Operating room fires
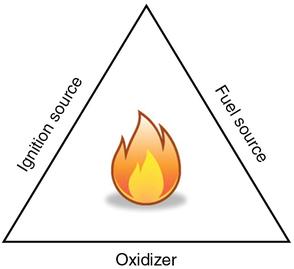
Fire triangle
For a fire to occur, three elements must come together: (1) an oxidizer, (2) fuel, and (3) an ignition source. These three elements are commonly called the “fire triad” and can be represented as a “fire triangle” (Figure 4-1). An OR fire can be prevented by removing any one element of the triangle.
The two oxidizing agents most prevalent in the OR are oxygen (O2) and nitrous oxide (N2O). In the OR, many potential fuel sources are present (Box 4-1). The most common ignition source is diathermy or electrocautery with other ignition sources listed in Box 4-1.
Prevention
General OR fire prevention strategies are summarized in Box 4-2 and involve minimizing or avoiding oxidizer-enriched atmospheres, fuels or ignition sources. A useful strategy for prevention of an OR fire is the identification of a high risk procedure, (i.e., a procedure in which an ignition source will be used in proximity to an oxidizer-enriched environment). The presence of an oxidizer (O2 and N2O) lowers the combustion threshold and increases the intensity of a fire. This oxidizer-enriched atmosphere exists in (and around) the patient’s breathing circuit and the risk of fire is increased in these areas. The risk of ignition is magnified when certain procedures (e.g., electrosurgery during tracheostomy, cauterization of airway lesions) are performed in close proximity to this environment. A number of techniques can be employed to reduce the fire risk during these high-risk procedures (Box 4-3).
Management of an operating room fire
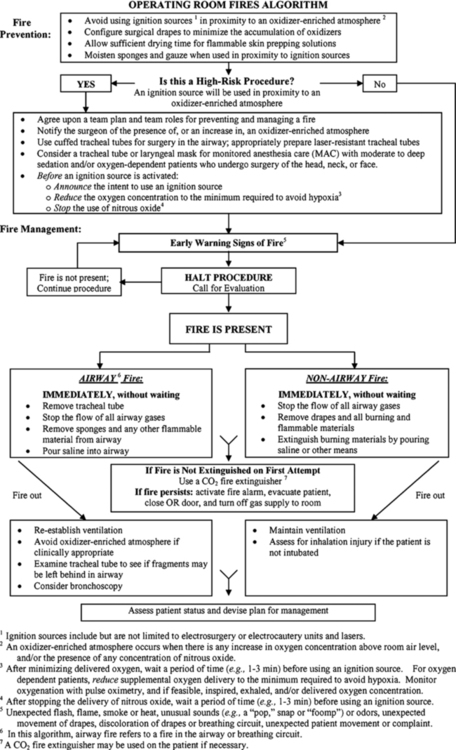
An overall strategy for management of an OR fire has been developed by the American Society of Anesthesiologists (Figure 4-2). Once a fire is detected, the surgical procedure should be immediately halted and all OR personnel and appropriate external resources should be notified.