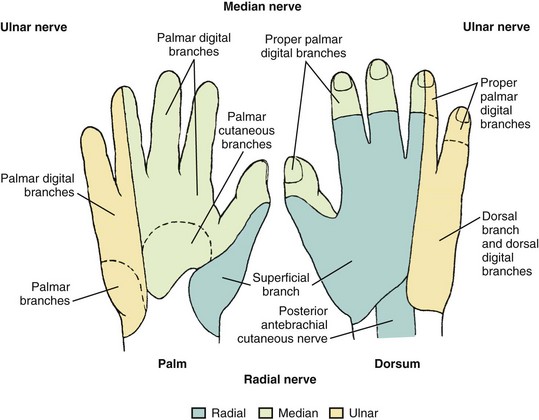
1. Entire hand supplied by branches of median, radial, and ulnar nerves
2. Sensory innervation of hand—Figure 7-10
3. Median nerve—innervates pronator teres, FDS, FCR, PL, radial two lumbricals
 Anterior interosseous branch of median nerve—innervates FPL, index and long FDP (50% of time), pronator quadratus
Anterior interosseous branch of median nerve—innervates FPL, index and long FDP (50% of time), pronator quadratus


4. Ulnar nerve—innervates FCU, ring/small FDP (50% of time), ulnar two lumbricals
 Deep motor branch of ulnar nerve—innervates hypothenar and interosseous muscles, adductor pollicis, and deep head of flexor pollicis brevis
Deep motor branch of ulnar nerve—innervates hypothenar and interosseous muscles, adductor pollicis, and deep head of flexor pollicis brevis
5. Martin-Gruber anastomoses—crossover variations between median and ulnar nerves, approximately 15% of population
6. Radial nerve proper—innervates lateral portion of brachialis (also musculocutaneous), triceps, anconeus, brachioradialis, extensor carpi radialis longus (ECRL)
 Divides into superficial sensory branch and posterior interosseous nerve (PIN), which innervates remaining extensor muscles
Divides into superficial sensory branch and posterior interosseous nerve (PIN), which innervates remaining extensor muscles
 Extensor carpi radialis brevis (ECRB) has variable innervation.
Extensor carpi radialis brevis (ECRB) has variable innervation.
 Terminal branch of PIN—lies at floor of fourth extensor compartment
Terminal branch of PIN—lies at floor of fourth extensor compartment
7. Proper digital nerves lie volar to proper digital arteries.
8. Vascular anatomy is covered in the section Vascular Disorders.
1. Most common fracture of the upper extremity (>300,000 per year in United States)
2. High-energy trauma in young
3. Low-energy falls in elderly persons with osteoporotic bone
1. Distal radius articular surface—biconcave, scaphoid and lunate facets
2. Distal radioulnar joint (DRUJ)—articulation with ulna at sigmoid notch
3. Lister tubercle—small dorsal prominence, landmark for dorsal approach to wrist
4. Metaphysis—thin cortex, vulnerable to bending forces
1. Pain, swelling, and deformity at the wrist after trauma
2. Open injuries more common in young patients
3. Examine for concurrent anatomic snuffbox and ulnar-sided tenderness.
4. Evaluate the shoulder and elbow.



D Radiographic evaluation (posteroanterior, lateral, and oblique views)





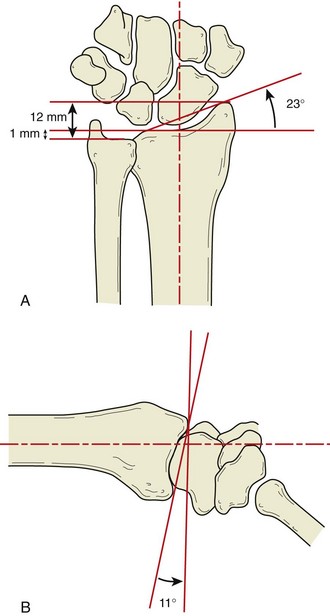

5. Volar tilt (lunate fossa inclination)

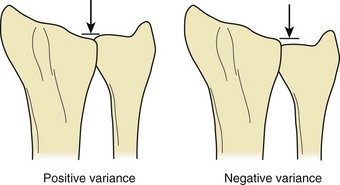
6. Ulnar variance—neutral (normal), positive, or negative



8. Associated fractures—ulnar styloid, distal ulna, carpus
 Isolated fracture of radial styloid (chauffeur’s fracture)—may be associated with scapholunate ligament disruption
Isolated fracture of radial styloid (chauffeur’s fracture)—may be associated with scapholunate ligament disruption




9. Other imaging studies—computed tomography (CT) for detail of complex intraarticular patterns; magnetic resonance imaging (MRI) for occult fracture, bone contusion, associated soft tissue injury
2. Common eponyms (Colles, Smith, Barton, Hutchinson) predate radiography.
3. Over 10 other schemes exist (e.g., AO, Frykman, Fernandez, Melone, Mayo) but largely fail to help predict treatment or prognosis.
1. General goals—maintain reduction until union, restore function, prevent symptomatic post-traumatic radiocarpal osteoarthrosis
2. Factors considered—age, medical condition, activity demands, bone quality, fracture stability, associated injuries
 Definitive cast immobilization (favored over removable splints) sufficient in minimally displaced low-energy injuries, especially in functionally low-demand patients
Definitive cast immobilization (favored over removable splints) sufficient in minimally displaced low-energy injuries, especially in functionally low-demand patients


 Dorsal hematoma block with local anesthetic
Dorsal hematoma block with local anesthetic
 Finger traps, upper arm counterweight for ligamentotaxis
Finger traps, upper arm counterweight for ligamentotaxis
 Recreate deformity, manipulate distal fragment.
Recreate deformity, manipulate distal fragment.
 Sugar tong plaster splint with three-point mold
Sugar tong plaster splint with three-point mold
 Keep MCP and interphalangeal joints free for motion.
Keep MCP and interphalangeal joints free for motion.
 Radiographs obtained weekly for first 3 weeks
Radiographs obtained weekly for first 3 weeks
 Loss of reduction correlates with increasing age.
Loss of reduction correlates with increasing age.
 Postreduction benchmarks (American Academy of Orthopaedic Surgeons guideline)
Postreduction benchmarks (American Academy of Orthopaedic Surgeons guideline)



 Immobilization for 6 to 8 weeks (no evidence to support any particular type)
Immobilization for 6 to 8 weeks (no evidence to support any particular type)



 Closed reduction and percutaneous pinning (CRPP)
Closed reduction and percutaneous pinning (CRPP)



 Open reduction with internal fixation (ORIF)
Open reduction with internal fixation (ORIF)

 Approach between third and fourth extensor compartments
Approach between third and fourth extensor compartments
 Articular reduction directly visualized
Articular reduction directly visualized
 Best for dorsally displaced fractures with dorsal bony defects
Best for dorsally displaced fractures with dorsal bony defects
 Historical disadvantage—extensor tendon irritation/rupture from prominent hardware
Historical disadvantage—extensor tendon irritation/rupture from prominent hardware

 Henry approach between FCR and radial artery or through floor of FCR tendon sheath
Henry approach between FCR and radial artery or through floor of FCR tendon sheath
 Articular reduction not directly visualized, relies on fluoroscopic guidance
Articular reduction not directly visualized, relies on fluoroscopic guidance
 Fixed-angle and variable-angle plates available
Fixed-angle and variable-angle plates available
 Best for Smith and Barton fracture patterns, increasingly used for dorsally displaced injuries
Best for Smith and Barton fracture patterns, increasingly used for dorsally displaced injuries












 Concurrent treatment of ulnar styloid fracture not routinely necessary
Concurrent treatment of ulnar styloid fracture not routinely necessary


 Median nerve dysfunction is the most common complication following a distal radius fracture.
Median nerve dysfunction is the most common complication following a distal radius fracture.
 Extensor pollicis longus (EPL) tendon rupture
Extensor pollicis longus (EPL) tendon rupture
 Most commonly occurs as a late complication following closed treatment because of attritional wear and/or vascular insufficiency near the Lister tubercle
Most commonly occurs as a late complication following closed treatment because of attritional wear and/or vascular insufficiency near the Lister tubercle
 Typically presents as a painless, acute loss of thumb extension
Typically presents as a painless, acute loss of thumb extension
 Treat with PL intercalary autograft or extensor indicis proprius (EIP)-to-EPL tendon transfer.
Treat with PL intercalary autograft or extensor indicis proprius (EIP)-to-EPL tendon transfer.


 Asymptomatic malunion in a functionally low-demand patient does not require treatment.
Asymptomatic malunion in a functionally low-demand patient does not require treatment.

 A corrective radius osteotomy with ORIF and bone grafting may be indicated for high-demand patients.
A corrective radius osteotomy with ORIF and bone grafting may be indicated for high-demand patients.

 Multiple case reports of flexor tendon ruptures after volar plating
Multiple case reports of flexor tendon ruptures after volar plating



III CARPAL FRACTURES AND INSTABILITY
1. Eight carpal bones aligned in two rows
2. Proximal row—scaphoid, lunate, and triquetrum

3. Distal row—trapezium, trapezoid, capitate, and hamate
4. Pisiform is sesamoid within the FCU tendon.
5. Dart-thrower’s motion is combined wrist extension–radial deviation to wrist flexion–ulnar deviation.


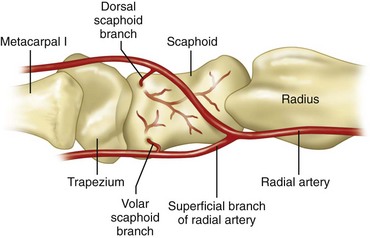
6. Carpus has a rich vascular supply with multiple anastomoses.
7. Scaphoid, lunate, and capitate may each have large area supplied by a single interosseous vessel.
8. Some evidence suggests a proprioceptive role for the terminal branch of the posterior interosseous nerve, which may be compromised when this branch is sacrificed during dorsal approaches to the wrist.
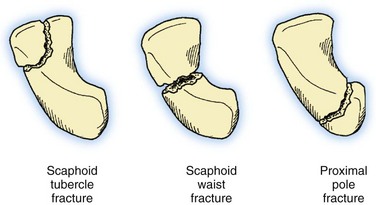
1. Most common carpal fracture (Table 7-2), accounting for up to 15% of all acute wrist injuries
Table 7-2
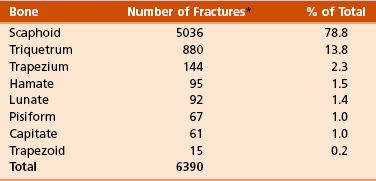
*The number of fractures represents a total of 6390 fractures compiled from three referenced studies to accumulate incidence of carpal bone fractures.
From Green DP, et al, editors: Green’s operative hand surgery, ed 5, Philadelphia, 2005, Churchill Livingstone, p 711.

 Approximately 75% covered by articular cartilage
Approximately 75% covered by articular cartilage


 Tenuous vascular anatomy renders waist and proximal pole fractures at risk for nonunion and post-traumatic osteonecrosis (Figure 7-13).
Tenuous vascular anatomy renders waist and proximal pole fractures at risk for nonunion and post-traumatic osteonecrosis (Figure 7-13).

 Suspect when chief complaint is radial-sided wrist pain after injury or trauma
Suspect when chief complaint is radial-sided wrist pain after injury or trauma
 Most common mechanism is forced hyperextension and radial deviation of the wrist.
Most common mechanism is forced hyperextension and radial deviation of the wrist.
 This results in force transmission through the radioscaphoid articulation and concentration at the scaphoid.
This results in force transmission through the radioscaphoid articulation and concentration at the scaphoid.
 Swelling, anatomic snuffbox/volar tubercle tenderness, limited wrist motion
Swelling, anatomic snuffbox/volar tubercle tenderness, limited wrist motion
 Posteroanterior, lateral, oblique, and scaphoid radiographic views
Posteroanterior, lateral, oblique, and scaphoid radiographic views
 Scaphoid view—approximately 30 degrees of wrist extension and approximately 20 degrees of ulnar deviation
Scaphoid view—approximately 30 degrees of wrist extension and approximately 20 degrees of ulnar deviation
 Radiographs initially nondiagnostic in more than 30% of cases
Radiographs initially nondiagnostic in more than 30% of cases

 Bone scan, ultrasonography, CT, and MRI have all been used for earlier diagnosis.
Bone scan, ultrasonography, CT, and MRI have all been used for earlier diagnosis.
 MRI has highest sensitivity, specificity, and accuracy (all >95%) with high positive and negative predictive values.
MRI has highest sensitivity, specificity, and accuracy (all >95%) with high positive and negative predictive values.
 CT has lower predictive values.
CT has lower predictive values.
 Bone scan and ultrasonography lowest specificity and positive predictive value
Bone scan and ultrasonography lowest specificity and positive predictive value
 All of these are better for ruling out rather than ruling in a scaphoid fracture.
All of these are better for ruling out rather than ruling in a scaphoid fracture.
 Neglect of injury for 4 weeks increases nonunion rate from approximately 5% to 45%.
Neglect of injury for 4 weeks increases nonunion rate from approximately 5% to 45%.








 Cast immobilization for nondisplaced fractures
Cast immobilization for nondisplaced fractures


 Consequently, length of cast immobilization should be greater for more proximal fractures.
Consequently, length of cast immobilization should be greater for more proximal fractures.

 Indications include greater than 1 mm displacement, intrascaphoid angle greater than 35 degrees (humpback deformity), and trans-scaphoid perilunate dislocation.
Indications include greater than 1 mm displacement, intrascaphoid angle greater than 35 degrees (humpback deformity), and trans-scaphoid perilunate dislocation.
 Proximal pole fracture is also a relative indication
Proximal pole fracture is also a relative indication
 Minimally displaced fractures may be treated with percutaneous internal fixation.
Minimally displaced fractures may be treated with percutaneous internal fixation.



 Formal ORIF with headless compression screw for displaced injuries
Formal ORIF with headless compression screw for displaced injuries

 Approach dictated by fracture location and surgeon preference
Approach dictated by fracture location and surgeon preference
 Volar approach potentially avoids disruption to the blood supply of the scaphoid and is the most commonly employed approach.
Volar approach potentially avoids disruption to the blood supply of the scaphoid and is the most commonly employed approach.
 Union rates of over 90% to 95% expected
Union rates of over 90% to 95% expected
 Aggressive physical therapy typically delayed until radiographic union achieved
Aggressive physical therapy typically delayed until radiographic union achieved


 Include nonunion, malunion, osteonecrosis, and post-traumatic osteoarthrosis
Include nonunion, malunion, osteonecrosis, and post-traumatic osteoarthrosis
 Symptomatic, early-stage scaphoid nonunion may be treated with ORIF and bone grafting.
Symptomatic, early-stage scaphoid nonunion may be treated with ORIF and bone grafting.
 Inlay (Russe) technique best used in cases with minimal deformity and vascularized proximal pole
Inlay (Russe) technique best used in cases with minimal deformity and vascularized proximal pole

 Grafts obtained from distal radius or iliac crest
Grafts obtained from distal radius or iliac crest
 Most surgeons typically use supplemental headless compression screw in nonunion cases.
Most surgeons typically use supplemental headless compression screw in nonunion cases.
 Presence of intraoperative punctate bleeding is most reliable sign of vascular proximal pole.
Presence of intraoperative punctate bleeding is most reliable sign of vascular proximal pole.
 Vascularized bone grafting has gained popularity in nonunions with avascular proximal pole.
Vascularized bone grafting has gained popularity in nonunions with avascular proximal pole.
 Most commonly harvested from dorsal aspect of distal radius, based on 1,2 intercompartmental supraretinacular artery (1,2 ICSRA)
Most commonly harvested from dorsal aspect of distal radius, based on 1,2 intercompartmental supraretinacular artery (1,2 ICSRA)







C Other carpal bone fractures—small fraction of wrist injuries (see Table 7-2)
1. Lunate—rarely encountered in isolation



2. Capitate neck—may occur in combination with scaphoid fracture or perilunate dislocation, treated with ORIF or intercarpal fusion
3. Triquetrum—Majority of injuries are dorsal capsular avulsion fractures (wrist sprain) and require only brief period of immobilization.
4. Hook of hamate—often from blunt trauma to palm, frequently associated with certain sports (e.g., golf, baseball, hockey, racquet sports)








1. Disruption of normal kinematics of wrist
2. Characterized by wrist pain, loss of motion, weakness
3. If untreated, may lead to degenerative arthritis and disability
4. Spectrum of injury from occult (predynamic) to dynamic to static
5. Static instability detected on standard radiographs, whereas dynamic instability requires either stress radiographs requires either stress radiographs, cineradiography, or live fluoroscopy
6. Carpal instability dissociative (CID) describes instability between individual carpal bones of single carpal row.
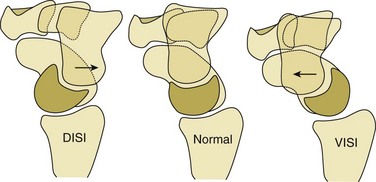
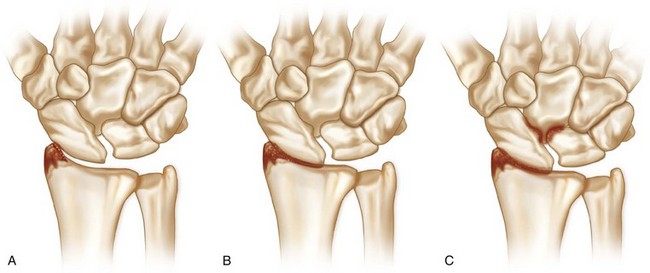
 Examples include classical patterns of dorsal intercalated segmental instability (DISI) and volar intercalated segmental instability (VISI) (Figure 7-16).
Examples include classical patterns of dorsal intercalated segmental instability (DISI) and volar intercalated segmental instability (VISI) (Figure 7-16).

7. Carpal instability nondissociative (CIND) describes instability between carpal rows, such as midcarpal or radiocarpal instability.
8. Carpal instability resulting from malunited distal radius fracture is an example of carpal instability adaptive.
9. Perilunate dislocations combine CID and CIND and are classified as carpal instability complex.
 DISI—most common form of carpal instability
DISI—most common form of carpal instability
 Scapholunate ligament disruption
Scapholunate ligament disruption
 Dorsal fibers are stronger than volar fibers.
Dorsal fibers are stronger than volar fibers.

 Scaphoid hyperflexion and lunate hyperextension
Scaphoid hyperflexion and lunate hyperextension
 May be traumatic or result from inflammatory or crystalline arthropathy
May be traumatic or result from inflammatory or crystalline arthropathy

 Dorsal wrist pain, often with loading
Dorsal wrist pain, often with loading

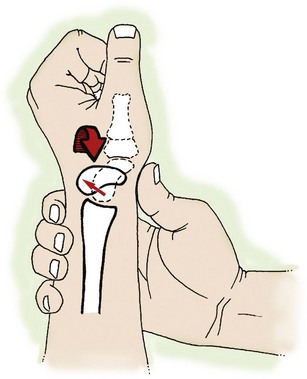
 Reproduction of pain/palpable clunk with scaphoid shift test (dorsally directed pressure over volar scaphoid tubercle while wrist brought from ulnar to radial deviation subluxates or dislocates scaphoid over dorsal ridge of distal radius that when released causes scaphoid to reduce with painful clunk) (Figure 7-17)
Reproduction of pain/palpable clunk with scaphoid shift test (dorsally directed pressure over volar scaphoid tubercle while wrist brought from ulnar to radial deviation subluxates or dislocates scaphoid over dorsal ridge of distal radius that when released causes scaphoid to reduce with painful clunk) (Figure 7-17)

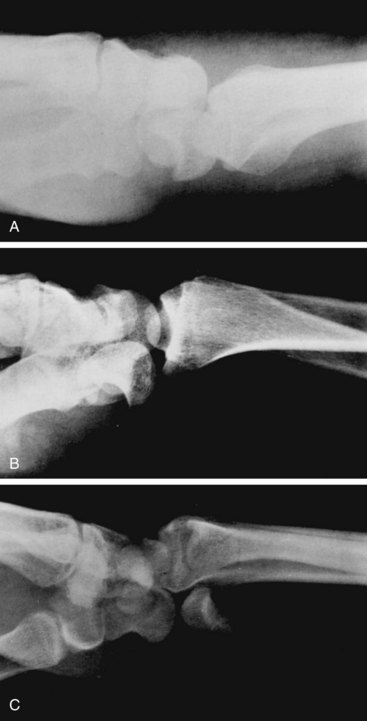
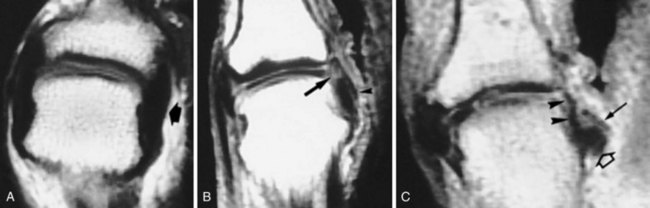
 Standard radiographs may reveal cortical ring sign (Figure 7-18), increased scapholunate angle (>70 degrees), or widened scapholunate interval (>3 mm) in static DISI.
Standard radiographs may reveal cortical ring sign (Figure 7-18), increased scapholunate angle (>70 degrees), or widened scapholunate interval (>3 mm) in static DISI.


 MRI best, but not perfect, for detection of scapholunate ligament injury (see Figure 7-18)
MRI best, but not perfect, for detection of scapholunate ligament injury (see Figure 7-18)
 Gold standard is wrist arthroscopy.
Gold standard is wrist arthroscopy.
 Geissler classification (Table 7-3)
Geissler classification (Table 7-3)
Table 7-3
Geissler Classification of Arthroscopic Scapholunate Ligament Disruption
| Grade | Description |
| I | Attenuation or hemorrhage of interosseous ligament as seen from radiocarpal space. No incongruity of carpal alignment in midcarpal space. |
| II | Attenuation or hemorrhage of interosseous ligament as seen from radiocarpal space. There may be a slight gap (less than width of probe) between carpal bones in midcarpal space. |
| III | Incongruity or step-off of carpal alignment as seen from both radiocarpal and midcarpal space. Probe may be passed through gap between carpal bones. |
| IV | Incongruity or step-off of carpal alignment as seen from both radiocarpal and midcarpal space. There is gross instability with manipulation. A 2.7-mm arthroscope may be passed through the gap between carpal bones (“drive-through sign”). |
 Treatment depends on stage of instability.
Treatment depends on stage of instability.
 Partial injuries may improve with nonoperative treatment or arthroscopic débridement.
Partial injuries may improve with nonoperative treatment or arthroscopic débridement.
 Acute scapholunate ligament rupture may be amenable to primary repair.
Acute scapholunate ligament rupture may be amenable to primary repair.

 Limited clinical data on reduction-association of scaphoid and lunate (RASL) procedure
Limited clinical data on reduction-association of scaphoid and lunate (RASL) procedure
 Tendon and bone-retinaculum-bone grafts have been attempted for scapholunate reconstruction.
Tendon and bone-retinaculum-bone grafts have been attempted for scapholunate reconstruction.
 Cases of chronic, static instability may result in scapholunate advanced collapse (SLAC wrist).
Cases of chronic, static instability may result in scapholunate advanced collapse (SLAC wrist).




 VISI—second most common form of carpal instability
VISI—second most common form of carpal instability
 Disruption of lunotriquetral interosseous ligament
Disruption of lunotriquetral interosseous ligament
 Volar fibers are stronger than dorsal fibers.
Volar fibers are stronger than dorsal fibers.
 Accompanying injury of the dorsal extrinsic ligaments may result in static instability.
Accompanying injury of the dorsal extrinsic ligaments may result in static instability.


 Both the scaphoid and lunate tilt volarly.
Both the scaphoid and lunate tilt volarly.




 MRI may show pathology of lunotriquetral ligament.
MRI may show pathology of lunotriquetral ligament.







 Clunking wrist that may or may not be painful
Clunking wrist that may or may not be painful
 Many patient have generalized ligamentous laxity.
Many patient have generalized ligamentous laxity.
 History of trauma often absent
History of trauma often absent
 Sudden shift of proximal carpal row with active radial or ulnar deviation (cineradiographic studies)
Sudden shift of proximal carpal row with active radial or ulnar deviation (cineradiographic studies)


 Radiocarpal dislocation (CIND)
Radiocarpal dislocation (CIND)



 Volar more severe than dorsal dislocation
Volar more severe than dorsal dislocation
 May be purely ligamentous or include radial and/or ulnar styloid fractures
May be purely ligamentous or include radial and/or ulnar styloid fractures
 Ulnar translocation of the carpus signifies global ligamentous disruption.
Ulnar translocation of the carpus signifies global ligamentous disruption.





 Moneim proposed two types based on accompanying intracarpal fracture or interosseous ligament injury
Moneim proposed two types based on accompanying intracarpal fracture or interosseous ligament injury

 ORIF of styloid fractures may be enough to restore stability.
ORIF of styloid fractures may be enough to restore stability.
 May also require direct ligamentous repair and/or external fixation to neutralize forces
May also require direct ligamentous repair and/or external fixation to neutralize forces

 Carpal instability adaptive from distal radius malunion
Carpal instability adaptive from distal radius malunion

 Perilunate dislocations (carpal instability complex)
Perilunate dislocations (carpal instability complex)
 Potentially devastating injuries resulting from forced dorsiflexion, ulnar deviation, and supination of wrist
Potentially devastating injuries resulting from forced dorsiflexion, ulnar deviation, and supination of wrist
 Approximately 25% of cases may be missed in the emergency department
Approximately 25% of cases may be missed in the emergency department

 Stage I—scapholunate disruption
Stage I—scapholunate disruption
 Stage II—scaphocapitate disruption
Stage II—scaphocapitate disruption
 Stage III—lunotriquetral disruption
Stage III—lunotriquetral disruption


 Stage IV—circumferential disruption
Stage IV—circumferential disruption

 Lesser-arc injuries—purely ligamentous
Lesser-arc injuries—purely ligamentous
 Greater-arc injuries—carpal fracture
Greater-arc injuries—carpal fracture


 May attempt immediate closed reduction, especially in setting of acute carpal tunnel syndrome
May attempt immediate closed reduction, especially in setting of acute carpal tunnel syndrome








IV METACARPAL AND PHALANGEAL INJURIES
1. Most frequently encountered injuries of skeletal system
2. Vast majority treated nonoperatively
 Many initially splinted with hand in intrinsic-plus or “safe” position
Many initially splinted with hand in intrinsic-plus or “safe” position




3. Surgical intervention may be indicated in open injuries, intraarticular fractures, irreducible fractures, digit malrotation, and multiple fractures.
4. Digit rotation assessed statically with wrist tenodesis and dynamically as patient initiates making a fist

5. Goals of treatment are stable reduction, edema control, and early range of motion.

 Most commonly occurs in index or middle finger
Most commonly occurs in index or middle finger




 Most frequently involves the ring and small finger
Most frequently involves the ring and small finger
 “Boxer’s fracture”—metacarpal neck fracture of the small finger
“Boxer’s fracture”—metacarpal neck fracture of the small finger
 Intrinsic muscles are major deforming force leading to apex dorsal angulation.
Intrinsic muscles are major deforming force leading to apex dorsal angulation.
 Check rotation, MCP joint extensor lag.
Check rotation, MCP joint extensor lag.
 Many treated with closed reduction (Jahss maneuver) and 3 to 4 weeks of immobilization (Figure 7-21)
Many treated with closed reduction (Jahss maneuver) and 3 to 4 weeks of immobilization (Figure 7-21)
 Suggested acceptable angulation of each metacarpal neck
Suggested acceptable angulation of each metacarpal neck


 Small finger less than 70 degrees (controversial)
Small finger less than 70 degrees (controversial)
 Greater compensation from more mobile fourth and fifth carpometacarpal (CMC) joint
Greater compensation from more mobile fourth and fifth carpometacarpal (CMC) joint

 May be transverse, oblique, or spiral
May be transverse, oblique, or spiral
 May be associated with higher risk of malrotation
May be associated with higher risk of malrotation

 Suggested acceptable angulation of each metacarpal shaft
Suggested acceptable angulation of each metacarpal shaft


 Every 2 mm of metacarpal shortening leads to 7 degrees of extensor lag.
Every 2 mm of metacarpal shortening leads to 7 degrees of extensor lag.
 Up to 5 mm is acceptable without significant functional deficit.
Up to 5 mm is acceptable without significant functional deficit.



4. Metacarpal base fracture and CMC joint dislocation
 Stable, minimally displaced fractures of metacarpal base are typically treated nonoperatively.
Stable, minimally displaced fractures of metacarpal base are typically treated nonoperatively.
 Ring and small CMC joint fracture-dislocations often result from higher-energy mechanisms.
Ring and small CMC joint fracture-dislocations often result from higher-energy mechanisms.


 Small-finger CMC joint fracture-dislocation is termed a “reverse” or “baby” Bennett fracture.
Small-finger CMC joint fracture-dislocation is termed a “reverse” or “baby” Bennett fracture.

 Accompanying distal row carpal fractures may be seen.
Accompanying distal row carpal fractures may be seen.


 Delayed treatment, painful malunion, or post-traumatic osteoarthrosis may require arthrodesis.
Delayed treatment, painful malunion, or post-traumatic osteoarthrosis may require arthrodesis.
 Most common pattern is extraarticular epibasal fracture.
Most common pattern is extraarticular epibasal fracture.
 Up to 30 degrees of angulation acceptable secondary to compensatory CMC joint motion
Up to 30 degrees of angulation acceptable secondary to compensatory CMC joint motion
 Excessive angulation may lead to MCP joint hyperextension and requires CRPP.
Excessive angulation may lead to MCP joint hyperextension and requires CRPP.
 Bennett fracture is an intraarticular fracture-dislocation.
Bennett fracture is an intraarticular fracture-dislocation.
 Abductor pollicis longus (APL) and thumb extensors cause proximal, dorsal, and radial displacement of the metacarpal shaft.
Abductor pollicis longus (APL) and thumb extensors cause proximal, dorsal, and radial displacement of the metacarpal shaft.
 Adductor pollicis causes supination and adduction of the metacarpal shaft.
Adductor pollicis causes supination and adduction of the metacarpal shaft.
 Anterior oblique or “beak” ligament keeps the volar-ulnar base fragment reduced to trapezium.
Anterior oblique or “beak” ligament keeps the volar-ulnar base fragment reduced to trapezium.
 CRPP or ORIF is chosen based on size of fragment.
CRPP or ORIF is chosen based on size of fragment.


 Rolando fracture is a comminuted intraarticular fracture that may be in shape of Y or T (Figure 7-22).
Rolando fracture is a comminuted intraarticular fracture that may be in shape of Y or T (Figure 7-22).


6. Skier’s or gamekeeper’s thumb
 Acute (skier’s) or chronic (gamekeeper’s) injury to the thumb MCP joint ulnar collateral ligament (UCL)
Acute (skier’s) or chronic (gamekeeper’s) injury to the thumb MCP joint ulnar collateral ligament (UCL)
 Competent UCL is critical for strong, effective pinch.
Competent UCL is critical for strong, effective pinch.
 Mechanism of injury is usually forceful thumb hyperextension and/or hyperabduction.
Mechanism of injury is usually forceful thumb hyperextension and/or hyperabduction.
 Spectrum of injury potentially involving proper UCL, accessory UCL, and volar plate
Spectrum of injury potentially involving proper UCL, accessory UCL, and volar plate
 Radiographs should be obtained before stress examination to rule out bony avulsion injury.
Radiographs should be obtained before stress examination to rule out bony avulsion injury.
 Stress joint with radial deviation both at neutral and 30 degrees of flexion.
Stress joint with radial deviation both at neutral and 30 degrees of flexion.
 Instability in 30 degrees of flexion indicates injury to proper UCL.
Instability in 30 degrees of flexion indicates injury to proper UCL.
 Additional instability in neutral indicates additional injury to accessory UCL and/or volar plate.
Additional instability in neutral indicates additional injury to accessory UCL and/or volar plate.



 Partial injuries may be initially treated with thumb spica cast immobilization for 4 to 6 weeks.
Partial injuries may be initially treated with thumb spica cast immobilization for 4 to 6 weeks.
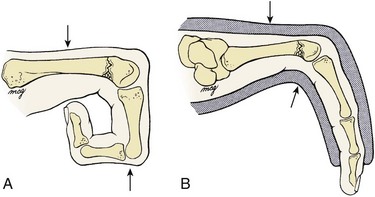
 In over 85% of cases, a complete injury is accompanied by a Stener lesion, in which the adductor pollicis aponeurosis is interposed between the avulsed UCL and its insertion site on the base of the proximal phalanx (Figure 7-23).
In over 85% of cases, a complete injury is accompanied by a Stener lesion, in which the adductor pollicis aponeurosis is interposed between the avulsed UCL and its insertion site on the base of the proximal phalanx (Figure 7-23).




 Classified as simple or complex
Classified as simple or complex
 Dorsal dislocations are most common.
Dorsal dislocations are most common.

 Index, small fingers most frequently involved
Index, small fingers most frequently involved
 In simple dislocation, P1 is perched on metacarpal and closed reduction usually possible
In simple dislocation, P1 is perched on metacarpal and closed reduction usually possible







 Most common hand injury in both amateur and professional fighters
Most common hand injury in both amateur and professional fighters

 Presents with swelling, reduced range of motion, and occasional extensor lag
Presents with swelling, reduced range of motion, and occasional extensor lag

 Fractures of P1 deform with apex volar angulation.
Fractures of P1 deform with apex volar angulation.


 Fractures of P2 deform with apex dorsal or volar angulation.
Fractures of P2 deform with apex dorsal or volar angulation.


 Majority treated nonoperatively if less than 10 degrees of angulation and no rotational deformity
Majority treated nonoperatively if less than 10 degrees of angulation and no rotational deformity
 Three weeks of immobilization followed by aggressive motion recovery
Three weeks of immobilization followed by aggressive motion recovery
 Radiographic union lags behind clinical union by several weeks.
Radiographic union lags behind clinical union by several weeks.
 Irreducible or unstable fracture patterns may require surgery.
Irreducible or unstable fracture patterns may require surgery.







 Dorsal dislocation—most common
Dorsal dislocation—most common
 Injury to volar plate and at least one collateral ligament
Injury to volar plate and at least one collateral ligament
 “Simple” dislocation—middle phalanx in contact with condyles of proximal phalanx
“Simple” dislocation—middle phalanx in contact with condyles of proximal phalanx


 Volar plate acts as block to reduction if longitudinal traction applied.
Volar plate acts as block to reduction if longitudinal traction applied.
 Reduction via hyperextension of middle phalanx followed by a palmar force
Reduction via hyperextension of middle phalanx followed by a palmar force
 Short-term buddy taping is sufficient aftercare.
Short-term buddy taping is sufficient aftercare.
 Persistent instability is rare but may be treated by dorsal block splinting.
Persistent instability is rare but may be treated by dorsal block splinting.









11. PIP joint fracture-dislocation
 Inappropriate recognition and treatment of these injuries may result in significant functional deficits.
Inappropriate recognition and treatment of these injuries may result in significant functional deficits.
 Dorsal dislocation accompanied by fracture at P2 base (Figure 7-24)
Dorsal dislocation accompanied by fracture at P2 base (Figure 7-24)
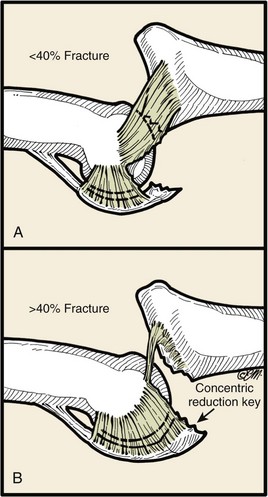
 Hastings classification based on amount of P2 articular surface involvement (Table 7-4)
Hastings classification based on amount of P2 articular surface involvement (Table 7-4)
Table 7-4
Classification of PIP Joint Fracture-Dislocations (Hastings)
| Type | Amount of P2 Articular Surface Involved | Treatment |
| I—Stable | <30% | Dorsally based extension block splint |
| II—Tenuous | 30%-50% | If reducible in flexion, dorsally based extension block splint |
| III—Unstable | >50% | ORIF, hamate autograft, or volar plate arthroplasty |
ORIF, open reduction with internal fixation; PIP, proximal interphalangeal; P2, middle phalanx.
 Treatment options include dorsal block splinting, ORIF, and volar plate arthroplasty.
Treatment options include dorsal block splinting, ORIF, and volar plate arthroplasty.
 Regardless of treatment, maintenance of adequate joint reduction is the most important factor for favorable long-term outcome.
Regardless of treatment, maintenance of adequate joint reduction is the most important factor for favorable long-term outcome.

 Chronic PIP fracture-dislocations are best treated with volar plate arthroplasty or arthrodesis.
Chronic PIP fracture-dislocations are best treated with volar plate arthroplasty or arthrodesis.
12. DIP dislocation and distal phalanx fractures
 DIP dislocation is treated with closed reduction followed by immobilization in slight flexion with a dorsal splint for 2 weeks.
DIP dislocation is treated with closed reduction followed by immobilization in slight flexion with a dorsal splint for 2 weeks.

 May accompany extensive soft tissue and/or nail bed disruption in severe fingertip injuries
May accompany extensive soft tissue and/or nail bed disruption in severe fingertip injuries



 Soft tissue loss treated accordingly
Soft tissue loss treated accordingly

 For further details see the section “Nail and Fingertip Injuries”
For further details see the section “Nail and Fingertip Injuries”
V TENDON INJURIES AND OVERUSE SYNDROMES
1. Description and treatment are based on zones of injury (Figure 7-25).

2. Most commonly injured digit is long finger.
3. Partial lacerations less than 50% of tendon width do not require direct repair if patient can extend finger against resistance.

4. After direct suture repair of complete lacerations or those constituting more than 50% of tendon width, rehabilitation is based on zone of injury.

 Disruption of terminal extensor tendon at or distal to the DIP joint
Disruption of terminal extensor tendon at or distal to the DIP joint
 Sudden forced flexion of the extended fingertip
Sudden forced flexion of the extended fingertip
 Patient cannot actively extend at DIP joint, and finger remains in flexed posture.
Patient cannot actively extend at DIP joint, and finger remains in flexed posture.
 May be accompanied by bony avulsion injury from dorsal base of P3 (bony mallet)
May be accompanied by bony avulsion injury from dorsal base of P3 (bony mallet)

 No consensus on best type of splint to use
No consensus on best type of splint to use
 Hyperextension should be avoided; skin necrosis can occur.
Hyperextension should be avoided; skin necrosis can occur.

 Maintenance of PIP joint motion often overlooked
Maintenance of PIP joint motion often overlooked





 Chronic mallet finger detected more than 12 weeks after injury
Chronic mallet finger detected more than 12 weeks after injury
 Closed treatment only if joint supple, congruent, and without arthritic changes
Closed treatment only if joint supple, congruent, and without arthritic changes


 Prolonged DIP flexion may lead to swan neck deformity (Figure 7-26), caused by dorsal subluxation of lateral bands and corresponding PIP joint hyperextension.
Prolonged DIP flexion may lead to swan neck deformity (Figure 7-26), caused by dorsal subluxation of lateral bands and corresponding PIP joint hyperextension.



 A painful, stiff, arthritic DIP joint is treated with arthrodesis.
A painful, stiff, arthritic DIP joint is treated with arthrodesis.

 Occurs over middle phalanx of digit or over proximal phalanx of thumb
Occurs over middle phalanx of digit or over proximal phalanx of thumb
 Mechanism of injury usually involves a dorsal laceration or crush component.
Mechanism of injury usually involves a dorsal laceration or crush component.
 Partial disruptions (<50%) are treated nonoperatively with local wound care and early mobilization.
Partial disruptions (<50%) are treated nonoperatively with local wound care and early mobilization.
 Direct repair may be attempted for greater than 50% lacerations.
Direct repair may be attempted for greater than 50% lacerations.
 Some surgeons will temporarily pin across terminal joint after direct repair.
Some surgeons will temporarily pin across terminal joint after direct repair.

 Occurs over PIP joint of digit (central slip) or MCP joint of thumb
Occurs over PIP joint of digit (central slip) or MCP joint of thumb
 Open injuries are directly repaired if possible.
Open injuries are directly repaired if possible.

 For closed injuries, the Elson test is performed by flexing the patient’s PIP joint 90 degrees over the edge of a table and asking patient to extend the PIP joint against resistance (Figure 7-27).
For closed injuries, the Elson test is performed by flexing the patient’s PIP joint 90 degrees over the edge of a table and asking patient to extend the PIP joint against resistance (Figure 7-27).
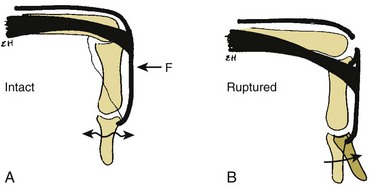
 If the central slip is intact, the DIP joint will remain supple.
If the central slip is intact, the DIP joint will remain supple.
 If the central slip is ruptured, the DIP joint will be rigid.
If the central slip is ruptured, the DIP joint will be rigid.
 An acute boutonniere deformity results from central slip disruption and volar subluxation of the lateral bands, resulting in DIP hyperextension (Figure 7-28).
An acute boutonniere deformity results from central slip disruption and volar subluxation of the lateral bands, resulting in DIP hyperextension (Figure 7-28).
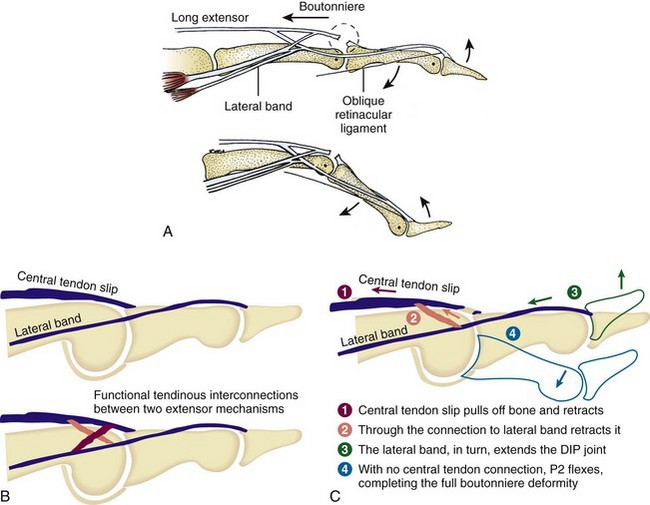



 Chronic (untreated) boutonniere deformity
Chronic (untreated) boutonniere deformity
 May require dynamic splinting or serial casting to achieve maximal passive motion first
May require dynamic splinting or serial casting to achieve maximal passive motion first







 A painful, stiff, arthritic PIP joint is treated with arthrodesis.
A painful, stiff, arthritic PIP joint is treated with arthrodesis.

 Occurs over proximal phalanx of digit or over the metacarpal of thumb
Occurs over proximal phalanx of digit or over the metacarpal of thumb
 Treatment is similar to that for injuries in zone II.
Treatment is similar to that for injuries in zone II.
 A common complication in this zone is adhesion formation, with resulting loss of digital flexion.
A common complication in this zone is adhesion formation, with resulting loss of digital flexion.



 Occurs over MCP joint of digit or over CMC joint of thumb
Occurs over MCP joint of digit or over CMC joint of thumb
 Lacerations involving more than 50% of the tendon substance should be repaired.
Lacerations involving more than 50% of the tendon substance should be repaired.
 Early mobilization and dynamic splinting is advocated.
Early mobilization and dynamic splinting is advocated.
 A fight bite requires surgical débridement of the MCP joint with loose or delayed wound closure.
A fight bite requires surgical débridement of the MCP joint with loose or delayed wound closure.


 A sagittal band rupture (“flea-flicker” injury) may result from forced extension of flexed digit.
A sagittal band rupture (“flea-flicker” injury) may result from forced extension of flexed digit.







 Occurs over metacarpal and represents most frequently injured zone
Occurs over metacarpal and represents most frequently injured zone
 Associated lacerations of superficial veins and nerves are likely.
Associated lacerations of superficial veins and nerves are likely.
 Direct repair is indicated when the disruption constitutes more than 50% of the tendon substance.
Direct repair is indicated when the disruption constitutes more than 50% of the tendon substance.
 Early protected motion advocated postoperatively
Early protected motion advocated postoperatively
 Dynamic splinting may offer better short-term range of motion and strength without increased complications over static splinting.
Dynamic splinting may offer better short-term range of motion and strength without increased complications over static splinting.

 The prognosis is good in the absence of concurrent skeletal injury.
The prognosis is good in the absence of concurrent skeletal injury.

 Zone VII injury occurs at the level of the wrist joint, and zone VIII injury occurs in the distal forearm at the musculotendinous junction.
Zone VII injury occurs at the level of the wrist joint, and zone VIII injury occurs in the distal forearm at the musculotendinous junction.

 The retinaculum should be repaired to prevent tendon bowstringing.
The retinaculum should be repaired to prevent tendon bowstringing.

 The results of surgical repair in these zones are not as good as those in zones IV, V, and VI.
The results of surgical repair in these zones are not as good as those in zones IV, V, and VI.
 This injury usually results from volar lacerations, and concomitant neurovascular injury is common.
This injury usually results from volar lacerations, and concomitant neurovascular injury is common.


 The profundus tendons (middle through small) typically share a common muscle belly so that DIP flexion of each digit must be tested while blocking the other digits in extension.
The profundus tendons (middle through small) typically share a common muscle belly so that DIP flexion of each digit must be tested while blocking the other digits in extension.


 Patial lacerations may be associated with gap formation or triggering with nonoperative treatment.
Patial lacerations may be associated with gap formation or triggering with nonoperative treatment.
 Triggering may be alleviated by trimming tendon ends under flexor tendon sheath.
Triggering may be alleviated by trimming tendon ends under flexor tendon sheath.

 Basic surgical techniques of flexor tendon repair
Basic surgical techniques of flexor tendon repair
 Strength of repair proportional to number of suture strands that cross repair site
Strength of repair proportional to number of suture strands that cross repair site


 A locking-loop configuration decreases gap formation.
A locking-loop configuration decreases gap formation.
 Epitendinous repair decreases gap size and increases overall strength by 10% to 50%.
Epitendinous repair decreases gap size and increases overall strength by 10% to 50%.

 Dorsally placed core sutures are stronger.
Dorsally placed core sutures are stronger.
 Repair of the flexor tendon sheath has no effect on flexor tendon repair.
Repair of the flexor tendon sheath has no effect on flexor tendon repair.
 An atraumatic minimal-touch technique minimizes adhesions.
An atraumatic minimal-touch technique minimizes adhesions.

 Risk of tendon rupture greatest 3 weeks after repair, and failure typically occurs at suture knots.
Risk of tendon rupture greatest 3 weeks after repair, and failure typically occurs at suture knots.

 Use of an active flexion protocol postoperatively requires a minimum four-strand repair with epitendinous suture.
Use of an active flexion protocol postoperatively requires a minimum four-strand repair with epitendinous suture.


 Abundant research continues to be focused on flexor tendon injuries.
Abundant research continues to be focused on flexor tendon injuries.
 No repair tissue matches the strength and stiffness of a normal uninjured tendon.
No repair tissue matches the strength and stiffness of a normal uninjured tendon.
 Intrinsic healing is directed by tendon fibroblasts (tenocytes).
Intrinsic healing is directed by tendon fibroblasts (tenocytes).




 Treatment according to Verdan zones (Figure 7-29)
Treatment according to Verdan zones (Figure 7-29)


 Zone I injury (“rugger jersey” finger)
Zone I injury (“rugger jersey” finger)
 Closed FDP avulsion occurring distal to the FDS insertion
Closed FDP avulsion occurring distal to the FDS insertion
 Mechanism of injury is forced extension of the DIP joint during grasping.
Mechanism of injury is forced extension of the DIP joint during grasping.
 The ring finger is involved in 75% of cases.
The ring finger is involved in 75% of cases.








 Zone II injury (“no man’s land”)
Zone II injury (“no man’s land”)
 Occurs within the flexor tendon sheath between the FDS insertion and the distal palmar crease
Occurs within the flexor tendon sheath between the FDS insertion and the distal palmar crease






 Occurs between the distal palmar crease and the distal end of the carpal tunnel
Occurs between the distal palmar crease and the distal end of the carpal tunnel
 Compared with zone II injuries, the results of direct repair are much better.
Compared with zone II injuries, the results of direct repair are much better.
 Lumbrical muscles originate from the radial aspect of FDP tendons in zone III.
Lumbrical muscles originate from the radial aspect of FDP tendons in zone III.








 Zone I injuries—occur distal to interphalangeal joint
Zone I injuries—occur distal to interphalangeal joint
 Zone II injuries—occur between interphalangeal and MCP joints
Zone II injuries—occur between interphalangeal and MCP joints


 Two most common postoperative rehabilitation protocols are those of Kleinert and Duran.
Two most common postoperative rehabilitation protocols are those of Kleinert and Duran.


 Both programs restrict active flexion for approximately 6 weeks.
Both programs restrict active flexion for approximately 6 weeks.

 These protocols require stronger repair methods, such as the use of more than four core strands.
These protocols require stronger repair methods, such as the use of more than four core strands.











C Stenosing tenosynovitis (trigger finger)
1. Most common in women over 50 years of age
2. Common in diabetic patients and patients with inflammatory arthropathy
3. May simply result from repetitive grasping activities (idiopathic form)
4. Inflammation of the flexor tendon sheath, which inhibits the smooth gliding motion of flexor tendons in the digits or thumb
5. Initially characterized by pain and tenderness at the distal palm near the A1 pulley
6. If left untreated, stenosing tenosynovitis may lead to catching and locking of the digit as the space available for the flexor tendon narrows.
7. Green classification (Table 7-5)
Table 7-5
Classification of Trigger Digit (Green)
| Grade | Description |
| I | Pain and tenderness at the A1 pulley |
| II | Catching of digit |
| III | Locking of digit; passively correctable |
| IV | Fixed, locked digit |
8. Ring finger most common in adults
9. Many respond to corticosteroid injection into flexor tendon sheath.


10. Failure of nonoperative management treated surgically with release of A1 pulley








1. Attritional and degenerative condition affecting the first extensor compartment (APL/EPB)
2. Commonly affects middle-age women
3. Other high-risk groups—new mothers, golfers, and racquet-sport athletes
4. Dorsoradial wrist tenderness, swelling, crepitus
5. Finkelstein test and/or Eichoff maneuver places first extensor compartment tendons under maximum tension and exacerbates symptoms.
6. Nonoperative management includes rest, activity modification, thumb spica splinting/bracing, nonsteroidal anti-inflammatory drugs (NSAIDs), and corticosteroid injections into the first dorsal extensor compartment.

7. When these measures fail, surgical release of the first extensor compartment may be performed.





1. Tenosynovitis and/or bursitis occurring at the junction between the first and second extensor compartments, where APL and EPB tendons cross ECRL and ECRB
2. Affects rowers, weight lifters, football lineman, martial artists, and golfers
3. Tenderness, swelling, and crepitus are localized to an area approximately 4 to 5 cm proximal to the radiocarpal joint.
4. Initially treated with ice, splinting, NSAIDs, corticosteroid injection into the second extensor compartment
5. When nonoperative measures fail, surgical release of the second extensor compartment and débridement of inflamed bursae may be effective.
1. Overuse syndrome from repetitive resisted wrist flexion
2. Most frequently described for FCU but may also involve FCR
3. Acute onset of wrist pain, swelling, and discoloration that mimics infection or crystalline arthropathy in severity
4. Fluffy calcium deposits may be detected on plain radiographs
5. Usually responds to short course of oral steroids or high-dose NSAIDs, ice, and immobilization
G ECU tendonitis and subluxation
1. ECU tendon held tightly within a groove in the distal ulna, tethered by a fibroosseous sheath
2. Overuse tendonitis often affects racquet-sport athletes.
3. MRI may reveal thickening (hypertrophy), partial longitudinal tears, or generalized increased signal intensity within tendon.
4. Nonoperative management with rest, activity modification, splinting, NSAIDs, and corticosteroid injections recommended
5. Traumatic subluxation of ECU tendon may result from forceful hypersupination and ulnar deviation of wrist.




VI DISTAL RADIOULNAR JOINT, TRIANGULAR FIBROCARTILAGE COMPLEX, AND WRIST ARTHROSCOPY
1. Radius rotates about a fixed ulna at the DRUJ.
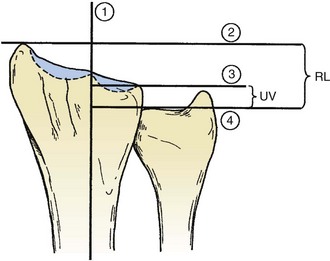
2. Ulnar variance measures the distance in millimeters between the distal aspect of the ulnar head and the articular surface of the distal radius (Figure 7-31).


3. The TFCC stabilizes the DRUJ and transmits 20% of axial load at the wrist (neutral ulnar variance).
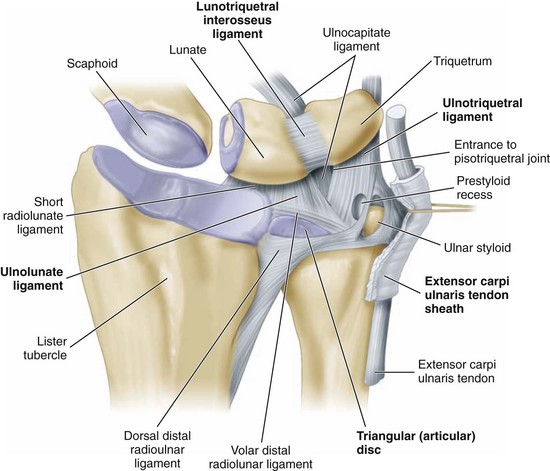
4. Components of the TFCC include the dorsal and volar radioulnar ligaments, the articular disc, a meniscus homologue, the ECU subsheath, and the origins of the ulnolunate and ulnotriquetral ligaments.
5. Periphery is well vascularized, whereas the radial central portion is relatively avascular (Figure 7-32).


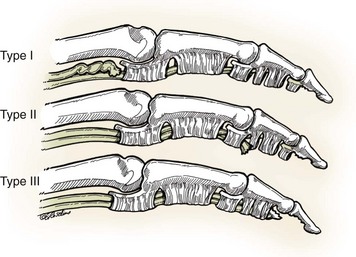
1. Classified as traumatic (class I) or degenerative (class II)
2. Further divided by Palmer into subtypes based on the specific location within the complex (Tables 7-6 and 7-7)
Table 7-6
Class I: Traumatic TFCC Injuries
| Class | Characteristics | Treatment |
| IA | Central perforation or tear | Resection of an unstable flap back to a stable rim |
| IB | Ulnar avulsion with or without ulnar styloid fracture | Repair of the rim to its origin at the ulnar styloid |
| IC | Distal avulsion (origins of UL and UT ligaments) | Advancement of the distal volar rim to the triquetrum (bone anchor) |
| ID | Radial avulsion (involving the dorsal and/or volar radioulnar ligaments) | Direct repair to the radius to preserve the TFCC contribution to DRUJ stability |
Table 7-7
Class II: Degenerative TFCC Tears (Ulnocarpal Impaction Syndrome)
| Class | Characteristics |
| IIA | TFCC wear (thinning) |
| IIB | IIA + lunate and/or ulnar chondromalacia |
| IIC | TFCC perforation + lunate and/or ulnar chondromalacia |
| IID | IIC + LT ligament disruption |
| IIE | IID + ulnocarpal and DRUJ arthritis |
DRUJ, distal radioulnar joint; LT, lunotriquetral; TFCC, triangular fibrocartilage complex.
3. Class and location of the tear have important implications for treatment.
4. Value of MRI is increasing with regard to overall detection and localization of TFCC pathology.
5. All acute traumatic TFCC injuries are initially managed with immobilization and NSAIDs.
6. When nonoperative management fails to relieve persistent symptoms, wrist arthroscopy and/or open repair is indicated.
7. Arthroscopic trampoline test is performed to assess TFCC resiliency by balloting central portion with small probe.

 Central class IA tears are inherently stable and may simply be débrided when persistently symptomatic.
Central class IA tears are inherently stable and may simply be débrided when persistently symptomatic.

 Peripheral class IB tears are amenable to arthroscopic or open repair.
Peripheral class IB tears are amenable to arthroscopic or open repair.
 Concurrent fractures of ulnar styloid with persistent instability are either excised or internally fixed.
Concurrent fractures of ulnar styloid with persistent instability are either excised or internally fixed.
 Rare class IC tears are managed by either arthroscopic or open repair.
Rare class IC tears are managed by either arthroscopic or open repair.



 Degenerative class II tears are associated with positive ulnar variance, increased ulnocarpal loading, and ulnocarpal impaction syndrome from abutment of the ulnar head into the proximal carpal row.
Degenerative class II tears are associated with positive ulnar variance, increased ulnocarpal loading, and ulnocarpal impaction syndrome from abutment of the ulnar head into the proximal carpal row.
 Patients present with chronic ulnar-sided wrist pain, increased with forearm rotation and grip.
Patients present with chronic ulnar-sided wrist pain, increased with forearm rotation and grip.
 Pain with loading wrist in extension and ulnar deviation
Pain with loading wrist in extension and ulnar deviation

 When conservative management fails, the goal of surgery is reduction of ulnocarpal loading.
When conservative management fails, the goal of surgery is reduction of ulnocarpal loading.



C DRUJ instability and post-traumatic osteoarthritis
 Acute dislocation of DRUJ can occur alone or in combination with ulnar styloid (base), radial shaft (Galeazzi), or Essex-Lopresti injuries.
Acute dislocation of DRUJ can occur alone or in combination with ulnar styloid (base), radial shaft (Galeazzi), or Essex-Lopresti injuries.
 Isolated dislocations may be treated by closed reduction and immobilization.
Isolated dislocations may be treated by closed reduction and immobilization.
 Closed reduction may be impeded by interposition of the ECU tendon.
Closed reduction may be impeded by interposition of the ECU tendon.
 Concurrent distal ulna fractures and TFCC tears may require open or arthroscopic treatment.
Concurrent distal ulna fractures and TFCC tears may require open or arthroscopic treatment.
 In a Galeazzi injury, ORIF of the radial shaft is followed by assessment of DRUJ stability.
In a Galeazzi injury, ORIF of the radial shaft is followed by assessment of DRUJ stability.
 An unstable DRUJ may require TFCC repair and/or temporary radioulnar pinning proximal to the joint with the forearm immobilized in relative supination.
An unstable DRUJ may require TFCC repair and/or temporary radioulnar pinning proximal to the joint with the forearm immobilized in relative supination.











1. Indicated for the diagnosis of unexplained wrist pain





3. May assist in the treatment of distal radius and scaphoid fractures
4. Traction tower, 2.7-mm 30-degree arthroscope
5. Arthroscopic portals (Figure 7-33)
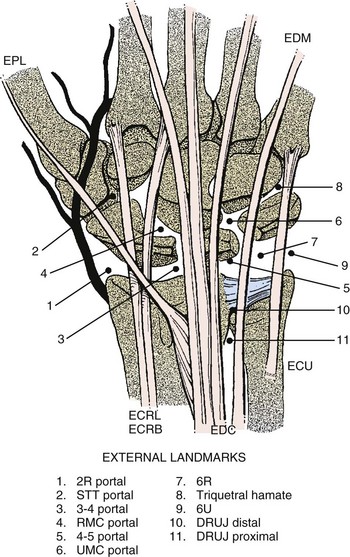
6. Radiocarpal and midcarpal joint inspected systematically
7. Injury to superficial sensory nerves is most common complication.
VII NAIL AND FINGERTIP INJURIES
1. Fingertip injuries are most common hand injuries seen in emergency departments.
2. Long finger is most commonly involved digit.
3. These injuries may be broadly classified as those with and those without soft tissue loss.
4. Crush injuries without extensive soft tissue loss may result in nail plate avulsions, nail matrix lacerations, and distal phalanx (tuft) fractures.
5. Distal phalanx fractures are typically reduced when the nail bed is repaired, but large, displaced fragments may require percutaneous pinning.
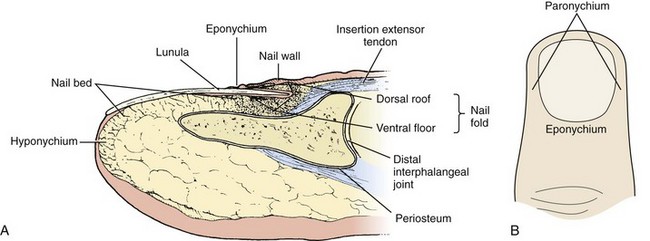
1. Nail plate is composed of keratin and originates from germinal matrix proximal to nail fold.
2. Sterile matrix lies directly beneath nail plate and contributes keratin to increase plate thickness.
3. Crescent-shaped white lunula is seen through proximal nail plate at junction of sterile and germinal matrices.
4. Hyponychium lies between distal nail bed and skin of fingertip, serving as a barrier to microorganisms.
5. The eponychium, also called the cuticle, is at distal margin of proximal nail fold.
1. A small subungual hematoma constituting less than 50% of nail area may be treated without nail plate removal.

2. Subungual hematomas greater than 50% of nail area require nail plate removal for repair of underlying nail matrix lacerations.
 Acute repair offers best results.
Acute repair offers best results.
 Tetanus prophylaxis and antibiotics given
Tetanus prophylaxis and antibiotics given

 If it is still available, the nail plate is removed and soaked in Betadine.
If it is still available, the nail plate is removed and soaked in Betadine.




3. If significant nail matrix has been lost, options include a split-thickness matrix graft from an adjacent injured finger or transfer of the nail matrix from second toe.
4. Nail plate deformities, especially nail ridging, are very common after crush injuries and nail bed repair.
5. A hook nail may result from a tight nail bed repair, distal advancement of the matrix, or loss of underlying bony support.
6. Patients should be counseled about high incidence of fingertip hypersensitivity and/or cold intolerance for up to 1 year.
7. Complete growth of a new nail plate takes 3 to 6 months, depending on the age of the patient.
D Fingertip injuries with tissue loss
1. Treatment of these injuries may be time intensive and challenging.
2. The general principles of treatment include preservation of digit length, maintenance of sensate fingertip pulp, prevention of joint contracture, and eventual pain-free use of digit.
3. The correct characterization of the injury is critical and guides treatment.
 Fingertip injuries without exposed bone
Fingertip injuries without exposed bone
 These may be allowed to heal by secondary intention if less than 1 cm2 of the tip or pulp is involved.
These may be allowed to heal by secondary intention if less than 1 cm2 of the tip or pulp is involved.


 Fingertip injuries with exposed bone
Fingertip injuries with exposed bone
 Characterized by the orientation of tissue loss
Characterized by the orientation of tissue loss


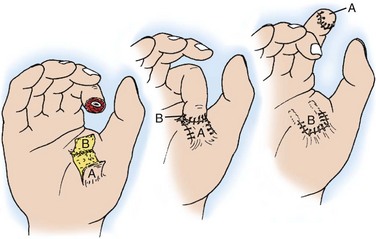
 Dorsal skin and subcutaneous tissue elevated superficial to the paratenon from adjacent digit to create a bed for the injured fingertip
Dorsal skin and subcutaneous tissue elevated superficial to the paratenon from adjacent digit to create a bed for the injured fingertip
 Donor site is covered with a split-thickness skin graft.
Donor site is covered with a split-thickness skin graft.
 The flap is split during a separate procedure 2 to 3 weeks later (Figure 7-35).
The flap is split during a separate procedure 2 to 3 weeks later (Figure 7-35).
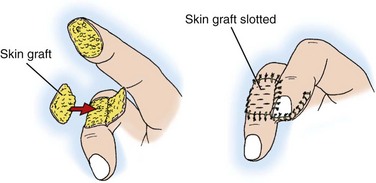

 Best reserved for volar oblique injuries to the index or long digits
Best reserved for volar oblique injuries to the index or long digits
 Flap is lifted parallel to the proximal thumb crease and split after 2 to 3 weeks (Figure 7-36).
Flap is lifted parallel to the proximal thumb crease and split after 2 to 3 weeks (Figure 7-36).







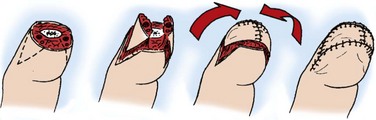
 Transverse or dorsal oblique digit injury
Transverse or dorsal oblique digit injury

 May be performed to preserve length and cover transverse or dorsal oblique fingertip injuries
May be performed to preserve length and cover transverse or dorsal oblique fingertip injuries

 Flap is advanced over the fingertip toward the dorsal side, and a tension-free closure is made (Figure 7-37).
Flap is advanced over the fingertip toward the dorsal side, and a tension-free closure is made (Figure 7-37).

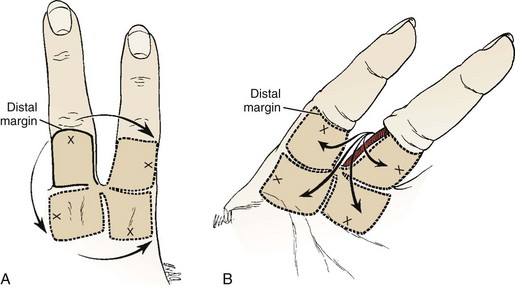
 Kutler popularized two separate smaller V-Y advancements from the lateral aspects of the digit to cover transverse fingertip injuries (Figure 7-38).
Kutler popularized two separate smaller V-Y advancements from the lateral aspects of the digit to cover transverse fingertip injuries (Figure 7-38).













VIII SOFT TISSUE COVERAGE AND MICROSURGERY
 Management begins with thorough assessment of wound, including size, location, involvement of deep structures, and presence of contamination.
Management begins with thorough assessment of wound, including size, location, involvement of deep structures, and presence of contamination.
 Standard of care involves early débridement and administration of antibiotics.
Standard of care involves early débridement and administration of antibiotics.
 Complex wounds may require several surgical débridements to remove nonviable tissue.
Complex wounds may require several surgical débridements to remove nonviable tissue.
 A clean wound bed is essential before any definitive coverage procedure.
A clean wound bed is essential before any definitive coverage procedure.
 Infection rates increase dramatically if coverage is delayed longer than 1 week after injury.
Infection rates increase dramatically if coverage is delayed longer than 1 week after injury.
 Goals of soft tissue reconstruction
Goals of soft tissue reconstruction



 Options for soft tissue reconstruction
Options for soft tissue reconstruction




 Choice of definitive procedure is guided by wound characteristics and patient factors.
Choice of definitive procedure is guided by wound characteristics and patient factors.





 Autografts may be either split-thickness skin grafts or full-thickness skin grafts.
Autografts may be either split-thickness skin grafts or full-thickness skin grafts.
 Both types require clean wound bed without exposed bone or tendon.
Both types require clean wound bed without exposed bone or tendon.
 Skin grafts are prone to early failure from shear stress and hematoma formation.
Skin grafts are prone to early failure from shear stress and hematoma formation.





 Preferred for volar hand and fingertip wounds
Preferred for volar hand and fingertip wounds
 More durable, contract less, and provide better sensibility
More durable, contract less, and provide better sensibility

 Proximal forearm, medial arm and hypothenar aspect of the hand are common donor sites.
Proximal forearm, medial arm and hypothenar aspect of the hand are common donor sites.
 Allografts may be used as temporary measure to prepare a wound bed for later autografting.
Allografts may be used as temporary measure to prepare a wound bed for later autografting.


 A flap is a unit of tissue supported by blood vessels and moved from a donor site to a recipient site to cover a defect.
A flap is a unit of tissue supported by blood vessels and moved from a donor site to a recipient site to cover a defect.

 Transfer of vascularized tissue promotes healing and lowers the secondary infection rate.
Transfer of vascularized tissue promotes healing and lowers the secondary infection rate.

 Flaps may be classified by their vascular supply, tissue type, donor site, and method of transfer.
Flaps may be classified by their vascular supply, tissue type, donor site, and method of transfer.
 Flap classification by blood supply
Flap classification by blood supply









 Flap classification by tissue type
Flap classification by tissue type








 Cutaneous flaps include skin and subcutaneous tissue.
Cutaneous flaps include skin and subcutaneous tissue.

 Fasciocutaneous flaps include fascia with overlying skin and subcutaneous tissue.
Fasciocutaneous flaps include fascia with overlying skin and subcutaneous tissue.

 Musculocutaneous flaps include muscle with the overlying skin, subcutaneous tissue, and fascia.
Musculocutaneous flaps include muscle with the overlying skin, subcutaneous tissue, and fascia.

 Osteocutaneous flap composed of a portion of bone with overlying soft tissue
Osteocutaneous flap composed of a portion of bone with overlying soft tissue

 Innervated flaps preserve the nerve supply with the tissue unit.
Innervated flaps preserve the nerve supply with the tissue unit.

 Flap classification by donor site
Flap classification by donor site
 Local flap—provided by tissue adjacent to or near the defect
Local flap—provided by tissue adjacent to or near the defect
 Transposition flaps are geometric in design and may be either axial or random pattern with regard to blood supply.
Transposition flaps are geometric in design and may be either axial or random pattern with regard to blood supply.


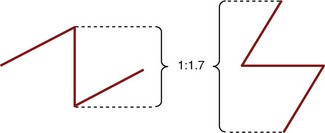
 Theoretically 30 degrees, 45 degrees, 60 degrees yields 25%, 50%, 75% lengthening, respectively, along the line of the central limb (Figure 7-40).
Theoretically 30 degrees, 45 degrees, 60 degrees yields 25%, 50%, 75% lengthening, respectively, along the line of the central limb (Figure 7-40).
 Rotation flaps are not geometric and are universally random pattern with regard to blood supply.
Rotation flaps are not geometric and are universally random pattern with regard to blood supply.
 Length of rotated flap should not exceed the width of its base, for doing so will exceed the capacity of the microcirculation to maintain tissue viability.
Length of rotated flap should not exceed the width of its base, for doing so will exceed the capacity of the microcirculation to maintain tissue viability.
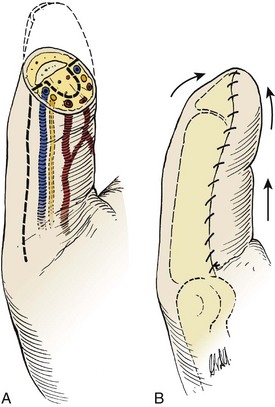
 Advancement flaps such as V-Y and Moberg types proceed in straight line to fill defect.
Advancement flaps such as V-Y and Moberg types proceed in straight line to fill defect.
 Axial flag flaps are based on the dorsal digital artery (Figure 7-41).
Axial flag flaps are based on the dorsal digital artery (Figure 7-41).








 Flap classification by method of transfer
Flap classification by method of transfer
 Flap reconstruction may be performed in a single stage or in two stages, like the previously mentioned abdominal or groin pocket flap.
Flap reconstruction may be performed in a single stage or in two stages, like the previously mentioned abdominal or groin pocket flap.
 In most instances, the donor tissue remains attached to the native vasculature.
In most instances, the donor tissue remains attached to the native vasculature.


 Most frequently used donors for use in the upper extremity include
Most frequently used donors for use in the upper extremity include
 Gracilis (medial femoral circumflex artery)
Gracilis (medial femoral circumflex artery)
 Latissimus dorsi (thoracodorsal artery)
Latissimus dorsi (thoracodorsal artery)
 Serratus anterior (the serratus branch of the subscapular artery)
Serratus anterior (the serratus branch of the subscapular artery)
 Anterolateral thigh (descending branch of lateral femoral circumflex artery)
Anterolateral thigh (descending branch of lateral femoral circumflex artery)

 Patients typically monitored postoperatively in intensive care unit
Patients typically monitored postoperatively in intensive care unit
 The room is kept warm for vasodilation.
The room is kept warm for vasodilation.
 Main cause of free-flap failure is inadequate arterial blood flow.
Main cause of free-flap failure is inadequate arterial blood flow.
 Persistent vasospasm may lead to thrombosis at the anastomosis.
Persistent vasospasm may lead to thrombosis at the anastomosis.
 Hypotension must be avoided and the patient kept well hydrated.
Hypotension must be avoided and the patient kept well hydrated.
 Vasoconstrictive agents such as nicotine and caffeine are restricted.
Vasoconstrictive agents such as nicotine and caffeine are restricted.

B Traumatic upper extremity amputation
1. Indications and contraindications
 Primary indications to attempt replantation
Primary indications to attempt replantation




 Relative indication is a level distal to the FDS insertion (zone I).
Relative indication is a level distal to the FDS insertion (zone I).







 Part should be wrapped in moist gauze (normal saline or lactated Ringer solution) and placed within a sealed plastic bag, which is then placed in an ice-water bath.
Part should be wrapped in moist gauze (normal saline or lactated Ringer solution) and placed within a sealed plastic bag, which is then placed in an ice-water bath.


3. Operative sequence of replantation
















 Most reliable methods are close observation of color, capillary refill, and tissue turgor.
Most reliable methods are close observation of color, capillary refill, and tissue turgor.

 Either a drop in temperature of more than 2° C in 1 hour or a temperature of less than 30° C indicates decreased digital perfusion.
Either a drop in temperature of more than 2° C in 1 hour or a temperature of less than 30° C indicates decreased digital perfusion.
 Others advocate placement of implantable venous Doppler probe.
Others advocate placement of implantable venous Doppler probe.

 Most frequent cause of early (within 12 hours) replantation failure is arterial thrombosis from persistent vasospasm.
Most frequent cause of early (within 12 hours) replantation failure is arterial thrombosis from persistent vasospasm.
 Arterial insufficiency suggested by pale skin color, decreased or absent capillary refill, loss of Doppler-measurable signal.
Arterial insufficiency suggested by pale skin color, decreased or absent capillary refill, loss of Doppler-measurable signal.

 If these measures fail, exploration and attempt at reanastomosis warranted
If these measures fail, exploration and attempt at reanastomosis warranted
 Failure after 12 hours is typically secondary to venous congestion or thrombosis.
Failure after 12 hours is typically secondary to venous congestion or thrombosis.
 Venous insufficiency suggested by ruborous skin color, increased capillary refill, tissue engorgement
Venous insufficiency suggested by ruborous skin color, increased capillary refill, tissue engorgement
 May subsequently diminish arterial inflow
May subsequently diminish arterial inflow
 Remove dressings and elevate extremity.
Remove dressings and elevate extremity.






 Late complications include tendon adhesions, bone nonunion, and neuroma formation.
Late complications include tendon adhesions, bone nonunion, and neuroma formation.

 Factor most predictive of digit survival after replantation is mechanism of injury.
Factor most predictive of digit survival after replantation is mechanism of injury.
 Next most important factor is probably ischemia time.
Next most important factor is probably ischemia time.




8. Forearm and arm replantation
 Arterial inflow established before skeletal stabilization with the use of shunts, if necessary, to minimize ischemia time
Arterial inflow established before skeletal stabilization with the use of shunts, if necessary, to minimize ischemia time
 Post replantation fasciotomies performed to prevent reperfusion-induced compartment syndrome
Post replantation fasciotomies performed to prevent reperfusion-induced compartment syndrome
 Muscle necrosis may lead to myoglobinuria and life-threatening renal failure.
Muscle necrosis may lead to myoglobinuria and life-threatening renal failure.
 Elevated postoperative serum potassium level may be prognostic of replantation failure.
Elevated postoperative serum potassium level may be prognostic of replantation failure.

 Controversial procedure that introduces potentially life-threatening complications from postoperative immunosuppression for a condition that is not itself life threatening
Controversial procedure that introduces potentially life-threatening complications from postoperative immunosuppression for a condition that is not itself life threatening

 Bilateral transplants have been performed with good survivorship, including one above the elbow.
Bilateral transplants have been performed with good survivorship, including one above the elbow.
 Newer immunosuppressive protocols are less toxic and may lead to less long-term morbidity.
Newer immunosuppressive protocols are less toxic and may lead to less long-term morbidity.
 Still debatable whether this tremendously expensive endeavor is superior to an upper limb prosthetic
Still debatable whether this tremendously expensive endeavor is superior to an upper limb prosthetic