Rosacea
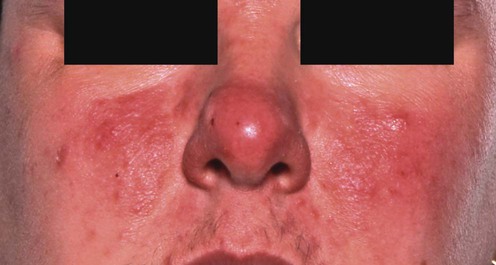


Inflammatory rosacea
First-line treatments
 Topical metronidazole Topical metronidazole |
A |
 Topical azelaic acid Topical azelaic acid |
A |
 Oral tetracyclines Oral tetracyclines |
A |
 Oral erythromycin Oral erythromycin |
C |
 Emollients Emollients |
C |
Second-line treatments
 Topical erythromycin
Topical erythromycin Topical clindamycin
Topical clindamycin Oral metronidazole
Oral metronidazole Topical benzoyl peroxide
Topical benzoyl peroxide Ampicillin
Ampicillin Azithromycin
AzithromycinThird-line treatments
 Systemic isotretinoin
Systemic isotretinoin Topical tretinoin
Topical tretinoin Topical adapalene
Topical adapalene Topical sulfur
Topical sulfur Topical corticosteroids
Topical corticosteroids Topical ketoconazole
Topical ketoconazole Systemic ketoconazole
Systemic ketoconazole Topical bifonazole
Topical bifonazole Photodynamic therapy
Photodynamic therapy Spironolactone
Spironolactone Demodex eradication
Demodex eradication Helicobacter pylori eradication
Helicobacter pylori eradication Sunscreens
Sunscreens Topical tacrolimus
Topical tacrolimus Topical pimecrolimus
Topical pimecrolimus Octreotide
Octreotide Inhibition of ovulation
Inhibition of ovulation Topical NADH
Topical NADH Topical 1-methylnicotinamide
Topical 1-methylnicotinamide Oral nicotinamide with zinc
Oral nicotinamide with zinc Zinc sulphate
Zinc sulphate Trichloroacetic acid peels
Trichloroacetic acid peels
Erythematotelangiectatic rosacea
First-line therapies
 Brimonidine tartrate
Brimonidine tartrate Oxymetazoline
Oxymetazoline Cosmetic camouflage
Cosmetic camouflage Intense pulsed light
Intense pulsed light Vascular lasers
Vascular lasers Ondansetron
Ondansetron
Rosacea flushing
First-line therapies
 Clonidine
Clonidine Rilmenidine
Rilmenidine β-Blockers
β-Blockers Naloxone
Naloxone Cosmesis
Cosmesis Pulsed dye laser
Pulsed dye laser Intense pulsed light
Intense pulsed light Hypnosis
Hypnosis Granisetron
GranisetronRosacea lymphedema (morbihan’s disease)
First-line therapies
 Broad-spectrum antibiotics
Broad-spectrum antibiotics Facial massage
Facial massage Isotretinoin with ketotifen and H1 antagonist
Isotretinoin with ketotifen and H1 antagonist Prednisolone with metronidazole
Prednisolone with metronidazole CO2 laser blepharoplasty
CO2 laser blepharoplasty Surgical debulking of the eyelids
Surgical debulking of the eyelids Prednisolone and doxycycline
Prednisolone and doxycyclineOcular rosacea
First-line therapies
 Tear substitutes, e.g., carbomers, liquid paraffin, hypromellose
Tear substitutes, e.g., carbomers, liquid paraffin, hypromellose Oral tetracyclines
Oral tetracyclines Topical cyclosporine
Topical cyclosporine Fusidic acid (topical)
Fusidic acid (topical) Helicobacter pylori eradication
Helicobacter pylori eradication Ondansetron
Ondansetron
 Systemic corticosteroids
Systemic corticosteroids Topical corticosteroids
Topical corticosteroids Isotretinoin
Isotretinoin Systemic antibiotics
Systemic antibiotics