Obstetric Issues, Labor, and Delivery
Amniocentesis is a procedure that involves the aspiration of amniotic fluid from the amniotic sac during pregnancy. It is generally carried out with a spinal needle (20–22 gauge) in a transabdominal approach, using a sterile technique under continuous ultrasound guidance. ∗
In Rh and other blood group isoimmunizations, amniocentesis has traditionally been used for bilirubin assessment using ΔOD 450, but it is being done far less frequently now because middle cerebral artery Doppler has been found to be extremely accurate in predicting the degree of fetal anemia. In this setting amniocentesis is used to determine whether the fetus is Rh positive or positive for the sensitized antigen so that testing can be avoided if the fetus is not at risk. ∗
3. What are the complications of amniocentesis?
 Miscarriage and fetal loss (less than 0.1%) above the background rate of spontaneous loss (0.5–1%) in specialized centers with high procedure volumes (Eddleman, Towner). The rate is higher in low-volume centers (Tabor).
Miscarriage and fetal loss (less than 0.1%) above the background rate of spontaneous loss (0.5–1%) in specialized centers with high procedure volumes (Eddleman, Towner). The rate is higher in low-volume centers (Tabor).
 Transient leakage of amniotic fluid (about 1%)
Transient leakage of amniotic fluid (about 1%)
 Persistent rupture of membranes (rare)
Persistent rupture of membranes (rare)


 Failure to achieve diagnosis (i.e., cell culture failure, which occurs in 1% of cases)
Failure to achieve diagnosis (i.e., cell culture failure, which occurs in 1% of cases)
 Increased Rhesus isoimmunization, especially if the placenta is transversed. In Rh-negative women, Rh immune globulin (e.g., RhoGAM) is given to prevent sensitization. ∗†‡
Increased Rhesus isoimmunization, especially if the placenta is transversed. In Rh-negative women, Rh immune globulin (e.g., RhoGAM) is given to prevent sensitization. ∗†‡
5. What options, aside from amniocentesis, are available for prenatal diagnosis?
 Available tests for fetal chromosome evaluation are classified as “diagnostic” (the result is a definitive karyotype) or “screening” (the result quantifies the risk of aneuploidy).
Available tests for fetal chromosome evaluation are classified as “diagnostic” (the result is a definitive karyotype) or “screening” (the result quantifies the risk of aneuploidy).





 KEY POINTS: AMNIOCENTESIS AND GENETIC DIAGNOSIS
KEY POINTS: AMNIOCENTESIS AND GENETIC DIAGNOSISmarker” (alpha-fetoprotein (AFP), hCG, estriol) or “quadruple marker” (triple marker plus inhibin-A) at 15 to 20 weeks’ gestation. Depending on which combination of tests is performed, detection of Down syndrome is 60% to 95% with a 5% screen positive rate. Reasonable detection rates are also achieved for trisomy 18 and open neural tube defects. ∗†‡§¶ ∗∗††
∗∗††
Third-trimester hemorrhage refers to any bleeding from the genital tract during the third trimester of pregnancy. In practice, it refers to any bleeding that occurs from the time of viability, (i.e., 23 to 24 weeks’ gestation). The common causes are classified as placenta previa (7%), placental abruption (13%), and other bleeding (80%), including local lesions of the lower genital tract, vasa previa, early labor, trauma, neoplasia, and marginal placental separation. Such bleeding complicates about 6% of pregnancies. ∗
Ultrasound visualization is the method of choice for diagnosis of placenta previa. Multiple reports show a transvaginal approach to be safe and superior in its accuracy compared with transabdominal ultrasound. ∗


















Placental abruption is the separation of the normally implanted placenta before the birth of the fetus. It results from bleeding from a small arterial vessel into the decidua basalis. It is termed a revealed abruption when vaginal bleeding is present (90%) and a concealed abruption if no bleeding is visible (10%). It is uniquely dangerous to the fetus and the mother because of its serious pathophysiologic sequelae. The incidence varies but averages about 0.83% or 1 in 120 deliveries. Abruption severe enough to cause fetal death is less common (approximately 1 in 420 deliveries). ∗†
14. What are the main risk factors for a placental abruption? Is placental abruption a recurrent disease?
















Fetal and neonatal complications
 IUGR: especially in preterm deliveries
IUGR: especially in preterm deliveries
 Increased risk of congenital malformations: 4.4%
Increased risk of congenital malformations: 4.4%




Fetomaternal hemorrhage is caused by a disruption of the normal barrier at the placental-decidual interface. It may occur with abruptio placentae; however, it occurs more commonly with abruptio placentae associated with maternal trauma, with maternal trauma without abruptio placentae, or spontaneously without an apparent precipitating event. Approximately 5% of stillbirths without apparent cause are the result of fetomaternal hemorrhage. The diagnosis is made by performing a Kleihauer–Betke test on maternal blood, which allows quantification of fetal cells in maternal serum. In patients with spontaneous fetomaternal hemorrhage, the presenting symptom is decreased fetal movement. If the fetus is still alive and the hemorrhage is severe enough, the diagnosis is often made because of a sinusoidal fetal heart rate (FHR) tracing. Treatment can consist of immediate delivery if the fetus is near term or intrauterine transfusion if the fetus is premature and no abruption is apparent. ∗
 KEY POINTS: THIRD-TRIMESTER HEMORRHAGE
KEY POINTS: THIRD-TRIMESTER HEMORRHAGE
1. Bleeding at any time during pregnancy is cause for concern and should always be carefully investigated.
2. During the third trimester, however, onset of hemorrhage may be particularly ominous.
3. Some of the diagnoses that should be considered include placenta previa, placental abruption, marginal placental separation, and lesions of the lower genital tract.
4. Approximately 6% of all pregnancies, however, will have some bleeding.
17. A 32-year-old, G2P1001 woman at term gestation presents in labor. Her membranes are intact, she is afebrile, and the fetal heart tracing is reassuring. Reviewing her prenatal records, you notice that she had a positive Group B streptococcal culture obtained at 34 weeks’ gestation. She is allergic to penicillin and “had difficulty breathing and swelled up” when she received it many years ago. What therapy is appropriate?
For pencillin-allergic women with high risk of anaphylaxis (as in the present case), the CDC’s 2010 guidelines recommend susceptibility testing against both erythromycin and clindamycin. Prophylaxis with erythromycin is no longer recommended, even if sensitivity is documented. Prophylaxis with clindamycin is recommended if GBS is proved sensitive to both clindamycin and erythromycin and if there is no inducible resistance to clindamycin using D-zone testing. If sensitivity is unknown, or if all these requirements are not met, vancomycin is recommended. ∗†‡
18. What are the major risk factors for preterm labor?




 Preterm premature rupture of membranes
Preterm premature rupture of membranes
 Maternal age younger than 18 years
Maternal age younger than 18 years

 Diethylstilbestrol (DES) exposure
Diethylstilbestrol (DES) exposure





 KEY POINTS: PRETERM LABOR
KEY POINTS: PRETERM LABOR
1. One of the most difficult problems with preterm labor is simply making the diagnosis.
2. Many women, believing that they are not yet due to deliver, ignore subtle symptoms of preterm labor until it is too late to intervene.
3. In some women, however, cervical dilation may occur in the absence of contractions, eliminating the possible use of tocolytic agents.
4. One of the most important new therapies for preventing preterm labor appears to be the use of progesterone for women who have previously delivered a preterm infant.












Fetal fibronectin is an extracellular matrix protein, the presence of which in cervicovaginal secretions is a predictor of preterm birth. This predictor has a high negative predictive accuracy (>99% negative predictive value; i.e., the absence of fetal fibronectin indicates <1% chance of delivery within 2 weeks) but only a mediocre positive predictive accuracy. ∗†
Most commonly, this test is used in patients with preterm contractions in which the diagnosis of preterm labor is uncertain. A negative test result allows greater than 99% reassurance that the patient will not deliver in the next 2 weeks and often prevents unnecessary treatment. ∗
23. What are the common pharmacologic agents used for the inhibition of preterm labor and their mechanisms of action?
TABLE 3-1
COMMON PHARMACOLOGIC AGENTS USED FOR THE INHIBITION OF PRETERM LABOR
| PHARMACOLOGIC AGENT | MECHANISM OF ACTION |
| Beta-adrenergic agonists | Adenylate cyclase inhibitor—sequesters intracellular calcium (e.g., terbutaline, ritodrine) |
| Magnesium sulfate | Uncertain—magnesium suppresses muscle contraction of myometrial strips in vitro, decreases intracellular calcium, and affects acetylcholine release |
| Prostaglandin synthase inhibitors (indomethacin) | Inhibition of the cyclooxygenase enzyme responsible for prostaglandins that promote uterine contractions |
| Calcium antagonists (nifedipine) | Inhibition of influx of calcium through the cell membrane |
TABLE 3-2
ADVERSE EFFECTS OF TOCOLYTIC AGENTS ON THE FETUS AND NEONATE
| PHARMACOLOGIC AGENT | ADVERSE EFFECTS |
| Beta-adrenergic agonists | Fetal tachycardia, neonatal hypoglycemia, hypocalcemia, and hypotension |
| Magnesium | Fetal demineralization with prolonged use, neonatal respiratory and motor depression at higher serum levels, ileus |
| Prostaglandin synthase inhibitors | Constriction of fetal ductus arteriosus leading to pulmonary hypertension, oligohydramnios, decreased fetal urine production, and spontaneous intestinal perforation |
| Calcium antagonists | No known human effects—decreases fetal arterial PO2 and pH in animal studies |
There is no question that tocolysis is effective over short-term intervals; however, clinical trials have not consistently demonstrated that gestation can be prolonged significantly or that respiratory distress syndrome can be consistently prevented with tocolysis. ∗
 Preterm labor: PROM accounts for 25% to 50% of preterm deliveries.
Preterm labor: PROM accounts for 25% to 50% of preterm deliveries.
 Maternal and neonatal infections
Maternal and neonatal infections
 KEY POINTS: PREMATURE RUPTURE OF MEMBRANES
KEY POINTS: PREMATURE RUPTURE OF MEMBRANES
1. The factors that lead to premature rupture of membranes may also provoke increased production of cytokines in both the fetus and the mother.
2. Cytokines appear to adversely affect neonatal outcome and to predispose the neonate to both neurologic and pulmonary problems, especially after a preterm birth.


27. A patient makes inquiries regarding multiple courses of steroids to enhance fetal lung maturity. What should you tell her about this approach?
Multiple courses of antenatal steroids (more than three) are associated with suppression of the fetal adrenal gland and decreased response to stress in a critically ill neonate. In addition, animal and human data suggest less brain growth and developmental delay in childhood after multiple doses of steroids. The benefit of more than one course of antenatal steroids is controversial. A National Institutes of Health consensus conference on antenatal steroids recommended that only a single course of steroids be used and that the use of subsequent courses be limited to patients in research studies that address this question. Several clinical trials tested weekly repeated courses of steroids versus a single course. A Cochrane review concluded that repeated courses may result in a modest reduction in neonatal respiratory distress syndrome. Still, more than three courses can result in other problems, as noted previously. A reasonable compromise is the use of a “rescue course” of steroids—that is, a single repeat course targeted at those most likely to deliver within a week. ∗†
28. During a review of the perinatal outcomes for premature infants at your hospital, the nurse manager for the intensive care nursery inquires whether there is an effective method to detect women at risk for premature delivery before they present in active preterm labor. What do current data indicate?
Many strategies have been used to identify patients who are destined to deliver prematurely. Risk assessment scoring using the modified Creasy score ( Table 3-3) or other similar systems works well in some populations but not in others. The Creasy score looks at a series of variables in an attempt to define clinical indicators that are likely to result in preterm labor. A major limitation of most clinical risk scoring systems is that they rely heavily on a history of preterm birth in a prior pregnancy, yet the majority of preterm births occur in women without such a history.
TABLE 3-3
RISK FACTORS IN THE PREDICTION OF SPONTANEOUS PRETERM LABOR (MODIFIED CREASY SCORE)
| MAJOR RISK FACTORS | MINOR RISK FACTORS |
| Multiple gestation | Febrile illness |
| DES exposure | Bleeding after 12 weeks’ gestation |
| Hydramnios | History of pyelonephritis |
| Uterine anomaly | Cigarette smoking >10 cigarettes/day |
| Cervix dilated >1 cm at 32 weeks’ gestation | One second-trimester abortion |
| ≥ Two second-trimester abortions | More than two first-trimester abortions |
| Previous preterm delivery | |
| Previous preterm labor, term delivery | |
| Abdominal surgery during pregnancy | |
| History of cone biopsy | |
| Cervical shortening <1 cm at 32 weeks’ gestation | |
| Uterine irritability | |
| Cocaine abuse |
Fetal fibronectin screening can identify a subgroup of women at high risk for preterm birth, but there is no known therapy that will consistently prevent preterm delivery in women with positive fibronectin screening. ∗
Since 2003, there have been over a dozen trials evaluating prophylactic use of progesterone agents, either vaginal or oral micronized progesterone or intramuscular 17-hydroxyprogesterone caproate (17Pc). In women with prior preterm birth, weekly 17Pc reduced the recurrence of preterm birth by 33% to 45% and vaginal micronized progesterone showed similar benefit in one large trial but not another. In women with short cervix detected by endovaginal ultrasound screening, vaginal micronized progesterone reduced early preterm delivery by 40% to 50% in two large trials. The ACOG has endorsed progesterone therapy in such patients. Several trials showed that these agents are not effective in twin or triplet pregnancies. ∗†‡§¶
30. What are some of the increased risks of twin pregnancies?









31. Why are monozygotic twins considered to be at higher risk for complications than dizygotic twins?
 Thoracopagus: joined at the thorax
Thoracopagus: joined at the thorax
 Xiphopagus: joined at the anterior abdominal wall (from the xiphoid to the umbilicus)
Xiphopagus: joined at the anterior abdominal wall (from the xiphoid to the umbilicus)
 Pygopagus: joined at the buttocks or rump
Pygopagus: joined at the buttocks or rump


 KEY POINTS: TWIN PREGNANCIES AND MULTIPLE BIRTHS
KEY POINTS: TWIN PREGNANCIES AND MULTIPLE BIRTHS
1. Multiple births are associated with an increased risk of problems during pregnancy.
2. The higher the number of fetuses, the greater the risk.
3. Preterm labor, twin-twin transfusion, developmental abnormalities, discordant growth, congenital malformations, fetal crowding syndrome, and several other abnormalities are all more common.
4. Monozygotic twins appear to be at greater risk than fraternal twins.
 Arterial cord pH sample below 7.0
Arterial cord pH sample below 7.0
 Apgar scores of 4 or less for at least 5 minutes
Apgar scores of 4 or less for at least 5 minutes
 Evidence of altered neurologic status (e.g., obtundation, seizures, altered level of consciousness)
Evidence of altered neurologic status (e.g., obtundation, seizures, altered level of consciousness)

34. Why has the term nonreassuring fetal status been used to replace the term fetal distress in practice?
In labor electronic FHR monitoring is the primary modality used to determine fetal oxygenation. Although this method is quite reliable when results are normal, when marked abnormalities occur on the FHR tracing the infant is more often vigorous and not acidotic at birth. Thus the term fetal distress is more often than not inaccurate. A more accurate expression is that the FHR is no longer reassuring and that either other information must be used to establish fetal well-being or, failing that option, the fetus must be delivered (Fig. 3-1).
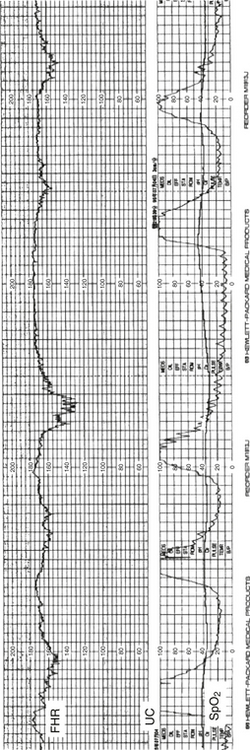
Figure 3-1 A fetal heart rate strip showing late decelerations of the heart rate following intrauterine contractions.
 KEY POINTS: PERINATAL ASPHYXIA
KEY POINTS: PERINATAL ASPHYXIA
1. The term perinatal asphyxia applies to relatively few pregnancies, yet it commonly makes its way into medical records with some degree of regularity.
2. Delineation of the physiologic abnormalities seen in the fetus and neonate should be used instead of the term perinatal asphyxia, which appears to be an exceedingly uncommon event as defined by the ACOG-AAP criteria.






A CST was one of the earliest techniques to assess fetal well-being. In this test uterine contractions are induced, either by maternal nipple stimulation or by an intravenous infusion of oxytocin (oxytocin challenge test [OCT]). The former method may be quicker and removes the need to establish an intravenous infusion; the latter is the traditional, time-honored technique. Results are interpreted the same, regardless of the method of inducing contractions. The mother is monitored with a tocodynamometer and a FHR transducer while uterine contractions are stimulated until adequate, which is defined as three contractions within 10 minutes. In a negative test result, there are no late decelerations of the FHR. In a positive test result, in which there are late decelerations, the risk of mortality and morbidity for the fetus increases, with some reports of mortality as high as 15%. There are, however, many false-positive instances of CST results. In such situations the obstetrician often faces a difficult decision of how aggressively to proceed with delivery of the fetus because the cervix may not be in a favorable condition at that time, and a cesarean section may be required. If the test results are equivocal, it may be reasonable to wait an additional 24 hours to repeat the test.





Neonatal depression is not always caused by hypoxia and acidosis. Furthermore, given the litigious environment surrounding the issue of perinatal brain damage, the issue of documenting the fetal blood gas status at birth is critical to an objective assessment of the baby’s condition. The following are indications for assessing blood gas status at birth:
 Operative intervention for nonreassuring fetal status
Operative intervention for nonreassuring fetal status


 Fetuses that had nonreassuring fetal status but did not have operative intervention
Fetuses that had nonreassuring fetal status but did not have operative intervention


 KEY POINTS: FETAL EVALUATION
KEY POINTS: FETAL EVALUATION
1. The goal of all pregnancies is the preservation of maternal well-being while delivering a healthy neonate.
2. To this end, assessment of the fetus is one of the most important aspects of care during pregnancy.
3. Although techniques for fetal evaluation have greatly contributed to improved outcomes, no technique is infallible and each should be considered only as a single additional piece of information.
4. Reliance on any single test is potentially hazardous to both mother and fetus.
 Anticonvulsants: Infants of mothers using anticonvulsants have twice the risk of malformations compared with the general population, especially cleft lip and palate and congenital cardiac defects. Valproic acid may cause neural tube defects, and diphenylhydantoin is associated with fetal hydantoin syndrome (i.e., microcephaly, developmental delay, growth failure, mental retardation, dysmorphic facies, and nail hypoplasia). Carbamazepine may also produce dysmorphism.
Anticonvulsants: Infants of mothers using anticonvulsants have twice the risk of malformations compared with the general population, especially cleft lip and palate and congenital cardiac defects. Valproic acid may cause neural tube defects, and diphenylhydantoin is associated with fetal hydantoin syndrome (i.e., microcephaly, developmental delay, growth failure, mental retardation, dysmorphic facies, and nail hypoplasia). Carbamazepine may also produce dysmorphism.














 KEY POINTS: MATERNAL DRUGS AND MEDICATIONS DURING PREGNANCY
KEY POINTS: MATERNAL DRUGS AND MEDICATIONS DURING PREGNANCY∗National Institutes of Child Health and Human Development National Registry for Amniocentesis Study Group. Amniocentesis for prenatal diagnosis: safety and accuracy. JAMA 1976;236:1471–1476.
∗Canadian Early and Mid-trimester Amniocentesis Trial (CEMAT) Group. Randomised trial to assess safety and fetal outcome of early and mid-trimester amniocentesis. Lancet 1998;351:242–247.
∗Eddleman KA, Malone FD, Sullivan L, et al. Pregnancy loss rates after midtrimester amniocentesis. Obstet Gynecol 2006;108:1067–72.
†Towner D, Currier RJ, Lorey FW, et al. Miscarriage risk from amniocentesis performed for abnormal maternal serum screening. Am J Obstet Gynecol 2007 Jun;196(6):608.e1–5
†Tabor A, Vestergaard CH, Lidegaard ø. Fetal loss rate after chorionic villus sampling and amniocentesis: an 11-year national registry study. Ultrasound Obstet Gynecol 2009 Jul;34(1):19–24.
∗Sundberg K, Bang J, Smidt-Jensen S, et al. Randomised study of risk of fetal loss related to early amniocentesis versus chorionic villus sampling. Lancet 1997;350:697–703.
†Goldenberg RL, Andrews WW, Guerrant RL, et al. The preterm prediction study: cervical lactoferrin concentration, other markers of lower genital tract infection, and preterm birth. National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network. Am J Obstet Gynecol 2000;182:631–635.
†Goldenberg RL, Andrews WW, Mercer BM, et al. The preterm prediction study: granulocyte colony-stimulating factor and spontaneous preterm birth. National Institute of Child Health and Human Development Maternal-Fetal Units Network. Am J Obstet Gynecol 2000;182:625–630.
§Goldenberg RL, Iams JD, Das A, et al. The preterm prediction study: sequential cervical length and fetal fibronectin testing for the prediction of spontaneous preterm birth. National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network. Am J Obstet Gynecol 2000;182:636–643.
¶Iams JD, Goldenberg RL, Mercer BM, et al. National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network. The preterm prediction study: can low-risk women destined for spontaneous preterm birth be identified? Am J Obstet Gynecol 2001;184:652–5.

∗∗Palomaki GE, Kloza EM, Lambert-Messerlian GM, et al. DNA sequencing of maternal plasma to detect Down syndrome: an international clinical validation study. Genet Med 2011;13:913–20.
††Norton ME, Brar H, Weiss J, et al. Non-Invasive Chromosomal Evaluation (NICE) Study: results of a multicenter prospective cohort study for detection of fetal trisomy 21 and trisomy 18. Am J Obstet Gynecol 2012;207:137.e1–8.
∗Konje JC, Walley RJ. Bleeding in late pregnancy. In: James DK, Steer PJ, Weiner CP, Gonik B, editors. High risk pregnancy: management options. Philadelphia: Saunders; 1994. p. 119–136.
∗Rao KP, Belogolovkin V, Yankowitz J, et al. Abnormal placentation: evidence-based diagnosis and management of placenta previa, placenta accreta, and vasa previa. Obstet Gynecol Surv 2012 Aug;67(8):503–19.
∗Ananth CV, Berkowitz GS, Savitz DA, et al. Placental abruption and adverse perinatal outcome. JAMA 1999;17:1646–1651.
†Han CS, Schatz F, Lockwood CJ. Abruption-associated prematurity. Clin Perinatol 2011 Sep;38(3):407–21.
∗Kim YA, Makar RS. Detection of fetomaternal hemorrhage. Am J Hematol 2012;87:417–23.
∗Verani JR, McGee L, Schrag SJ. Division of Bacterial Diseases, National Center for Immunization and Respiratory Diseases, Centers for Disease Control and Prevention (CDC). Prevention of perinatal group B streptococcal disease—revised guidelines from CDC, 2010. MMWR Recomm Rep 2010 Nov 19;59(RR-10):1–36.
†Byington CL, Polin RA. Policy statement—recommendations for the prevention of perinatal group B streptococcal (GBS) disease. Committee on Infectious Diseases; Committee on Fetus and Newborn. Pediatrics 2011;128:611–6.
†Randis TM, Polin RA. Early-onset group B Streptococcal sepsis: new recommendations from the Centres for Disease Control and Prevention. Arch Dis Child Fetal Neonatal Ed 2012;97:F291–4.
∗McParland PC. Obstetric management of moderate and late preterm labour. Semin Fetal Neonatal Med 2012;17:138–42.
∗Joffe GM, Jacques D, Bernis-Heys R, et al. Impact of the fetal fibronectin assay on admissions for preterm labor. Am J Obstet Gynecol 1999;180:581–586.
†Goldenberg RL, Iams JD, Das A, et al. The preterm prediction study: sequential cervical length and fetal fibronectin testing for the prediction of spontaneous preterm birth. National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network. Am J Obstet Gynecol 2000;182:636–643.
∗Sanchez-Ramos L, Delke I, Zamora J, et al. Fetal fibronectin as a short-term predictor of preterm birth in symptomatic patients: a meta-analysis. Obstet Gynecol 2009;114:631–40.
∗Conde-Agudelo A, Romero R. Antenatal magnesium sulfate for the prevention of cerebral palsy in preterm infants less than 34 weeks’ gestation: a systematic review and metaanalysis. Am J Obstet Gynecol 2009;200:595–609.
∗Abramovici A, Cantu J, Jenkins SM. Tocolytic therapy for acute preterm labor. Obstet Gynecol Clin North Am 2012;39:77–87.
∗NIH Consensus Statement: Effect of Cortiocosteroids for Fetal Maturation on Perinatal Outcomes. NIH Consensus Statement, volume 12. February 28–March 2, 1994.
†Garite TJ, Kurtzman J, Maurel K, et al. Obstetrix Collaborative Research Network. Impact of a ‘rescue course’ of antenatal corticosteroids: a multicenter randomized placebo-controlled trial. Am J Obstet Gynecol 2009;200:248.e1–9. Erratum in: Am J Obstet Gynecol 2009;201:428.
¶Iams JD, Goldenberg RL, Mercer BM, et al. National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network. The preterm prediction study: can low-risk women destined for spontaneous preterm birth be identified? Am J Obstet Gynecol 2001 Mar;184:652–5.
∗Meis PJ, Klebanoff M, Thom E, et al. National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network. Prevention of recurrent preterm delivery by 17 alpha-hydroxyprogesterone caproate. N Engl J Med 2003;12;348:2379–85. Erratum in: N Engl J Med 2003;25;349:1299.
†da Fonseca EB, Bittar RE, Carvalho MH, et al. Prophylactic administration of progesterone by vaginal suppository to reduce the incidence of spontaneous preterm birth in women at increased risk: a randomized placebo-controlled double-blind study. Am J Obstet Gynecol 2003 Feb;188(2):419–24.
†da Fonseca EB, Celik E, Parra M, et al. Fetal Medicine Foundation Second Trimester Screening Group. Progesterone and the risk of preterm birth among women with a short cervix. N Engl J Med 2007;2;357:462–9.
§Hassan SS, Romero R, Vidyadhari D, et al. PREGNANT Trial. Vaginal progesterone reduces the rate of preterm birth in women with a sonographic short cervix: a multicenter, randomized, double-blind, placebo-controlled trial. Am J Obstet Gynecol 2011;204:221.e1–8.
¶Combs CA, Garite T, Maurel K, et al. Obstetrix Collaborative Research Network. 17-hydroxyprogesterone caproate for twin pregnancy: a double-blind, randomized clinical trial. Am J Obstet Gynecol 2011;204:221.e1–8.


