Chapter 102 Interrelationships between Renal and Neurologic Diseases and Therapies
Renal Diseases Secondarily Affecting the Nervous System
Acute Renal Failure
Acute renal failure is a common problem occurring in as many as 4 percent of all hospital admittances in the United States, or nearly 20 percent of those requiring critical care management [Schrier et al., 2004]. The two most important potential morbidities of acute renal failure are neurologic and renal. Neurologic decompensation in association with acute intrinsic renal failure occurs with:
Neurologic abnormalities secondary to acute renal failure may occur in patients who have normal blood urea nitrogen and creatinine levels. The likelihood, severity, and nature of the neurologic decompensation resulting from acute renal failure are functions of the rate and severity of uremia and oliguria, metabolic balance of the whole organism, and intake (alimentary or parenteral) of free water, salt, and protein [Brouns and De Deyn, 2004].
Water Intoxication, Hyponatremia, and Brain Edema
Signs and symptoms of water intoxication may include headache, nystagmus, nausea, vomiting, diaphoresis, weakness, generalized tremulousness, ankle clonus, and the development of muscular irritability with coarse fibrillary twitching. Mental status changes range from apathy to progressive anxious restlessness, through agitation, confusion, or forgetfulness, to obtundation [Bhananker et al., 2004; Riggs, 2002]. It is possible that underlying predilections to migraine, anxiety, or other neurologic conditions may influence the symptomatic expression of water intoxication. The rate of deterioration in neurologic function ranges from gradual to rapid; the course ranges from linear to stepwise, and the severity ranges from mild to severe.
Children are at particularly high risk for the development of sudden decompensation due to brain edema at higher serum sodium concentrations than adults because they usually have higher brain:skull ratios. The immature brain often reaches adult size by 6 years of age, whereas adult skull size may not be achieved until 16 years of age [Moritz and Ayus, 2002]. Because of this vulnerability, the outcome of children whose water intoxication is overlooked may be worse than that for adults with similar duration and degree of excessive free water retention. Systemic aspects of water intoxication include cardiovascular compromise or pulmonary edema. These complications further jeopardize brain function owing to impaired oxygenation, provision of glucose, and removal of toxic metabolites of brain metabolism. Hyponatremia may result in seizures, increasing cerebral energy demand and the rate at which toxic byproducts of metabolism accumulate. Brain edema may develop and increase intracranial pressure, further impairing cerebral circulation. The edema is due to osmotically mediated flow across the blood–brain barrier (BBB), diluting extracellular electrolytes and then intracellular electrolytes.
If hyponatremia associated with neurologic decompensation remains uncorrected, convulsions, coma, and death due to brain herniation or complications of generalized convulsions may follow in quick succession. Under experimental conditions, the increase in brain water required to produce neurologic symptoms is about 3 percent, with an associated decrease in concentration of intracellular cations estimated to be 20 percent [Dodge et al., 1960].
Cerebral edema per se is unlikely to be the cause of many of the early neurologic signs and symptoms of water intoxication because these symptoms can be produced under experimental conditions without cerebral edema, and because cerebral edema in isolation does not necessarily produce a similar constellation of signs and symptoms. Exquisitely focal enhancement of neuronal excitability accompanies elevation (within certain bounds) of extracellular potassium ([K+]o ) and reduction of extracellular hydrogen ion ([H+]o). This state of ionic enhancement of highly regulated excitability is associated with similarly highly regulated changes in brain interstitial extracellular osmolarity. Reduction of osmolarity enhances neuronal excitability and synaptic transmission, while increases in osmolarity decrease excitability and synaptic transmission [Rosen and Andrew, 1990; Somjen, 1998]. Maintenance of low (isosmotic) cerebral interstitial sodium ([Na+]o) concentration enhances synaptic transmission via the voltage-dependant inward calcium ion (Ca2+) currents of presynaptic neurons. The integrity of the system is maintained by the fact that, as certain critical elevations of [K+]o are achieved, counter-regulatory partial inactivation of presynaptic currents produces a fall in [Na+]o and interstitial calcium ([Ca2+]o). Regulatory events occur that inhibit excessive excitation and prevent energy failure, excessive accumulation of toxic byproducts, and maldistribution of ions [Somjen, 2002]. This is a subject of considerable complexity, the discussion of which exceeds the confines of this chapter. Among other complexities is the probability that the characteristics of these ionic gradients may vary in various brain regions, a subject about which a considerable amount remains to be discovered. Much of what is currently understood is limited to the hippocampus. However, the general principles of the maintenance of brain to plasma ratios are likely to be fairly uniform across brain regions. The importance of these gradients to the proper function of the central nervous system (CNS) is represented by the considerable energy that is expended in order to maintain the actions of adenosine triphosphatase pumps, selective ion channels, and aquapores at the BBB to maintain different ionic concentrations in the brain interstitial fluids and cerebrospinal fluid (CSF) from those found in plasma [Schielke and Betz, 1992; Somjen, 2002]. This extraordinary energy demand is exemplified by the high density of mitochondrial brain capillary endothelia, required to maintain active transport to and from the cerebral interstitial compartment [Oldendorf et al., 1977]. In addition to other expenditures, a considerable amount of energy is devoted to the maintenance of a lower resting cerebral interstitial potassium concentration ([K+]o) than elsewhere in the body; the ion/solute brain barrier also maintains lower resting-state [HCO3−]o and calcium [Ca2+]o, but higher [Na+]o, magnesium [Mg2+]o, chloride [Cl−]o, and, as already noted, [H+]o than is found in plasma [Somjen, 2002].
The mechanisms and effects of disturbances in ionic gradients and solute concentrations within particular compartments can readily be seen to differ on the basis of the nature of perturbation. While shifts of ions and water in relationship to the osmolarity of adjacent compartments are normal within the context of cerebral autoregulation, deleterious examples are to be found in many disease states. Thus, given the extraordinary amount of energy expenditure required to maintain steady state and the minute compensations that occur in particular regions of brain, it can be seen that hypoxic-ischemic injury, with exhaustion of energy reserves and accumulation of a variety of ions, metabolic byproducts, and excitotoxic intermediates, produces one pattern of dysfunction. On the other hand, primarily osmotic provocations to maldistribution of ions and solute across the various compartments can be seen to produce a very different pattern of disturbance (the pattern seen in cerebral water intoxication or other sources of cerebral edema), so long as sources of energy continue to be supplied to brain. Excessive changes in plasma osmolarity may generate anisosmotic forces that overwhelm the compensations imposed by the BBB and disturb cerebral interstitial osmolarity and osmolality. BBB permeability for water is greater than that for ions. Water intoxication represents an acute form of hyposmolar plasma, which produces one pattern of cerebral compartmental ionic shifts that, at some point (when the capacity for renal compensation is exceeded), is the result of the entry of excessive water into the interstitial spaces of brain. The appearance on magnetic resonance imaging (MRI) in this situation shows cortical sulcal narrowing, T2 hyperintensity, restricted diffusion, and diffuse pial enhancement, changes characteristic for water intoxication [Yalcin-Cakmakli et al., 2010].
It has been demonstrated recently that the amount of glial plasma membrane expression of the water transport protein, aquaporin-4 (AQP4), correlates with the degree of vulnerability for water intoxication-associated brain swelling [Yang et al., 2008]. Interestingly, underexpression of astroglial AQP4 provides protection from brain swelling associated, under experimental conditions, not only with water intoxication, but also with focal cerebral ischemia and bacterial meningitis. On the other hand, underexpression renders experimental animals more vulnerable to brain injury from the vasogenic edema associated with brain tumor, brain abscess, hydrocephalus, or cortical freeze-injury. AQP4 plays additional roles, including exerting an influence on the rate of astrocyte migration during brain development, and in the fostering of glial scar formation, as well as enhancing sound- or light-evoked potentials and in modifying threshold and duration of experimentally induced seizures [Verkman et al., 2006]. The role that AQP4 may play, beyond that of water transport in neurological dysfunction associated with water intoxication, remains to be defined. It has been demonstrated that there is regional variation in AQP4 expression and function, with the perivascular, rather than endothelial, AQP4 being responsible for development of cerebral water intoxication [Amiry-Moquaddam et al., 2004]. There is experimental evidence that seizures may enhance cerebral water intoxication, and that this effect may be greater in female than male rats.
Cerebral dysfunction in the various types of ion/solute perturbations may involve depression of function (e.g., spreading cortical depression may be an example of this sort); or, in other situations, it may be associated with enhanced abnormal cerebral activities, such as seizures. These functional variations depend on the relative differences across various membranes, in the combination of sodium concentration and osmolarity within those locations, differences that alter, in concentration-dependent ways, voltage-dependent presynaptic calcium and potassium currents, characteristically enhancing one and depressing the other. In the case of water intoxication, cerebral calcium currents are increased as a consequence of dilution of the sodium concentration ([Na+]o) as the presynaptic extracellular milieu is lowered, an effect that occurs while compartmental osmolarity does not significantly change [Chebabo et al., 1995]. This effect correlates with spreading hippocampal depression. A salt-depleted extracellular cerebral interstitial state, with the development of hyposmolarity rather then isosmolarity, may result in enhanced synaptic excitability rather than cortical depression, due to lowering of extracellular chloride ([Cl–]o], since this produces a situation where there is failure of chloride-mediated function of glycine and gamma-aminobutyric acid (GABA)-mediated inhibitory synapses [Kaila, 1994; Huang and Somjen, 1997a, b; Somjen, 1998; Rosen and Andrew, 1990]. These pathophysiological observations indicate that the neurological findings of water intoxication or other particular forms of ion and solute disturbance manifest differences that are not merely the result of one element. Acute and chronic forms of water intoxication differ to some extent in manifestations. This is because the rate of introduction of water into cellular systems may result in nonlinear effects on osmolality and the concentrations of various solutes within various cellular compartments. Some of this variation is the result of adjustments to the function of barriers and membrane channels that are governed by hormonal influences.
The nature of the hyponatremic state having thus been parsed, the conditions that may produce hyponatremia, as well as hypernatremia (Table 102-1), may be addressed, with appropriate tests or recognition of the role that a chronic or acutely presenting condition might have exerted. Maintenance of circulation, in some instances, requires acute judicious administration of fluid, in which case isotonic sodium usually is permissible, pending further work-up. Volume expansion with hypotonic saline in a hyponatremic patient poses risks if the patient is actually sodium-depleted systemically. The decision to restrict fluids is appropriate if there is evidence for SIADH, a diagnostic theory that ought to be resisted if the patient has depleted intravascular volume. There are situations where hypertonic saline should be considered. Dialysis may be necessary in some patients [Bhananker et al., 2004; Riggs, 2002]. The rate of sodium correction is a particularly important consideration. Excessively rapid correction poses the danger of development of central pontine myelinolysis. In children, it is recommended that correction at the rate of approximately 1 mEq/L/hour be achieved, until the patient becomes alert and seizure-free, plasma sodium becomes 125–130 mEq/L, or serum sodium level is increased by 20–25 mEq/L, whichever occurs first. If seizures persist, or if there are signs of increased intracranial pressure (especially if these signs are worsening), the sodium concentration may be corrected at a rate of 4–8 mEq/L for 1 hour (if tolerated), or until seizures stop. Assuming that total body water comprises 50 percent of body mass, administration of 1 mL/kg of 3 percent NaCl solution will increase plasma sodium by approximately 1 mEq/L [Moritz and Ayus, 2002].
| Mechanism | Source | Causative Factor/Disorder |
|---|---|---|
| CAUSES OF HYPONATREMIA | ||
| Excessive NaCl loss | Gastrointestinal tract Skin Urinary tract |
Diarrhea
Cystic fibrosis |
| Excessive water intake | Oral
Parenteral Rectal |
Psychogenic Acute renal failure Therapeutic error Coma Tap water enema |
| Defective water excretion | Inappropriate antidiuretic hormone secretion | Anesthetic drugs Craniocerebral trauma Infection |
| CAUSES OF HYPERNATREMIA | ||
| Excess sodium intake | Improperly mixed formula or rehydration solution Excessive sodium bicarbonate administration during resuscitation Saltwater drowning |
|
| Water deficit | Diabetes insipidus Diabetes mellitus Excessive sweating Increased water loss Adipsia Inadequate water intake |
|
| Water deficit in excess of sodium deficit | Diarrhea Osmotic diuretics Obstructive uropathy Renal dysplasia |
|
Hyperkalemia
During the first 48 hours of anuric acute renal failure from prerenal causes there is loss of as much as 70–80 percent of renal outer medullary potassium secretory channels and 35–40 percent of the activity of potassium channel inducing factor. Cardiac and pulmonary manifestations of hyperkalemia generally precede and are greater threats for survival than neurologic ones. Cardiac dysfunction is usually the earliest and most ominous clinical sign of hyperkalemia. However, rare instances of hyperkalemia of acute renal failure presenting as a neurologic sign (e.g., striated muscle paralysis) rather than as cardiac decompensation have been described [Cumberbatch and Hampton, 1999].
Within the BBB, elevation of extracellular potassium ([K+]o) depolarizes neuronal membranes in a nonlinear fashion. As the elevation of [K+]o increases, countervailing increases in inward sodium currents attenuate the extent to which depolarization results, probably preventing wide fluctuations in the functional milieu of excitable cells and membranes. Significant [K+]o elevation, or, for that matter, diminution, may have drastic functional consequences within the CNS. In the case of elevation of interstitial potassium ion concentrations to levels ranging from the usual 3–3.5 mM to 5–6.25 mM, enhanced excitability and synaptic transmission is the dominant effect in neural tissues, such as hippocampal slices. On the other hand, concentrations of >8 mM begin variously to cause depression of excitability and conductance, and at certain concentrations to induce spontaneous epileptiform discharges. Elevation of serum potassium concentration reflects a complex set of equilibria. Factors include the degree of displacement of potassium from the intracellular compartment, as the result of acidemia and the state of dilution or concentration of body fluids (the balance of free water intake and output). Hyperkalemia may provoke smooth or striated muscle weakness, owing to lowered membrane resting depolarization potentials, delayed depolarization, rapid repolarization, or slowed cardiac and peripheral nerve conduction velocities [Chantler, 1988]. Correction of metabolic acidosis, with infusion of calcium or glucose, insulin, and, in some instances, administration of a β2-adrenergic receptor stimulant such as salbutamol, may shift the circulating potassium excess to safer intracellular loci [Kemper et al., 1996]. Management may involve the use of ion exchange resins or dialysis.
Particularly important causes of acute hyperkalemia involve muscular trauma, rhabdomyolysis from trauma or burns, and succinylcholine administration to susceptible individuals in the setting of acute muscle damage. Catecholamine elevation in the setting of hypothermia may produce hyperkalemia due to changes in the intracellular/extracellular distribution of potassium. A list of causes of hyperkalemia is found in Table 102-2.
| Mechanism | Causative Factor/Disorder |
|---|---|
| HYPOKALEMIA | |
| Deficient intake | Protein-calorie malnutrition Parenteral nutrition |
| Renal loss | Distal tubular acidosis |
| Renal disease | Proximal tubular acidosis (Fanconi’s syndrome) Bartter’s syndrome Interstitial nephritis Pyelonephritis |
| Extrarenal disease | Diabetes mellitus Cushing’s syndrome Aldosteronism Drug administration (diuretic, aspirin, steroids) Hypomagnesemia Hypercalcemia |
| Shift (extracellular to intracellular) | Alkalosis Drugs (insulin, catecholamines) Parenteral nutrition |
| Extrarenal loss | Vomiting, diarrhea Fistula drainage Laxative abuse Ion-exchange resins Congenital alkalosis |
| HYPERKALEMIA | |
| Excessive intake | Potassium-containing salt substitutes Parenteral administration (excessive infusion, outdated blood) Gastrointestinal bleeding |
| DECREASED RENAL EXCRETION | |
| Renal disease | Oliguric renal failure Chronic hydronephrosis Potassium-sparing diuretics |
| Extrarenal causes | Addison’s disease Congenital adrenal hyperplasia Diabetes mellitus Drugs (beta blockers, heparin) |
| Shift (intracellular to extracellular) | Rapid cell breakdown (trauma, infection, cytotoxic agents) Acidosis Freshwater drowning |
Hypokalemia
Hypokalemia is often encountered in the management of critically ill patients; some of the more common causes of hypokalemia are summarized in Table 102-2. One of the more frequently encountered situations involves the partitioning of potassium between the extracellular and intracellular spaces, which is affected by glucose and insulin metabolism, the renin-angiotensin-aldosterone system, and circulating catecholamines. Hypokalemia occurs in the setting of several different forms of renal tubular acidemia. Management of potassium is a particularly important aspect of the treatment of individuals with diabetic ketoacidosis. Clinical manifestations of hypokalemia, as is true of hyperkalemia, tend to involve smooth or striated muscle. The effects of potassium on the electrocardiogram (EKG) provide a valuable and acutely available adjunct to other tests intended to disclose potassium status. Among the neuromuscular conditions of importance is hypokalemic periodic paralysis, which is reviewed in Chapter 96.
Uremic Encephalopathy
It occurs when glomerular filtration rate has declined to less than 10 percent of normal. It is fatal if untreated. Most patients with acute uremia have experienced proportional injury to tubular and glomerular systems. Bicarbonate wasting occurs but is, in part, compensated for by the retention of nonchloride anions, such as sulfate and phosphate. The result is high anion gap acidosis with normal or increased serum potassium concentration. Sodium and chloride levels remain normal, unless free water excretion is impaired. Brain edema is uncommon in uremic encephalopathy because most of the osmotically active molecules that accumulate in uremia are small molecules that equilibrate readily across the BBB [Smogorzewski, 2001]. The occurrence and degree of uremic encephalopathy correlate poorly with renal function, as measured by the degree of blood urea nitrogen abnormality. It does appear that several guanidino compounds that are subject to significant elevation in uremic patients (creatinine, guanidine, guanidino-succinic acid, and methylguanidine) are capable of causing abnormal neuronal hyperexcitability that triggers seizures in experimental models of uremia, and may also precipitate cognitive disturbances [DeDeyn et al., 2001].
Disturbances of endocrine function occur in uremia, with possible elevations, especially in chronic renal failure, of parathyroid hormone (PTH), insulin, growth hormone, glucagons, thyrotropin, prolactin, luteinizing hormone, or gastrin. Elevated concentrations of PTH, associated particularly with cases of uremic decompensation of chronic renal failure, may activate second-messenger systems that alter cellular calcium hemostasis, the balance of which is viewed by many observers as a central element of the metabolic crisis that produces uremic encephalopathy [D’Hooge et al., 2003; Fraser, 1992]. PTH concentration elevations have been clearly linked to the reduction of mental status and electroencephalographic (EEG) abnormalities associated with uremic encephalopathy [Fraser, 1992; Moe and Sprague, 1994]. In chronically uremic patients, EEG abnormalities and mental and psychiatric manifestations may improve with parathyroidectomy or chemical suppression of parathyroid function [Cogan et al., 1978]. The degree of EEG abnormalities observed in the uremic state has been directly correlated with PTH levels. In one careful experimental study, it was determined that a rise in calcium concentration in gray and white matter occurred in association with nephrectomy-induced uremia, but that the degree of brain hypercalcemia was greater if thyroparathyroidectomy had been performed than if those organs had been left intact. EEG monitoring showed that EEG findings were more persistently abnormal in the thyroparathyroidectomized dogs than in those whose glands remained intact. Thus, uremic hyperparathyroidism appears to be an important negative influence on cerebral function [Akmal et al., 1984]. Exogenous toxins, infectious and inflammatory disturbances, and particularities of glomerulotubular dysfunction may also play variable roles in exacerbating uremic encephalopathy, but are not essential predisposing features for that condition.
Numerous lines of evidence suggest the considerable importance of disturbances of calcium homeostasis, membrane excitability, and neurotransmitter function as central functional abnormalities of uremic encephalopathy [Moe and Sprague, 1994]. Although extraordinarily abundant in the body, divalent cationic calcium is highly protein-bound or sequestered within organelles, including endoplasmic reticulum and mitochondria. What remains of the intracellular ionized calcium pool is at concentrations of 50–100 nM, approximately four orders of magnitude lower than [Ca2+] [Somjen, 2002]. The considerable transmembrane driving force that this concentration difference could exert is prevented by a high degree of membrane impermeability to calcium, and a high degree of regulation of such calcium channels as are present. The fact that such protective mechanisms are present and that free cytosolic calcium concentrations – designated [Ca2+]i – are so low (much lower than that even of highly restricted free cytosolic Mg2+) pays tribute to the potency of the free calcium ion [Somjen, 2002]. It is important to note that there is an extraordinarily elegant functional interaction – in some instances, synergistic, and in others, antagonistic – of calcium with the other physiologically important divalent cation, magnesium. Attachment of extracellular ionic calcium ([Ca2+]o) and magnesium ([Mg2+]o) to negative ions on the outer surface of cell membranes has been shown to stabilize excitable membranes because a resulting increase in transmembrane voltage reduces the likelihood that voltage-gated ion channels will open [Hille, 2001]. Within the nervous system, calcium influx through voltage-gated calcium channels into presynaptic terminals is a requirement for the occurrence of synaptic transmission [Hille, 2001]. This current and the likelihood of resulting neurotransmitter release are negatively modulated by the presence of [Mg2+]o [Somjen, 2002].
Acute deficiency of magnesium or calcium is the cause of cramps and tetany, due to loss of their collaborative stabilizing effect on peripheral nerve and muscle. Box 102-1 lists some of the common causes of hypocalcemia and hypo- and hypermagnesemia. The lack of associated central effects has been explained by the protective latency in concentrations of these cations within the BBB. With greater degrees of loss of this modulating effect peripherally, failure of neuromuscular transmission develops [Somjen, 2002]. On the other hand, chronic renal failure (glomerular filtration rate <30 mL/min) is one of the most common causes of acquired hypocalcemia. First, failing kidneys may inadequately perform the second hydroxylation that is essential in activating 1,25-dihydroxyvitamin D. Second, reduced glomerular function permits hyperphosphatemia to develop. Third, diminished calcitriol production impairs intestinal absorption of calcium. Fourth, deposition of calcium and of phosphorus in soft tissues occurs. The role that hypocalcemia plays in uremic encephalopathy remains uncertain. The likelihood that hypocalcemia will produce neurological manifestations is greatest in infants, as has been demonstrated for hypocalcemic seizures [Lynch and Rust, 1994]. However, there are few data specifically concerning individuals in this age group that happen to experience uremia. Among the manifestations of uremia that might be related to hypocalcemia should be those manifestations already known to occur in association with hypocalcemia without associated uremia.

















Clinical symptoms that occur in uremia include seizures, encephalopathy, poor feeding, lethargy, tremulousness, abdominal distention, and gastrointestinal autonomic dysregulation. Twitching or muscular weakness (due to impeded acetylcholine release at the neuromuscular junction) or cramping (including laryngospasm), apnea, paraesthesiae, seizures, and tetany of larynx, hands, and limb also may occur. Psychiatric manifestations are important to consider in relation to uremia with hypocalcemia, since such manifestations are more common in children than adults and may include moodiness and depression. Among these various manifestations, those with particular likelihood to derive, at least in part, from uremic hypocalcemia are altered mental status, tremulousness, and the muscle cramps that occur early in the development of uremia. Hypocalcemic tetany is produced because neuronal excitability overdrives the muscular atony and may be found especially in children [Cooper and Gittoes, 2008]. The muscle fasciculations of more severe and persistent uremia could be related to hypocalcemia, as may the peculiar movement disorder termed “uremic twitching.” Uremic encephalopathy remains a complicated condition, the pathophysiology of which could be multifactorial, but hypocalcemia could play a role. At any rate, hypocalcemia deserves a place beside hyponatremia and hypomagnesemia as a mediator of uremic encephalopathy [DeDeyn et al., 1992].
The interaction between calcium and magnesium is a quite remarkable partnership when things go well, and each must be considered in situations where the other has been implicated as a cause of dysfunction. Either hypomagnesemia or hypermagnesemia may occur in the setting of chronic renal disease. The former may develop from renal magnesium wasting. Hypomagnesemia is a condition that may be quite serious. In critically ill patients, including those who manifest renal failure, development of hypomagnesemia is associated with a 2- to 3-fold increased risk of death [Rubeiz et al., 1993]. It tends to be particularly serious in infants and the elderly. The observation that hypomagnesemia may be found in as many as 47 percent of patients with hypokalemia, 27 percent of individuals with hyponatremia, and 22 percent of those with hypocalcemia [Whang et al., 1984] – disturbances common in chronic renal disease – underlines the importance of considering its role in the neurological deficits associated with uremia. The fact that, at cerebral synaptic surfaces, extracellular magnesium serves as an important inhibitor of synaptic neurotransmitter release and is an N-methyl-d-aspartate (NMDA) receptor antagonist, reducing calcium influx, also suggests the potential importance of hypomagnesemia in uremic encephalopathy. Its antagonist in that function is calcium, an agonist that enhances neurotransmitter release [Somjen, 2002]. Should hypomagnesemia play a role, the most likely contributions would be to neurological manifestations tied to hypomagnesemia in nonrenal patients, including encephalopathy and seizures [Nuytten et al., 1991; Nakamura et al., 1994]. Hypomagnesemia might play a role in the twitching and other muscular manifestations of uremia, manifestations with which it has been associated in association with hypocalcemia [Kingston et al., 1986].
Hypermagnesemia is even more interesting as a possible cause of neurological manifestations of uremia. It is a relatively uncommon condition specifically because normal renal regulation of magnesium is quite efficient, including a rapid adaptation that permits the tubular system almost entirely to eliminate reabsorption of magnesium that has entered the tubular filtrate. It is thus not surprising that hypermagnesemia is most likely to be encountered in individuals with renal failure, especially children with acute renal failure, but also in individuals of any age with end-stage renal disease (ESRD). The normal adult filtered magnesium load is more than 2 g each day. Under normal conditions, 97 percent of this load is reabsorbed and re-enters the systemic extracellular space. Two-thirds of this reabsorption takes place in the thick ascending loop of Henle, and the remainder in the proximal tubule, except for a small amount (approximately 5 percent) recovered in the distal nephron [Quamme, 1989]. Surprisingly little is known about the mechanisms for nonrenal cellular transport of magnesium [Musso, 2009]. The fact that excess magnesium may be very efficiently eliminated by the kidney protects the public at large from the rather shocking amounts of magnesium that are imbibed in the form of antacids, laxatives, cathartics, or enemas [Woodard et al., 1990].
Many individuals with ESRD have only mild hypermagnesemia, likely because magnesium is readily dialyzable [Navarro-Gonzalez et al., 2009]. The initial presentation of hypermagnesemia is usually during the oliguric onset of renal failure. During that phase of severe renal dysfunction, magnesium supplementation may greatly worsen the degree of hypermagnesemia, particularly in instances where there is associated uremic acidemia. However, serum magnesium levels return to normal during the diuretic phase. In individuals with ESRD, magnesium-containing antacids and cathartics may worsen the hypermagnesemia. Neurological manifestations in uremic patients to which hypermagnesemia might contribute include lethargy, moodiness, depression, paraesthesiae, striated and smooth muscle weakness, and neuropathic changes in cardiac conduction, autonomic cardiovascular regulatory abnormalities, disorders of smooth and striated muscle function, and autonomic aspects of gastrointestinal function. Conditions that might worsen uremic hypermagnesemia are hypothyroidism, Addison’s disease, familial hypercalciuric hypercalcemia, and milk alkali syndrome. As with other electrolyte disturbances, clinically significant hypomagnesemia is found more commonly in infants and elderly individuals, usually in association with renal failure.
It appears likely that some combination of effects produced by the presence of low-molecular-weight, fast-acting toxic solutes that are not excreted in renal failure may contribute to the neurological and other abnormalities of chronic renal failure. Among the dozens of unexcreted solutes that might produce such effects are urea, creatinine, hippuric acid, polyamines, polypeptides, guanidino compounds, acetoin, myoinositols, sulfates, aliphatic and aromatic amines, phenols, purines, indoles, glucuronates, spermine, dl-homocysteine, orotate, and glycine [Arieff et al., 1976; D’Hooge et al., 2003]. These compounds have different capacities for the penetration of nervous tissues and also may have effects on blood vessels, membranes, enzymes, neurotransmitters, or receptors. Many of these potentially toxic chemicals, so quietly and efficiently removed by the normal kidney, are less efficiently removed from circulation by dialysis.
It has long been known that cerebral rates of utilization of glucose, oxygen, and high-energy phosphate compounds fall in uremic encephalopathy, apparently because of reduced demand rather than energy failure. To some extent this may be a protective adaptation [Mahoney et al., 1984], although it is possible that the reduction is due in part to failure of synaptic transmission. In uremic dogs, brain high-energy phosphates and glucose were normal, indicating normal energy reserve, as was the brain energy charge, representing the proportion of the adenine nucleotide made up by high-energy phosphates. In this study, the redox state was also high; hence the oxygen supply to brain cells was not limited. It was concluded that, in uremia, changes in energy metabolism were related, not to energy supply, but rather to energy demand [Mahoney et al., 1984]. A positron emission tomography (PET) study of uremic humans also suggested decreased brain energy demand, although a dysregulated metabolic state could not be excluded [Kanai et al., 2001]. Interestingly, the degree of reduction of oxygen metabolism was greatest in frontal cortex, the brain region that has shown the greatest degree of atrophy in individuals that have been on long-term hemodialysis [Savazzi et al., 1995]. These were studies of adults rather than children. Separate risk factors for cortical atrophy with greater emphasis in frontal cortex in adults are chronic hypertension and arteriosclerosis [Linder et al., 1974], the former being a factor that could affect outcome of children and adolescents with uremic renal failure.
It is not as yet known whether these indications of global brain metabolic reduction mask regional or focal excesses of utilization (in conjunction, for example, with focal seizure activity or “twitch-myoclonus”), or whether some aspects of this reduction may injure rather than protect the brain. Observed reduction in activity of the pentose phosphate shunt, an important source of reducing equivalents for maintenance of myelin and other synthetic tasks, may represent compensatory reduction of a temporarily dispensable energy expenditure. On the other hand, reduced flux in this pathway interferes with the maintenance of myelin. Interestingly, the uremic reduction in overall cerebral metabolic rate is not accompanied by reduction in cerebral blood flow, suggesting an unusual and as yet unexplained form of energy supply–demand uncoupling. Disturbances of the efficiency with which energy metabolism is carried out, as well as a number of the other forms of dysfunction already considered in the central nervous system, could produce changes in the pH of the CNS and its various compartments which could affect neurologic function [Arieff et al., 1976].
Uremic synaptosomal preparations confirm diminished activity of the metabolic pumps associated with Na+/K+ and Ca2+ adenosine triphosphatases and disturbances, not only in calcium, but also in cellular magnesium and potassium homeostasis. Evidence suggests that creatinine and acidic derivatives of guanidine metabolism (e.g., methyl guanidine and guanidinosuccinic acid) inhibit physiologic responses to GABA and glycine, disturb synaptic transmission in the CA1 region of the hippocampus, and elevate the excitatory tone of certain neuronal populations. Guanidino compounds, phenol, and spermine, among the first uremic small molecules to have been proven to exert definable deleterious effects on brain, alter various membrane ionic conductances by means of voltage- or ligand-gated channels. These include the NMDA receptor complex, which variously enhances inward calcium or outward potassium currents [D’Hooge et al., 2003].
Sufficient concentrations of some of these various small-molecule compounds are capable of engendering clonic seizures under experimental conditions, and it is possible that they are responsible for such classic manifestations of uremic encephalopathy as uremic “twitch-myoclonus.” Uremic myoclonus has also been associated with elevation of CSF phosphate to concentrations in excess of 3.8 mg/mL, perhaps reflecting a particular sensitivity of the brainstem reticular formation to this chemical [Chadwick and French, 1979]. Hypercalcemia is a known cause of myoclonic encephalopathy with seizures and dysarthria. Hypophosphatemia may also contribute to development of seizures in some patients [Rivera-Vazquez et al., 1980]. Toxicity of guanidinosuccinic acid is more marked in the posthypoxic state [Torremans et al., 2004], owing to the generation of superoxides and hydroxyl free radicals that have been found to produce glial cell death under experimental conditions [Hiramatsu, 2003]. It is of interest that many of the small molecules associated with uremia may play important positive roles in normal brain, perhaps as free-radical scavengers. Factors that may account for toxicity of these same molecules during renal failure likely include loss of closely regulated and carefully compartmentalized concentrations and enhanced transformation of nontoxic and metabolically useful ones into toxic molecules.
An important example of this process is free-radical-stimulated transformation of arginosuccinic acid into guanidinosuccinic acid [Cohen, 2003]. The generation of that toxic intermediate is enhanced in proportion to urea concentration [Aoyagi, 2003]. The complex state of uremia includes other pertinent and, as yet, incompletely understood or characterized metabolic and neurotransmitter disturbances, including the possible rise of glycine concentration in critical locations and fall in GABA concentrations in others. Uremic disturbance of tryptophan metabolism results in accumulation of kynurenine neurotransmitters that may provoke seizures, alter consciousness, or produce neuronal injury or cell death [Topczewska-Bruns et al., 2002]. Older data concerning uremic depression of metabolism of nucleotides, catecholamines, and amino acids involved in neurotransmitter synthesis [Fraser et al., 1985] may remain pertinent. Uremia may disturb the transport of amino and organic acids that activate excitatory or inhibitory synapses [Biasioli et al., 1986; Deferrari et al., 1981]. Although recent data on this subject are not abundant, one useful summary of available evidence suggests that low plasma levels of tryptophan and elevations of sulfuro-amino acids and of branched chain amino acids, among other abnormalities, might play a role [Furst, 1989].
Pathologic studies of uremic encephalopathy suggest variable degrees of generalized neuronal degeneration. In some instances, perivascular necrosis and demyelinative changes are discerned. Abnormalities may be emphasized in cerebral cortex, subcortical and brainstem nuclei, or cerebellum. In persons dying of acute uremic encephalopathy, Alzheimer type II astrocytes may be found [Norenberg, 1994]. Subdural hemorrhages are found in less than 3 percent of cases of chronic renal failure with uremia [Fraser and Arieff, 1997].
Acute uremic encephalopathy produces deterioration of higher cortical function at a rate that varies from slowly progressive to fulminant. These changes persist and perhaps worsen in a chronic uremic state requiring hemodialysis. The earliest characteristic changes, often subtle or insidious, include inattention, indecisiveness, irritability, and diminished intellectual agility. These changes may be improperly ascribed to depression. They are often more apparent to caregivers than to the patient. They may be overlooked in children or may be falsely ascribed to uncooperativeness or irritability. Standardized assessment of vigilance with digit span or serial subtraction may be useful in following patients at risk. A peculiar dyspraxic hesitancy of speech is a common and distinctive clue, usually dyspraxia without dysnomia or other associated aphasia [Martinez et al., 1978].
Lethargy, somnolence, anorexia, nausea, vomiting, pruritus [Zucker et al., 2003], and disturbance of the sleep–wake cycle are other common early manifestations. Episodic confusion, disinterest in surroundings, poor ability to concentrate, or impairment of recent memory may develop, interspersed with more lucid intervals. Occasionally, especially in persons with fulminant renal failure, acute agitation, delirium, psychosis, coma, or catatonia suggests the presence of uremic encephalopathy [Souheaver et al., 1982]. Higher cortical function deficits may worsen as a consequence of duration of hemodialysis therapy [Kimmel et al., 1993]. In such instances, the effects of an intoxicating drug (e.g., corticosteroids, propranolol, cimetidine, levetiracetam, phenobarbital, or tricyclic antidepressants) must be excluded. Uremic encephalopathy may produce signs suggestive of Wernicke–Korsakoff syndrome [Jagadha et al., 1987].
The development of tremor is a particularly reliable early sign of uremic encephalopathy and should prompt careful mental status evaluation. Both action (e.g., ataxic) and postural tremors of irregular amplitude may occur. Asterixis in persons with renal failure is another important sign of uremic encephalopathy but is seen in other metabolic encephalopathies that impair attentiveness. The asterixic flap is not an active movement but appears to occur because patients fail to maintain voluntary motor extension of the wrists or feet. The rapidity of the flap does not, however, resemble the slower relaxation of effort seen with inattention. Central inhibition of sustained motor neuron activity has also been proposed in explanation, and the phenomenon has been called a variety of “negative myoclonus.” Similar impersistence is observed with sustained eye closure or forced smiling. Truncal asterixis also occurs and may be so severe that it mimics epileptic drop attacks [Young and Shahani, 1986]. These various manifestations may improve with dialysis. Data on this subject remain scarce. A report of three adults with abnormal movements in association with uremia requiring dialysis noted either generalized or gait dyskinesias. In all three of the individuals, basal ganglia imaging changes were found (hyperintensities or hypointensities in the region of the lenticular nuclei). The lesions and the dyskinesias gradually resolved with adjustment of treatment of the uremia [Wang et al., 1998].
Muscle twitching or fasciculation, especially in the distal extremities, is common in acute renal failure. Some patients report that such activity is preceded by distal extremity muscle ache or cramping. Multifocal uremic stimulus-sensitive myoclonus, which Adams termed twitch-convulsive, often emerges as uremic stupor develops [Tyler, 1976]. Restless leg phenomenon is not uncommon in uremic encephalopathy. Tetany (i.e., tonic muscle irritability, carpopedal spasm, Trousseau sign) may develop in uremia and may not respond to calcium supplementation. Choreoathetosis and even hemiballism may be observed. Moderate to severe motor weakness (including alternating hemiplegia) may follow. In patients with chronic renal failure/ESRD, acute weakness must be distinguished from pre-existing changes related to neuropathy or hyperparathyroidism (see later). Hyperkalemia must be excluded. Rarely, signs of autonomic failure are noted, some of which may be manifestations of uremic neuropathy [Yildiz et al., 1998]. Cardiovascular autonomic dysregulation in uremia is a cause of considerable morbidity and elevates risk of mortality. It is important to measure the presence and extent of such dysfunction at the bedside. Dysfunction may include loss of parasympathetic, sympathetic, and cardiac baroreceptor responses. Unanticipated deficits may imperil patients during dialysis because of hypotension [Robinson and Carr, 2002]. In uremic diabetic individuals requiring chronic dialysis, autonomic dysfunction may result in inadequate atrial stretching that impairs secretion of atrial natriuretic factor [Zoccoli et al., 1992].
Among other treatable conditions that may require consideration are endocrinopathy or vitamin deficiency states; it should also be recognized that, in some instances, neurologic improvement may lag behind adequate correction of readily measurable metabolic parameters. Some abnormalities (e.g., emotional and intellectual) may respond quickly to dialysis, whereas others (e.g., motor and sensory) respond more slowly, persisting for an uncomfortable interval. This latency may be related to the inefficiency of dialysis in clearing unmeasured toxic intermediates. Among such substances are guanido or phenol adducts, myoinositols, and phenolic and indolic acids [Deguchi et al., 2002]. Drug screening, EEG, evoked potentials, brain imaging, bacterial cultures, and lumbar puncture may be indicated in individuals with uremic encephalopathy to detect alternative or related diagnoses. Any question of increased intracranial pressure suggested by focal neurologic signs and symptoms must be investigated urgently. Subdural or intracranial hemorrhages, stroke, and brain edema are among the causes to be excluded [Brouns and DeDeyn, 2004]. It is especially important to exclude hypertensive encephalopathy, although the contribution of this entity may be difficult to untangle from various metabolic disturbances.
In acute uremia, the EEG usually demonstrates generalized irregular but bisynchronous low-voltage slowing, particularly in patients whose blood urea nitrogen level is in excess of 60 mg/dL. The severity of these changes and prevalence of associated paroxysms roughly correlate with the further degrees of blood urea nitrogen elevation and degree of clinical encephalopathy. Slow alpha-dominant rhythm, with occasional theta bursts and characteristic prolonged bursts of bisynchronous slow-sharp activity or spike and wave, may be found. Bilateral spike discharges may accompany myoclonic jerks, and generalized electroconvulsive discharges in association with generalized convulsive seizures may also occur, possibly more commonly in patients with hypomagnesemia. Photomyoclonus and photic driving may be present. Rarely, the EEG may be normal, despite uremic encephalopathy [Röhl et al., 2007]. Bursts of high-voltage 12- to 13-Hz vertex sharp activity may be seen in drowsiness, spindles may be absent in stage 2 sleep, and high-voltage slow bursts may occur with wakening. EEG abnormalities may persist for quite some time, especially in patients with chronic renal failure for whom many months of dialysis may be required before restoration of a normal EEG pattern is seen. Deteriorations in blood urea control or other indications of transient worsening of renal function may be associated with transient intrusion of diffuse delta and theta waves, generalized spike-wave discharges, or heightened sensitivity to photic stimulation.
Infrequently, brain imaging in acute uremic encephalopathy may disclose subdural hemorrhage. Treatment may resolve encephalopathy, improve function, or in some instances fail. Some patients manifest a gyriform increase in T2-weighted signal or similar abnormalities on MRI of parietal and occipital subcortical areas, changes that reverse with treatment and must be distinguished from changes suggesting hypertensive encephalopathy. Generally, brain imaging is not of much practical value in straightforward uremic encephalopathy as it is often normal [Schmidt et al., 2001]. Abnormalities, when present, may be transient and of uncertain significance. In individuals with preceding chronic renal failure who develop uremic encephalopathy, MRI may show changes due to atrophy or visually indistinguishable corticosteroid pseudoatrophy.
The primary treatment of uremic encephalopathy is dialysis, with scrupulous attention to water balance, electrolytes, blood pressure, and ventilation. Consideration must be given to parathyroidectomy or chemical parathyroid suppression. Response to dialysis may be rapid or require many days. Fixed deficits may develop, especially when uremic encephalopathy is complicated by hypertension or CNS hemorrhage. Excessive or too rapid dialysis must be avoided because rapid shifts in water or solutes in various compartments may lead to alternative forms of neurologic decompensation. Only limited data are available concerning the possible neurophysiological or pathophysiological bases for progressive brain dysfunction due to chronic uremia. An early attempt to categorize such changes as might be found on postmortem analysis identified no distinctive pathology [Olsen, 1961]. That functional changes do occur in children with chronic renal disease has been documented [Rotundo et al., 1982; Fennell et al., 1990a, b; Crocker et al., 2002; Bawden et al., 2004]. The severity of deficits correlates with age of onset of renal failure, and includes difficulties with fine motor coordination, social adjustment, verbal and nonverbal learning and memory, and other measures of intelligence. Improvement in outcome in the wake of renal transplant is suggested by some but not other outcome studies [Fennell et al., 1984, 1990a, b].
Hypertensive Encephalopathy
The designation ‘hypertensive encephalopathy’ is generally reserved for hypertensive patients with alteration of consciousness and diffuse or multifocal CNS dysfunction, in whom there is no better or more complex etiologic explanation. Malignant hypertension, as a cause of the neurologic abnormalities of hypertensive encephalopathy, can arise in association with a number of underlying illnesses. The causes of malignant hypertension in children vary according to age [Flanigan and Vitberg, 2006]. Malignant hypertension is rare in neonates, although it may arise as the consequence of renal failure or congenital adrenal hyperplasia [Spoudeas et al., 1993]. In this age group, approximately two-thirds of cases are related to renovascular thrombosis (spontaneous or associated with asphyxia, cyanotic heart disease, disseminated intravascular coagulopathy, or umbilical artery catheterization). Nearly 20 percent of cases are due to CNS disturbances, and approximately 8 percent are caused by tumors (e.g., Wilms’ tumor, neuroblastoma) or coarctation. When hypertensive encephalopathy occurs in the first year of life, it carries a high risk of morbidity and mortality, owing to the severity of the illnesses that typically underlie pressure elevation at this young age. Causes include aortic coarctation and polycystic kidneys (each accounting for about one-third of such cases in young patients), nephritis (16 percent), and hemolytic-uremic syndrome (7 percent). The remaining cases are due to tumors that generate Cushing’s syndrome (e.g., neuroblastoma, corticotropin-secreting ganglioneuroblastoma), high doses of adrenocorticotropic hormone used to treat infantile spasms, and various forms of renovascular disease. No cases of so-called central (primarily CNS-mediated) hypertension were described in the Boston Children’s Hospital series of cases of malignant infantile hypertension [Ingelfinger, 1982]. No cases designated as representing central hypertension are to be found in the slightly earlier study by Uhari and colleagues in Sweden, either [Uhari et al., 1979]. Both studies point out that severe arterial hypertension of childhood is often unrecognized until the child presents with neurological findings.
In children older than 1 year of age, roughly two-thirds of cases are caused by inflammatory or infectious parenchymal renal disease. These include hemolytic-uremic syndrome, acute glomerulonephritis, and collagen vascular diseases (particularly systemic lupus erythematosus). Renal or aortic vascular abnormalities, such as renal artery stenosis, kidney malformations (multicystic or dysplastic kidneys), and tumors (Wilms’ tumor, neuroblastoma, pheochromocytoma), account for the remaining one-third in most centers. However, renal graft rejection may be the most frequently encountered cause of hypertensive encephalopathy in centers that perform many kidney transplants. Immunosuppression employed in such cases may increase the risk for acute hypertension, even without graft rejection [Primavera et al., 2001; Proulx et al., 1993; Still and Cottom, 1967; Stocker et al., 2003; Zangeneh et al., 2003]. More than 40 percent of patients with malignant hypertension develop significant neurologic complications, including encephalopathy. One or another of these neurologic complications was lethal in 20 percent of patients, particularly cerebral thrombosis or hemorrhage [Flynn and Tullus, 2009]. However, increasing sophistication in imaging has, particularly with the advent of MRI, applied the term reversible posterior leukoencephalopathy to at least some of these cases [Pavlakis et al., 1997]. Although the fatality rate has undoubtedly declined, fatalities still occur, especially as the result of intracranial hemorrhage [Schwartz et al., 1995b].
The risk for hypertensive encephalopathy is related to the rapidity and severity of blood pressure increases from any given baseline [Flynn and Tullus, 2009]. Risk is higher in acute renal failure caused by acute glomerulonephritis or hemolytic-uremic syndrome than it is in essential hypertension or chronic renal failure. Acute glomerulonephritis or hemolytic-uremic syndrome should be suspected in any child older than 1 month of age with unexplained hypertensive encephalopathy, even when initial laboratory findings are minimal. Some inflammatory illnesses that cause acute hypertensive renal failure in children, such as hemolytic-uremic syndrome, may have direct effects on the CNS beyond those provoked by severe hypertension. There is increasing appreciation of the manner in which the renin-angiotensin system acts in the development of hypertensive crises. This has included experience that suggests that treatment with nicardipine represents an advance over the use of sodium nitroprusside [Patel and Mitsnefes, 2005].
Generalized severe headache is almost universal with severe hypertension. Seizures and visual loss are other common early manifestations of hypertensive encephalopathy [Wright and Mathews, 1996]. Headache develops hours to days after the initiating blood pressure crisis and may be accompanied by lethargy, projectile vomiting, meningismus, or edema of the eyelids and ankles. Ophthalmoscopic findings of hypertensive encephalopathy were initially defined and classified according to the venerable scheme of Keith, Wagener, and Barker [1939]. Problems with this approach are seen in adults, as well as in children. Papilledema (KWB group 4) is present in only one-third of children with other clinical findings of hypertensive encephalopathy. The modified Scheie classification [Scheie, 1953] may be more useful, bearing in mind that children may have retinal changes consistent with grades 2 (obvious arterial narrowing with focal irregularities due to retinal arterial spasm), 3 (as with grade 2, but with the addition of retinal hemorrhages and white exudates), or 4 (as with grade 3 but with papilledema in addition). Retinal arteriolar spasm is a far more characteristic and important sign of the onset of hypertensive encephalopathy than the additional changes seen in grades 3 or 4 [Flynn and Tullus, 2009]. The white exudate (cotton-wool spots) due to ischemic infarction represents an important funduscopic finding of hypertensive encephalopathy; non-ophthalmologists involved in the care of children at risk for hypertensive encephalopathy should diligently seek to identify this finding in appropriate clinical settings [Browning et al., 2001].
The earliest non-ophthalmologic signs in newborns and infants with hypertensive encephalopathy include irritability, lethargy, and hypotonia. Infants without hypertensive encephalopathy may exhibit opisthotonos, fever, and unresponsiveness. The level of consciousness in older children consists of fluctuating confusion, irritability, and restlessness that may progress to coma. Encephalopathy in older children typically develops after 12–36 hours of headache and is often heralded by seizures, more commonly generalized than focal [Dedeoglu et al., 1996]. In virtually all cases of hypertensive encephalopathy with seizures, systolic and diastolic blood pressures are more than four standard deviations above the mean for age. Status epilepticus may further elevate systolic and diastolic blood pressures in more than 10 percent of cases. Elevation of blood pressure by four standard deviations above the mean for age should, in no case, be ascribed to seizures alone [Proulx et al., 1993]. Seizures without persistently associated mental status changes occasionally occur as the sole initial clinical manifestation of hypertensive encephalopathy.
Muscle twitching and myoclonus may occur. Focal neurologic signs may be present in various combinations of aphasia, scotomas (retinal, optic nerve, or cortical), cranial neuropathy (especially abducens or facial nerves), and focal motor weakness (especially hemiparesis). In severe cases, rapidly progressive brainstem failure may precede death, unless effective treatment is initiated [Lindfors-Lonnkvist and Jakobsson, 1994; Zangeneh et al., 2003]. Hypertension-associated occipital blindness, with additional features such as headache, lethargy, transient motor deficits, confusion, visual hallucination, and convulsive seizures (generalized more commonly than focal), constitutes a syndrome that has been termed reversible posterior leukoencephalopathy [Hinchey et al., 1996; Kwong et al., 1987; Saatci and Topaloglu, 1994; Sebire et al., 1995]. This clinically distinctive subcategory of hypertensive encephalopathy was first described in individuals receiving immunosuppression with cyclosporine. It occurs most commonly, however, in children or adults who develop acute hypertension in the setting of either acute or chronic nephrotic conditions.
Posterior Reversible Encephalopathy Syndrome
Posterior reversible encephalopathy syndrome (PRES, also termed reversible posterior leukoencephalopathy syndrome or RPLS) is thought to represent a disorder of cerebral autoregulation occurring in the setting of acute hypertension [Pande et al., 2006]. Nephrotoxic (e.g., acyclovir) or cytotoxic (e.g., cyclosporine) drugs and treatment with high doses of methylprednisolone enhance risk for the development of this syndrome, especially in patients receiving excessive fluid loads [Ikeda et al., 2001]. Cytotoxic drugs may enhance risk for PRES because they compromise the BBB [Mukherjee and McKinstry, 2001; Neuwelt, 2004]. The respiratory distress of fluid-overloaded patients may increase risk because of elevation of venous “back-pressure” of the cerebral venous circulation. Attention has been drawn to the development of MRI changes consistent with PRES in the hemisphere contralateral to predominantly hemiconvulsive seizures, suggesting that seizures themselves may have a role in the genesis and evolution of PRES [Obeid et al., 2004]. Interestingly, there has been recent demonstration that imaging changes of PRES are an important element of the MRI appearance of encephalopathy in the setting of thrombotic thrombocytopenic purpura, and that the severity of those changes tends to correspond with the severity of renal dysfunction [Burrus et al., 2010].
Brain imaging in PRES usually illustrates fairly symmetric and extensive abnormalities within 24 hours of clinical onset that are much more apparent on MRI than on computed tomography (CT). With MRI, T2-weighted bright and T1-weighted dark abnormalities usually are due to edema rather than infarction and tend to be located in the posterior parietal/occipital cortical ribbon, especially in the subjacent white matter. Changes are both cortical and subcortical, and are distributed similarly to the changes that are seen in watershed infarction. The cerebellum may be involved. Similar changes may be found elsewhere, such as in the basal ganglia or brainstem, but such changes are less common. Occasionally extensive hyperintense signal is seen in the brainstem and occasionally there is generalized white-matter edema. The changes are hypointense on T1WI weighting and hyperintense on T2WI weighting. Gradient-echo techniques may demonstrate characteristic petechial hemorrhages [Kandt et al., 1995; Weingarten et al., 1994]. In some instances, clinical and radiographic changes of reversible posterior leukoencephalopathy or of hypertensive encephalopathy do not resolve for days to as many as 8 weeks after control of hypertension. Reduction of dosage of medications such as cytotoxic or immunosuppressive agents may be required in persistent cases [Dedeoglu et al., 1996; Hinchey et al., 1996; Primavera et al., 2001].
Clinical findings and radiographic changes of PRES are similar to those found in the syndrome of cyclosporine neurotoxicity. The typical clinical appearance of PRES includes fairly sudden onset of severe headache, confusion, and visual disturbance. In a series of 22 episodes of PRES in children with renal disease, the mean age of the children was 12 years. Interestingly, for a West Virginia cadre, 45 percent of the children were African American. The prevalence of PRES in the West Virginia ESRD program for children was 9 percent. It is important to note that blood pressure was normal at the onset of PRES in 18 percent of the children. Half had considerable blood pressure elevation. Seizures occurred at the onset in 82 percent of cases, chiefly generalized convulsive seizures, with status epilepticus in only one case. Mental status was altered in 32 percent, while visual changes (black spots in the visual fields, visual hallucinations, or cortical blindness) occurred in 36 percent. Several children had recurrent PRES episodes [Onder et al., 2007]. Recurrent PRES is not uncommon [Girigsen et al., 2010]. Symptoms promptly resolve after correction of blood pressure with medications or dialysis. PRES has been described as a complication of parturition, potentially affecting the health of both mother and child [Long et al., 2007].
In cyclosporine-associated imaging changes resembling PRES, edema may be exacerbated by the effects of cyclosporine on BBB permeability rather than by any direct toxic effect of cyclosporine on the brain [Lopez-Garcia et al., 2004; Primavera et al., 2001]. Intracranial hemorrhage is more typically associated with cyclosporine-induced than other forms of hypertensive encephalopathy, probably potentiated by cyclosporine-induced thrombocytopenia [Schwartz et al., 1995a]. Changes resembling PRES develop in a minority of patients who have had long-term dialysis followed by administration of interferon-alpha in preparation for renal transplantation. Some of these individuals have chronic hepatitis C infection [Fatih et al., 2003]. Other differential considerations are acute cerebral ischemia (ACI) or acute cerebral hyperemia (ACH). The clinical setting is helpful in distinguishing these entities. PRES occurs in association with hypertension, although in some children, the clinical and imaging syndrome has arisen with normal or minimally elevated blood pressure. ACI occurs in the setting of a hypotensive event, and ACH in association with the occurrence of seizures, rapid decompression of chronic subdural hemorrhage, or rapid restoration of circulation due to angioplasty, arterectomy, or stenting [Coutts et al., 2003].
Focal clinical features of hypertensive encephalopathy are not always transient. Aphasia, optic nerve scotomas, and hemiparesis may indicate the occurrence of brain, cranial nerve, or brainstem infarction. Unilateral infarction of some portion of the anterior optic pathways is especially characteristic. Infarction may be more common in patients who have had long-standing unrecognized hypertension. It also occurs in individuals who experience hypotensive episodes due to overly aggressive management of blood pressure elevation [Sebire et al., 1995; Browning et al., 2001]. These data suggest the importance of early specialist evaluation of visual function in at-risk individuals to assure that deteriorating vision is urgently evaluated and treated. It is as yet unclear if infarctions are due to vasculopathy or to impairment of blood flow related to edema and hypotension.
Information concerning the pathologic changes that occur in hypertensive encephalopathy is scant. Perivascular edema (with or without microhemorrhages) and swelling of astrocytes and myelin have been described [Lumsden, 1970].
The exact nature of the pathophysiology of hypertensive encephalopathy is not fully understood, but two major theories are advocated. An older view states that encephalopathy is the result of excessive cerebral vasoconstrictive autoregulation, stimulated to protect cerebral microvascularity from high pressure. This reduction of microcirculatory flow is believed to compromise capillary integrity and result in edema, vascular necrosis, microinfarction, and petechial hemorrhages. This sequence has been demonstrated in experimental models [Finnerty, 1972]. A newer hypothesis suggests that hypertensive encephalopathy is actually the result of failure of cerebral (with associated retinal vascular) autoregulation. In this model, the vasoconstrictive threshold is exceeded and transudative perivascular edema develops, which may then compress the regional microvasculature. This process, perhaps in combination with back-pressure related to venous hypertension, may then result in proliferative endarteritis of retinal and cerebral arterioles with focal ischemic fibrinoid necrosis, petechial hemorrhages, and parenchymal microhemorrhages [Gulliksen et al., 1983]. Loss of autoregulation, significantly impairing vascular compensation in intercurrent hypotensive episodes, may render the individual vulnerable to infarction in areas of vascular watershed across the parasagittal and deep gray regions of the cerebral hemispheres.
Neither theory has been proved, although experimental and clinical observations have been advanced supporting both. Although it is known that hypertension is necessary, it is not known whether it is sufficient to cause hypertensive encephalopathy or whether other inciting circumstances are required. Regardless of the initial event, microinfarction, edema formation, and loss of autoregulation do occur, necessitating caution in blood pressure reduction and manipulation of cardiac output because rapid changes may result in acute cerebral infarction [Healton et al., 1982]. Generally, intact cerebral autoregulatory mechanisms are capable of blunting systolic arterial pressure elevations as high as 200 mmHg in adolescents and adults [Strandgaard et al., 1973]. These mechanisms can adapt to even greater pressures in patients with chronic hypertension. On the other hand, children with chronic renal disease may experience particularly acute and severe episodes of hypertension. This vulnerability is ascribed to chronic volume expansion, renovascular constriction that results in increased plasma renin and angiotensin II, and increased vascular responsiveness to angiotensin II owing to increased plasma Na+/K+ adenosine triphosphatase inhibitor [de Wardener and MacGregor, 1988].
The upper limits of vascular autoregulation in the newborn are more uncertain than in older individuals, and little is known about cerebrovascular autoregulation in young children in a hypertensive state [Fraser and Arieff, 1988]. Autoregulatory responses become more complex when metabolic homeostasis is disturbed. Both acidosis and carbon dioxide accumulation prompt cerebral arteriolar dilatation and may permit higher pressure to be conveyed to the delicate microcirculation of the brain, perhaps lowering the pressure threshold for decompensation. This effect is best illustrated by the fact that only moderate blood pressure elevation is required to produce hypertensive encephalopathy in some children with acute pulmonary edema. Abnormalities observed with MR perfusion imaging support the concept that vasodilatation is an important aspect of vulnerability to hypertensive encephalopathy [Jones et al., 1997]. There is no clear explanation for the occipital preponderance of MRI-demonstrated changes in brain appearances, although it seems likely that there are physiologic or anatomic differences in the blood vessels or associated BBB in posterior brain regions [Kandt et al., 1995].
As has been noted, acute hypertension, severe headache, and encephalopathy progressing over several days is highly suggestive of hypertensive encephalopathy, particularly if there is funduscopic evidence of arteriolar spasm or ischemic infarction of nerve fibers. It should be recalled that inflammatory vasculitides (especially systemic lupus erythematosus) associated with a chronic hypertensive state often produce similar retinal changes, even without hypertensive encephalopathy. Acute hypertensive encephalopathy associated with acute dependent edema and hematuria suggests the possibility of acute post-streptococcal glomerulonephritis. Diagnoses such as eclampsia, complications of immunosuppression, or acetaminophen-induced hepatorenal failure will be suggested by the clinical setting [Hinchey et al., 1996; Saatci and Topaloglu, 1994]. When appropriate, structural CNS lesions (tumor, hemorrhage, or stroke) should be excluded by unenhanced brain imaging because the presence of such lesions may influence blood pressure management. In some cases it is difficult to exclude ischemic brain injury without serial imaging. Cerebral hemorrhage in hypertensive encephalopathy is usually petechial. In the preadolescent patient, any large brain hemorrhage is more likely the cause than the result of hypertension, except in patients with cyclosporine-induced thrombocytopenia [Schwartz et al., 1995a].
Prompt remission with control of blood pressure is the most important confirmation of hypertensive encephalopathy [Hinchey et al., 1996; Kandt et al., 1995]. Medications employed in the management of blood pressure in children are shown in Box 102-2. Selection, utilization, side effects, and detailed dosage considerations for these medications fall outside the scope of this chapter. All patients should initially be managed as if cerebral edema is present. The fundamental steps include elevation of the head of the bed by 30 degrees and careful attention to free water balance. Further decisions about treatment depend on etiology. Unless hypertension is very severe, drug therapy should not be undertaken until space-occupying CNS lesions (stroke, tumor, hemorrhage) and the brittle dysautonomia of Guillain–Barré syndrome are excluded. Other important etiologic considerations for acute encephalopathy include intoxication, acute pulmonary edema, acute pancreatitis, and endocrine (e.g., pheochromocytoma) or metabolic diseases. Rarely, an acute anxiety reaction with hypertension and pseudoencephalopathy must be excluded. A careful history and examination should determine the selection of appropriate laboratory tests.



































If severe blood pressure elevation and the threat of permanent CNS injury (e.g., rapidly progressive visual loss) are present, blood pressure should be treated medically [Thien et al., 1979]. Care should be taken not to reduce the mean arterial pressure to less than the lower limit of cerebral blood flow autoregulation. Below this level, maximal autoregulatory vasodilatation fails to prevent cerebral ischemia, and permanent nervous system injury may result [Brown et al., 1987; Sebire et al., 1995]. Predicting this lower limit is difficult, given age-related variation, as well as the fact that chronic hypertension may reduce the vasodilatory capacity of arterioles and thus raise the mean pressure at which decompensation occurs. Within these limits for blood pressure reduction, aggressive treatment is likely to be well tolerated, except in the setting of increased intracranial pressure and dysautonomia, as in Guillain–Barré syndrome. The risk for neurologic sequelae (blindness, coma, pyramidal tract injury) from iatrogenic hypotension is related not only to the severity but also to the duration of hypotension [Franklin, 1984].
In most patients with childhood-accelerated hypertension, aggressive and safe blood pressure reduction can be achieved with intravenous sodium nitroprusside. This high-potency, brief-duration agent provides the considerable advantage of momentary titration to the responses of the individual patient. Sustained use in renal failure carries the risk of intoxication. Labetalol is another useful intravenous medication, but the longer duration of action is disadvantageous or even dangerous if hypotension develops. In patients with less severe elevations of blood pressure, hydralazine or nifedipine may be used [Kandt et al., 1995]. Captopril is a particularly useful oral agent in patients with renin-dependent hypertension (essential, renovascular, hemolytic-uremic syndrome, or related to thrombotic thrombocytopenic purpura). Advantages produced by replacement of sodium nitroprusside with nicardipine for the treatment of childhood hypertension have been reported by some [Patel and Mitsnefes, 2005]. Diazoxide is the medication most commonly associated with untoward hypotensive reduction of blood pressure with deleterious consequences. Large-bore venous access should be secured in every patient against the possibility of sudden hypotension, whatever therapeutic approach is undertaken. Some authorities recommend that acute treatment of hypertension in the neonate be undertaken with the calcium channel blocker, nicardipine, although this medication has been associated with reflex tachycardia. This complication is not so frequently encountered as it is with hydralazine. Enalopril has been advocated for use in neonatal renovascular hypertension, although this agent must be used – as is the case with all antihypertensives in the neonate – with extreme care [Wells et al., 1990]. Sodium nitroprusside may pose a greater risk for intoxication, and both methyldopa and reserpine may cause profound sedation.
Acute management of severe cerebral edema may involve mechanical hyperventilation, osmotic agents, or corticosteroids. In such instances, placement of an intracranial pressure monitor should be considered, especially with hyperventilation, because this action is associated with risk for reflexive cerebral capacitance vessel vasoconstriction that may worsen cerebral and brainstem perfusion defects. Osmotic agents may accumulate in acute renal failure and should be carefully dialyzed. Some patients respond slowly to treatment or develop permanent deficits, particularly visual and motor ones [Hulse et al., 1979]. Antiepileptic medications should be administered to children with acute, persistent seizures, but chronic anticonvulsant therapy is seldom required. Chronic hypertension carries a significant risk for seizures, cerebral thrombosis/hemorrhage, subarachnoid hemorrhage, and Bell’s palsy, even if acute hypertensive encephalopathy does not occur. In children and adolescents, the visual acuity deficits associated with malignant hypertension may fairly promptly improve with control of blood pressure. However, late deterioration of visual function and even blindness may develop over the longer term by processes including macular membranous choroidal neovascularization of progressive optic neuropathy. The degree and duration of the hypertensive phase appear to be important elements in the risk for such devastating reversion of visual dysfunction, underlining the importance of early diagnosis and treatment [Browning et al., 2001].
Some adults develop a subacute progressive hypertensive encephalopathy with pathologically identifiable changes in the deep cerebral microvasculature [Fisher, 1998]. It is unclear whether chronic hypertension or multiple episodes of acute blood pressure elevation produce similar changes in children. A number of antihypertensive medications may impair intellectual function of children and adults. Of particular importance are methyldopa, reserpine, propranolol, and clonidine. These changes may be due in part to sedation (usually transient), sleep disturbance, or depression [Light, 1980].
Complications of Chronic Renal Failure
Current estimate of the incidence of chronic renal disease in individuals less than 20 years of age may be as high as 58 per million [Seikaly et al., 2003]. Although variation in epidemiological methodology and in assignment of diagnosis must be taken into account, many authorities are concerned that there is a significant rise in prevalence of serious kidney disease in Western countries. In the United States, increase in risk may be particularly high for individuals of African American ancestry [Choi et al., 2009]. Data from the North American Pediatric Renal Transplant Study shows that 65.9 percent of those registered for transplantation are male and 63.9 percent are “white” [Benfield et al., 1999]. Although the pecise constituency of non-white individuals is not provided, black children constitute only approximately 13% rather than 36% of the North American population. An estimate of the prevalence of Western European chronic renal failure is 32.4 per million children. Of these children, 6 percent are less than 3 years of age, 30 percent are 3–9 years of age, and 64 percent are 9–15 years of age.
Congenital Uremic Encephalopathy
Severe chronic uremia (glomerular filtration rate  10 percent of normal), developing in the first year of life, carries a very high risk for ensuing subacute progressive encephalopathy [Valanne et al., 2004]. Most of these infants have inherited forms of nephrosis, particularly congenital nephrosis of the Finnish type. It is possible that some of the neurologic abnormalities noted in these infants are independently inherited developmental abnormalities or due to the prenatal metabolic effects of nephrosis. The appearance of abnormalities may appear after a latent interval. Early provision of dialysis has not prevented development of congenital uremic encephalopathy. Some children with genetically determined congenital nephroses have worse neurologic outcomes than others. There is emerging evidence concerning coexpression of defective enzymes in brain and kidney that may account for abnormal development and function of both organs. An important research priority remains that of discovering
10 percent of normal), developing in the first year of life, carries a very high risk for ensuing subacute progressive encephalopathy [Valanne et al., 2004]. Most of these infants have inherited forms of nephrosis, particularly congenital nephrosis of the Finnish type. It is possible that some of the neurologic abnormalities noted in these infants are independently inherited developmental abnormalities or due to the prenatal metabolic effects of nephrosis. The appearance of abnormalities may appear after a latent interval. Early provision of dialysis has not prevented development of congenital uremic encephalopathy. Some children with genetically determined congenital nephroses have worse neurologic outcomes than others. There is emerging evidence concerning coexpression of defective enzymes in brain and kidney that may account for abnormal development and function of both organs. An important research priority remains that of discovering
Older studies have tended to group together all individuals with infantile onset of severe renal failure (those that survive the neonatal period) for follow-up studies, without consideration of varied genetic causes that are now appreciated. These studies have proved that more than two-thirds of such children manifested seizures and developmental arrest in the first year of life, followed in the second year by developmental regression with acquired microcephaly [Polinsky et al., 1987; Sedman and Wilkening, 1984]. By several years of age, 60–80 percent have epilepsy (focal or generalized), as well as moderate to severe motor, cognitive, language, and psychosocial delay [McGraw et al., 1986; Rotundo et al., 1982]. By comparison, studies from the same era found that at least 90 percent of children who developed ESRD after early infancy enjoyed normal psychomotor development, even if assessed after far greater durations of illness and dialysis [Rasbury et al., 1983].
Despite careful attention to nutrition and metabolic parameters, the linear growth of the majority of children with infantile-onset ESRD is reduced. More than two-thirds of these children have acquired microcephaly. Craniosynostosis develops in a small number. Neurologic abnormalities include varied degrees of ataxia, choreoathetosis, facial myoclonus, hypotonicity, weakness, and hyperreflexia. If language develops, it is often compromised by dysarthria and lingual apraxia [Polinsky et al., 1987]. Most children with congenital uremic encephalopathy die within the first few years of life, often from progressive bulbar failure [Rotundo et al., 1982]. No evidence exists that renal transplantation reverses or even arrests progression of congenital uremic encephalopathy. Improved neurologic function with dialysis remains a reliable way to distinguish acute infantile uremia with encephalopathy from congenital nephrosis with progressive uremic encephalopathy that does not manifest improvement [McGraw et al., 1986]. Inexorable decline in neurologic function and somatic growth, despite careful attention to metabolic parameters, is so characteristic that the diagnosis of congenital progressive uremic encephalopathy can usually be made on clinical grounds.
The EEG initially indicates generalized slowing in either form of encephalopathy, but in the congenital progressive form, EEG organization deteriorates in a fashion parallel to observed neurologic deterioration despite treatment, with the development of paroxysmal sharp, rhythmic slow, or polyspike-wave discharges. The EEG findings improve in infantile uremia with encephalopathy in a fashion that roughly parallels improvement in the clinical capacities of the appropriately treated infant. These characteristic paroxysms resemble those observed in older children and adults with progressive dialysis encephalopathy. Brain imaging of infants with progressive uremic encephalopathy due to congenital nephrosis usually reveals brain atrophy [McGraw and Haka-Ikse, 1985], although pseudoatrophy due to the concurrent use of corticosteroids in many of these children makes interpretation of scans difficult until encephalomalacia is fairly advanced. Pathologic examination of the brain of children with congenital nephrotic syndromes has confirmed that sulcal widening and enlarged ventricles are the result of neuronal loss greatest in the cerebral cortex, brainstem sensory nuclei, and reticular formation [Papageorgiou et al., 1982]. The volume loss is compounded by Wallerian degeneration in the subcortical and brainstem fiber pathways.
Most children with congenital nephrosis have inherited the severe Finnish type. It is an autosomal-recessive condition due to mutations in both nephrin gene (NPHS1) alleles. Many of these children are born a month or so before term and have low birth weight, microcephaly, ascites, edema, and massive proteinuria. Suspicion of this condition is raised by the detection of persistent elevation of amniotic fluid α-fetoprotein without evidence for neural tube defects. The severity of the Finnish type of congenital nephrosis has led to termination of some pregnancies [Overstreet et al., 2002]. Many infants with Finnish-type congenital nephrosis die in the first few weeks or months of life. This genetic defect results in structural and functional abnormalities of the podocyte foot processes and slit-diaphragm structures of the developing kidney [Finn, 2003; Pollak, 2003; Valanne et al., 2004]. These infants lack renal expression of nephrin and have diminished expression of synaptopodin and GLEPP1, proteins that are crucial to the assembly of the kidney podocyte and associated structures. It has recently been discovered that these proteins are also expressed in neurons. Their function in the nervous system is as yet uncertain, although they may play a role in synaptic plasticity [Deller et al., 2000, 2002, 2003; Mundell et al., 1997; Mundell and Kelly, 1998].
Some children with congenital nephrosis have corticosteroid-resistant focal segmental glomerulosclerosis. Often, these children also have neurologic abnormalities. This form of congenital nephrosis occurs as the result of mutations of both podocin gene (NPHS2) alleles. The relation between nephrin, podocin, α-actinin-4 (ACTN4), and other genes whose proteins are co-expressed in kidney and brain to the poor neurologic development in many children with severe congenital renal disease remains unclear. Diminished expression of these various proteins is also found in renal conditions such as minimal change disease, which is not associated with neurologic abnormalities. In addition to genetic conditions that affect kidney structure, metabolic conditions such as type 1 carbohydrate-deficient glycoprotein disease may produce the phenotype of congenital renal failure with abnormal growth and neurologic dysfunction [Drouin-Garraud et al., 2001].
Galloway–Mowat, arthrogryposis, renal dysfunction, and cholestasis (ARC), and progressive encephalopathy with edema, hypsarrhythmia, and optic atrophy (PEHO) syndrome are among the heterogenous collection of phenotypes with early-onset nephropathy associated with various neurologic abnormalities. The Galloway–Mowat phenotype includes children with microcephaly, cerebellar atrophy or hypoplasia, and nephrosis due to focal segmental glomerulosclerosis that may not become clinically apparent until several years of age. ESRD may not develop until near the end of the first decade of life [Shiihara et al., 2003]. Certain potentially deleterious but preventable postnatal influences on neurologic development in children with congenital or early childhood chronic renal failure have been identified. These include aluminum toxicity, vascular accidents, chronic uremia, hypertension, malnutrition, circulatory disturbances, and psychosocial deprivation [Elzouki et al., 1994].
Aluminum toxicity
Approximately 90 percent of individuals with kidney failure take oral phosphate binders. There has been a recent suggestion that aluminum toxicity may be a cause of autistic spectrum disorders [Blaylock and Strunecka, 2009]. Infants, children, and adults with impaired renal function who are not being treated with dialysis are at risk for aluminum toxicity, due not only to the oral administration of phosphate binders, but also to use of calcium and phosphorus salts or albumin containing high levels of aluminum. Some infant formulas have been found to contain unacceptably high aluminum concentrations – especially soy formulas and formulas prepared for premature infants. The risk is highest for premature infants and in those with impaired renal function [AAP Committee on Nutrition, 1996]. Newer and stronger regulation remains an important concern worldwide [Poole et al., 2008; Bhatia and Greer, 2008]. The use of oral phosphate binders has been the subject of a recent thoughtful review [Tonelli et al., 2010]. The issues of possible aluminum toxicity as an element of dialysis encephalopathy will be considered in the next section.
It has been suggested, on the basis of limited information, that the known neurotoxicities of aluminum are due to alteration of cellular repair mechanisms, derangement of neurotransmitter or energy metabolism, or deleterious affects on vascular reactivity [Polinsky and Gruskin, 1984; Starkey, 1987; Wilson and Fearon, 1984]. It has also been suggested that aluminum may serve as an adjuvant for the toxic effects of other circulating toxins. It may alter membrane (e.g., BBB) characteristics, permitting greater access of toxins to the CNS. Sources of aluminum have included water (used in dialysate or commercially prepared infant formula), intravenous solutions, parenteral medications, and especially the aluminum salts administered to control hyperphosphatemia [McGraw et al., 1986; Milliner et al., 1985; Sedman et al., 1985]. Bladder irrigation with alum as a treatment for hemorrhagic cystitis has resulted in acute encephalopathic deterioration of patients with chronic renal failure [Perazella and Brown, 1993]. Infants with congenital uremic encephalopathy have been found to have serum, bone, and brain concentrations of aluminum that exceed control values by up to 25-fold [Andreoli et al., 1984; Freundlich et al., 1985; Nathan and Pedersen, 1980].
Serum levels of aluminum do not correlate directly with the degree of putative neurotoxicities observed in a given individual [Sedman et al., 1984]. Infants at high risk for aluminum toxicity had one or more of the following:
Management of infantile chronic renal failure without the use of aluminum salts has greatly diminished the prevalence of progressive nephrotic encephalopathy. In one study, infants managed without these salts who receive vigorous nutritional and psychosocial support have demonstrated markedly improved neurologic outcome by 4 years of age. Neurologic examinations of such children may indicate only hypotonia. Microcephaly is found in approximately one-third, brain atrophy in 20 percent, developmental delay in 20 percent, and neuropathy in less than 15 percent [Elzouki et al., 1994]. On the other hand, congenital uremic encephalopathy has developed in some infants who have never received aluminum-containing phosphate binders.
Stroke
Vascular accidents may cause acquired neurologic injuries in children with congenital nephroses. At 6–11 years of age, 50 percent of brains of children who have onset of nephrosis in the first year of life have vascular border zone abnormalities, mostly mild, suggesting prior ischemic brain injury. A smaller percentage has large artery territory or basal ganglia infarcts, and some have brain atrophy. The presence of lesions suggesting vascular territory infarctions appears to correlate with a history of pretransplantation hemodynamic crises and with greater duration of management by dialysis before renal transplantation [Valanne et al., 2004]. Attention devoted to ensuring hemodynamic stability in infants undergoing dialysis for chronic renal failure and early consideration of transplantation may improve outcome. Evidence has also accumulated concerning the likelihood of beneficial effects of folate, pyridoxine, and cobalamin administration with regard to the prevention of stroke in individuals undergoing peritoneal dialysis [Righetti et al., 2006; Bazzano et al., 2006; Wang et al., 2002].
Malnutrition
Head circumference is a reliable index of brain injury in malnourished infants with congenital uremic encephalopathy [Winick et al., 1971]. That severe encephalopathy does not develop in most patients with malabsorption syndromes, despite poor somatic growth, suggests that factors other than nutrition are of greater importance in producing this vulnerability to poor brain growth in children with congenital uremic encephalopathy [McGraw and Haka-Ikse, 1985]. Tube feedings and special formulas have improved growth but do not appear to prevent congenital uremic encephalopathy.
Nutritional disorders are difficult to dissociate from the metabolic and endocrine dysfunction of chronic renal failure. Recent information suggests that vitamin B12 deficiency with abnormalities of methionine metabolism and hyperhomocystinuria may contribute to neurologic abnormalities [Herrmann and Knapp, 2002]. Renal osteodystrophy and hyperparathyroidism, routinely found in patients with congenital renal failure, have long been appreciated as factors of importance in developmental and growth delay. Osteodystrophy may secondarily impair gross motor function but does not explain the significant delay exhibited by these patients in other areas of development.
Endocrinopathy
Hyperparathyroidism and either hypercalcemia or hypocalcemia may directly injure the nervous system [Seyahi et al., 2004]. Uremia with hyperparathyroidism is associated with slowing of the EEG and may increase brain calcium to the extent that cerebral calcification results. This calcification is found in the subcortex and basal ganglia in children, rather than the cortical and hypothalamic calcifications more typical of adults with ESRD. Parathyroid hormone excess may directly affect neurotransmission in brain [Smit, 1983]. Studies in animals and human adults have found that encephalopathy may be prevented or ameliorated with parathyroidectomy [Akmal et al., 1984]. Poor somatic growth in congenital chronic renal failure has been ascribed in part to hypothalamic-pituitary dysfunction [Schmitz and Moller, 1983]. It has been found that normalization of parathyroid hormone leads to acceleration of growth velocity and “catch-up” growth in children with chronic renal failure [Waller et al., 2003].
Some patients with congenital onset of chronic renal failure have fulminant deterioration in neurologic function at some point in their course. Often, this deterioration occurs in association with infection or severe metabolic decompensation, or after surgery, including renal transplantation [Griswold et al., 1983]. In such patients, CNS infection, hemorrhage, electrolyte disturbances, intoxications, and hypertension must be excluded.
Complications of Dialysis
Dialysis is efficacious in the remediation or prevention of acute uremic encephalopathy in patients with severe renal failure, and is also beneficial in the treatment of uremic peripheral neuropathy and of some cases of acquired deafness [Mitschke et al., 1975]. Dialysis is associated with many potential complications of greater or lesser significance. Many are neurologic, including headache, dialysis disequilibrium syndrome, thiamine and carnitine deficiencies, intracranial hemorrhage, and progressive dialysis encephalopathy. Problems related to the preparation of dialysis fluids are now seldom encountered. When they do occur, they tend to manifest as seizures or decline in mental status. Once such improperly prepared fluids are identified, a satisfactory outcome may be achieved after gradual correction with properly prepared dialysate, even after severe hypernatremia [Borrego Dominguez et al., 2003].
The prevalence of each of the various complications of dialysis varies from common to rare. Headache (2–25 percent) or cramps (15–50 percent) are common. Exceedingly rare complications in children include Wernicke’s encephalopathy (due to dialysis-induced thiamine deficiency) and dialysis-associated amyloidosis [Lopez and Collins, 1968; Rosa et al., 1980]. So far as we can determine, only one case of dialysis-associated Wernicke’s encephalopathy has been reported in the medical literature as having occurred in a person under 18 years of age [Ueda et al., 2007] since the entity was described in 1968 [Lopez and Collins, 1968]. Childhood dialysis-associated amyloidosis is a heterogeneous entity and is chiefly a complication that occurs when dialysis is necessary in individuals who manifest underlying chronic inflammatory, infectious, or heredofamilial diseases. In resource-rich nations, it has occurred in the setting of rheumatoid arthritis, while in resource-poor nations and Mediterranean countries, untreated familial Mediterranean fever is a very important cause [Tinaztepe, 1995]. The incidence of many complications has decreased markedly in the past decade, particularly dialysis disequilibrium syndrome. Episodic hypertension is a common concern in patients undergoing dialysis, and may be associated with hypertensive encephalopathy, brain hemorrhage, severe headache, and pulmonary edema. It is caused by extracellular fluid accumulation between dialysis sessions and the secretion of large amounts of renin, especially during and immediately after dialysis sessions. Hemodialyzed patients (in North America this may be particularly true of African Americans) may develop encephalopathy with hypertension related to acute pancreatitis [Avram, 1977], although there are no subsequent reports. Vulnerability to pancreatitis and encephalopathy is a rarity that is also found in dialyzed adolescents with lupus nephritis [Levy et al., 1991].
The frequency of dialysis-associated headache is unclear, with various reports suggesting figures between 2 and 70 percent of patients with chronic renal failure/ESRD [Antoniazzi et al., 2002; Goksan et al., 2004]. There is no reliable information concerning the frequency of headache in children who undergo dialysis. Mild to moderate headache is not uncommonly reported by older children. Criteria for diagnosis have been established by the International Headache Society, and these require headache related to dialysis to begin during hemodialysis and terminate within 24 hours of onset [Antoniazzi et al., 2003]. It is likely that dialysis headache is prompted by water and electrolyte shifts or by other aspects of dialysis disequilibrium. Risk can be reduced by adjustment of dialysis parameters, including the use of sodium modeling programs during dialysis rather than administering a constant concentration of dialysate sodium [Sadowski et al., 1993]. Dialysis headache may share some of the mechanisms of water-deprivation headache [Blau et al., 2004]. Patients with higher predialysis systolic and diastolic blood pressure may be at greater risk for headache, as well as those who experience dialysis-related hypotension or weight loss [Antoniazzi et al., 2002; Goksan et al., 2004].
Our experience suggests that at least half the children who experience dialysis-associated headaches have historical evidence for a migrainous disorder, although their worst headaches may develop only with dialysis. Family history, occurrence of throbbing hemicrania, and relief with sleep support the diagnosis of migraine. Migrainous dialysis headache develops after several hours of dialysis, usually with bilaterally throbbing pain, but pain may have a viselike or dull quality. Various other analgesics have been employed successfully, including dipyrone [Antoniazzi et al., 2002]. There is as yet no information on the risks and benefits of triptans in this setting. Children or adolescents who do not have a history of migrainous headaches may also develop headaches of mild to moderate severity after 3–4 hours of dialysis. These headaches often respond to acetaminophen, with or without butalbital. Headache can result from readily detectable metabolic abnormalities (e.g., hypernatremic cellular dehydration or water intoxication), which must, in some instances, be excluded. Hypertension or subdural hemorrhage should be considered when headache is more severe or persistent, particularly if obtundation or new focal neurologic signs are present. Use of worn-out cellulose acetate dialysis membranes has been blamed for an outbreak of postdialysis headache and, in some instances, loss of hearing or vision (with corneal opacity) [Hutter et al., 2000].
Dialysis Disequilibrium Syndrome
Dialysis disequilibrium syndrome is a variable but distinctive mixture of neurologic symptoms and signs that are particularly likely to occur in the early phases of a dialysis program. In the early days of dialysis, disequilibrium syndrome occurred in nearly 10 percent of adults and more than 30 percent of children [Tyler and Tyler, 1984]. The most common manifestations are irritability or restlessness, fatigue, headache, nausea, blurred vision, muscle cramps, and, in some instances, twitching. Hypertension, tremulousness, vomiting, disorientation, agitated delirium, seizures, visual loss, elevated intraocular pressure, papilledema, and asterixis are sometimes seen. Wernicke’s encephalopathy has been reported rarely. Coma may develop, and death may occur from central herniation [Milutinovich et al., 1979]. EEG changes are usually limited to variable degrees of background slowing. The syndrome is particularly likely to occur with recently initiated dialysis, utilization of rapid dialysis protocol, or dialysis with ultrafiltration [Kerr, 1980; Young et al., 1988]. The onset may be from 3 to 4 hours after initiation, or as late as 20 hours after the completion of a dialysis session. Intellectual dysfunction, psychiatric symptoms, and visual abnormalities are usually self-limited, lasting for several hours. These problems may, in some instances, persist for several days. It is likely that subtle and unrecognized intellectual dysfunction occurs not infrequently in the early stages of dialysis as a manifestation of mild dialysis disequilibrium syndrome. Dialysis with rapid correction of hyponatremia has been blamed for one case of fatal pontine myelinolysis [Loo et al., 1995].
The term osmotic demyelination has been applied to some patients who experience deterioration of neurologic function after dialysis and are found to have hypointense abnormalities on T2-weighted MRI in the region of the pons. These changes may be found also in some patients with dialysis-associated seizures or mild disturbances of consciousness. Repeat scans usually demonstrate the rapid and complete disappearance of these changes, the imaging characteristics of which are consistent with edema. It is likely that many individuals with dialysis disequilibrium have merely developed transient dialysis-related brain edema rather than demyelination [Tarhan et al., 2004]. Dialysis removes osmotically active molecules from blood more rapidly than they can diffuse out of the brain. This movement results in an osmotic gradient that provokes net flow of water into the brain, resulting in cerebral edema, increased intracranial pressure, and encephalopathy [Arieff et al., 1973].
These deleterious osmotic gradients were ascribed to effects of urea (“reverse urea syndrome”) because dialysis disequilibrium syndrome did not appear to develop when nonuremic patients were dialyzed, but studies failed to provide convincing evidence of a significant urea gradient. Urea enters the brain at a very slow rate, but the use of a urea-containing dialysate has failed to prevent edema. Another theory suggested that osmotic activity is the result of retention within the brain, or of nonurea “middle molecules” or “idiogenic osmoles” [Arieff et al., 1973]. The fall in CSF pH that may occur during dialysis was cited as indirect evidence for the accumulation of osmotically active organic acid and amine “middle molecules” in the CNS of patients with chronic renal failure [Arieff et al., 1973]. Another study found no evidence for any additional contribution by “idiogenic osmoles” to dialysis-induced cerebral edema [Silver et al., 1992]. Short echo-time MR spectroscopy has documented changes in cerebral concentration of myoinositol, choline-containing compounds, and water in brain during dialysis. These changes were greater in gray matter than in white matter [Michaelis et al., 1996].
Modifications in dialysis protocols have significantly reduced the frequency of dialysis disequilibrium. These modifications have included changes in dialysis priming, increased dialysate salt concentration, inclusion of colloids, such as mannitol and albumin, limitation of dialysis to 10 percent of blood volume, and more gradual initial reduction of blood urea nitrogen to the range of 70–80 mg/dL. The most important element in preventing dialysis disequilibrium is early diagnosis and dialysis, so that profound azotemia (blood urea nitrogen  200 mg/dL) is rarely encountered [Arieff et al., 1978; Port et al., 1973]. If dialysis disequilibrium is severe, mannitol administration may be beneficial. The use of mannitol must be carefully coordinated with dialysis to ensure that the mannitol and mobilized fluid are removed from the circulation with appropriate speed. Seizures due to dialysis disequilibrium are usually transient.
200 mg/dL) is rarely encountered [Arieff et al., 1978; Port et al., 1973]. If dialysis disequilibrium is severe, mannitol administration may be beneficial. The use of mannitol must be carefully coordinated with dialysis to ensure that the mannitol and mobilized fluid are removed from the circulation with appropriate speed. Seizures due to dialysis disequilibrium are usually transient.
Dialysis-Associated Seizures
Dialysis-associated seizures occur in 7–10 percent of children (newborn to 21 years) with ESRD. Most are generalized tonic-clonic seizures that occur during or shortly after dialysis [Swartz et al., 1983]. They are more commonly associated with hemodialysis (8–9 percent) than peritoneal dialysis (0–4 percent), and are likely due to chemical or osmotic disequilibria. The risk for dialysis-associated seizures is as high as 29 percent in children with a history of seizures [Glenn et al., 1992]. The most recent large-scale review with regard to prevalence of seizures in dialyzed individuals less than 23 years of age showed that dialysis-associated seizures continue to occur in about 7.2 percent of their 180 dialyzed individuals. Of these, 92 percent occurred during hemodialysis and 8 percent during peritoneal dialysis. Of the patients who experienced a seizure with hemodialysis, repeat hemodialysis carried a 29 percent risk for recurrence [Glenn et al., 1992]. Other risk factors noted in older literature are young age, malignant hypertension, or encephalopathy due to uremia, dialysis disequilibrium, or congenital uremic encephalopathy [Swartz et al., 1983]. However, a recent Finnish series showed no dialysis-associated seizures in their series of 23 children undergoing chronic peritoneal dialysis. In this series, 73 percent had heritable renal disease, especially Finnish-type congenital nephrotic syndrome [Laakkonen et al., 2008]. Seizures are more likely to occur during the early phases of a dialysis program, when solute changes are the greatest. Increased risk with hemodialysis may be related to more rapid clearance of electrolytes and other osmotically active solutes by this method than by peritoneal dialysis [Glenn et al., 1992]. The frequency of dialysis-associated seizures in older children and in children who have undergone dialysis for more than 2 months may be accounted for by the greater likelihood of hemodialysis in those groups [Glenn et al., 1992]. Severe azotemia (blood urea nitrogen >200 mg/dL), hypocalcemia (<6 mg/dL), hypomagnesemia (<1 mg/dL), anemia (hemoglobin <5 mg/dL), hypertonicity, acidosis, and hypoxemia also increase the risk for dialysis-associated seizures [Swartz et al., 1983].
MRI abnormalities suggesting edema in the pons, as well as in extrapontine locations, have been noted in some individuals with dialysis-related seizures. These changes resemble those seen in dialysis disequilibrium syndrome [Tarhan et al., 2004]. MRI changes of PRES, often occurring in the setting of seizures, have been discussed. The EEG may indicate frontal intermittent rhythmic delta and diffuse slowing, with prominent photic activation [Watemberg et al., 2002]. These changes have been interpreted by some as representing the presence of old structural injury, perhaps related to ischemic watershed infarction [Watemberg et al., 2002]. The efficacy of antiepileptic drugs in treating or preventing dialysis-associated seizures is poorly defined. The use of readily dialyzable medications may increase the risk for dialysis-associated seizures because these drugs are removed at the same time as the dialytic metabolic stress may induce seizures. In individuals chronically treated with antiseizure medications, dialysis-associated seizures may, of course, be due to dialysis-related reduction of antiseizure medication concentration. Management issues related to this will be considered in another section.
Vitamin and Co-factor Deficiencies
The B vitamins are water-soluble, and most are readily dialyzable. A single dialysis session may reduce plasma thiamine concentration by as much as 40 percent. Patients with ESRD continue to be at risk for thiamine deficiency, which may present as confusion progressing rapidly to obtundation or coma [Don et al., 2010]. Associated findings may include chorea, visual loss, ophthalmoparesis, ataxia, myoclonus, or seizures. It has been estimated that this deficiency may account for as many as one-third of all cases of unexplained acute encephalopathy in chronically dialyzed adults [Hung et al., 2001a, b]. It is somewhat surprising that symptomatic thiamine deficiency has been reported only rarely in children, probably because stores of thiamine accumulated before the development of renal disease are only gradually depleted and considerable effort is expended by parents and caregivers to ensure good nutrition. Wernicke’s encephalopathy has been described in a child undergoing dialysis, who demonstrated the characteristic triad of ophthalmoplegia, encephalopathy, and ataxia [Faris, 1972]. Adult cases usually develop in the wake of prolonged malnutrition [Raskin and Fishman, 1976]. Prompt recognition and treatment are important. Response to intravenous thiamine may confirm the diagnosis [Hung et al., 2001b]. Attention to water-soluble B vitamin supplementation in children requiring dialysis likely reduces the risk for Wernicke’s encephalopathy. This precaution must not be neglected, since there is evidence that many children requiring chronic dialysis do not obtain even the daily recommended dietary allowance for thiamine, as well as vitamin B6 (e.g., pyridoxine) and folic acid [Wang et al., 2002]. Appropriate vitamin supplementation is obviously sensible practice in managing individuals with renal failure.
Pyridoxine-deficiency seizures have been described in a child treated with peritoneal dialysis [Joshioka et al., 1984]. Deficiency of vitamin B12 may, in turn, provoke abnormal methionine metabolism. Hyperhomocystinuria is an important indicator of vitamin B12 deficiency. If found, it is associated with higher risk for pre-eclampsia, neural tube defects in offspring, atherosclerotic arterial disease (large and peripheral vessels), stroke, and venous thrombosis [Herrmann and Knapp, 2002]. Supplementation with B vitamins is routine to avoid these various complications. Dialysis may also result in depletion of serum carnitine; the possible clinical significance of this effect requires more investigation [Bartel et al., 1982]. Chapter 103 reviews the vitamin and other micronutrient deficiency states seen in children.
Progressive Dialysis (Aluminum) Encephalopathy (Dementia)
The issue of aluminum toxicity as a result of the use of oral phosphate binders has been discussed. In addition, there is the concern that aluminum may play a role in the progressive and lethal dementia affecting chronically dialyzed patients with ESRD and manifesting dyspraxia and multifocal seizures at the onset. This entity was first described by Alfrey and associates in 1972. It quickly appeared to assume epidemic proportions and caused considerable consternation in dialysis patients and their physicians [Mahurkar et al., 1973]. Aluminum exposure was the result of utilization of dialysate water purified with aluminum sulfate techniques, and the utilization of aluminum hydroxide as a phosphate binder [Dunea, 2001]. A largely unheeded warning about the potential toxicity of aluminum had been offered in 1970 [Berlyne et al., 1970], but the flurry of research that followed Alfrey’s report of the clinical syndrome greatly enhanced recognition of the public health threat posed by this metal [Verstraeten et al., 2008]. In the early stages, aluminum dementia must be distinguished from each of the many treatable forms of encephalopathy associated with chronic uremia. It is especially important to consider thiamine deficiency, a condition for which all ESRD patients are at risk and which may present as confusion, progressing rapidly to encephalopathy or coma. The chronically poor development and gradual decline of patients with congenital uremic encephalopathy are usually readily distinguishable from the abrupt deterioration of function that occurs early in aluminum dementia. Acquired speech dyspraxia is especially difficult to distinguish from the severe speech and language problems characteristically found in individuals with Finnish-type congenital renal failure.
Intracranial Hemorrhage
The most recent epidemiological study estimated that individuals requiring chronic dialysis for renal failure had an 11-fold greater risk for cerebral hemorrhage and 4-fold greater lifetime risk for subarachnoid hemorrhage, as compared to normal individuals [Iseki et al., 1993]. No recent epidemiological information concerning children could be found. Replacement of generalized with regional anticoagulation in individuals undergoing dialysis has reduced the risk of this serious complication. However, hemodialyzed renal patients are at risk of systemic coagulopathy. Moreover, such individuals may experience marked fluctuations in intracranial pressure during hemodialysis, sometimes associated with dialysis disequilibrium syndrome, whether their renal failure is acute or chronic [Lin et al., 2008]. Subdural hematoma must be considered in renal patients with persistent drowsiness, headache, or vomiting, and particularly in those with persistent focal neurologic signs (typically hemiparesis) or meningismus. Signs and symptoms may fluctuate or progressively worsen. Posterior fossa hemorrhage has been described in the wake of PRES in a heparinized teenager with chronic renal failure [Machinis et al., 2002].
Milder Forms of Encephalopathy
Neuropsychologic studies of adults have consistently documented forms of cortical dysfunction in some patients with chronic renal failure, particularly low verbal IQ. Ability to concentrate may be reduced by even moderate azotemia [Teschan et al., 1983]. Abnormalities of performance IQ, short-term visual and auditory memory, attention span, memory, and speed of decision-making have been documented. The risk for such problems is greatest if ESRD developed in early childhood (particularly during the first year of life), or if renal failure arising in childhood is of very long duration [Crittenden et al., 1985; Fennell et al., 1984; Osberg et al., 1982]. Subtle intellectual and behavioral abnormalities that are responsive to dialysis have been detected in older [Grushkin, 1972], but not all [Fennell et al., 1986], studies. In one small recent study, children with chronic renal disease were found to be at significantly greater risk for grade retention and, to a somewhat lesser extent, for absenteeism, as compared to peers. They were more likely to have mild impairments in intelligence, mathematics, and reading, and were found to satisfy the criteria for the low achievement definition of learning disability [Duquette et al., 2007]. Sensorineural hearing abnormalities may be present in as many as half of patients with ESRD [Bergstrom and Thompson, 1983]. Drugs used for treatment of ESRD and its complications may provoke encephalopathy (see later). Seizures may interfere with school performance.
Evaluation of speech performance requires consideration of the high prevalence of depression, anxiety, and emotional stress in patients with chronic renal failure, and exclusion of the confounding effects of prior developmental dysmaturity and chronic hospitalization [Brickman et al., 1996]. Recent neuropsychological assessment of anxiety and depression in 80 individuals requiring chronic dialysis showed that 52 percent had manifestations of depression in the Beck Depression Inventory (BDI), while 47 percent had evidence for mild anxiety and 49 percent had evidence for moderate or severe anxiety on the Hamilton Anxiety Rating Scale (HARS). Scores on the BDI correlated significantly and directly with degree of abnormality of creatinine, as well as inversely with plasma 25-OH vitamin D level, Mini Mental Status Examination, and interleukin-6 level. Scores on the HARS did not correlate with these variables [Bossola et al., 2010]. A long-term outcome study of individuals whose renal management was initiated before 16 years of age is on-going in Holland. Researchers have reported a comparatively low mean IQ value for their cadre and difficulties in their educational achievements. However, their patients report good overall quality of life despite comorbidities and disabilities. Among the problems they characterize death (occurring in 25 percent) and skeletal abnormalities due to metabolic bone disease were the most common nonrenal disabilities [Groothoff, 2004]. One careful study of 426 chronically dialyzed individuals showed that state anxiety was a more significant predictor of difficulties with concentration and memory than somatic depression symptoms. They concluded that affect and personality make important contributions to memory and concentration [Brickman et al., 1996].
In another study, short-term memory and list-learning correlated with the level of renal dysfunction in 6- to 11-year-old children, and age-appropriate verbal performance correlated with duration of their renal failure. Immediate recall correlated with degree of hypertension. However, there were no other clear correlations of medical parameters with the neuropsychological variables that were assessed [Fennell et al., 1990a]. A 2-year longitudinal study at 6-month intervals of children presenting with what became chronic renal failure evaluated the effect of interventions, including hemodialysis, peritoneal dialysis, or renal transplantation. The investigators documented lower baseline function with regard to verbal ability, memory, visual perception, and especially visual motor skills. With follow-up, patients improved less or, in some instances, deteriorated in function, as compared to age-matched normal controls [Fennell et al., 1990b].
Poor intellectual function should lead to identification and scrupulous correction of metabolic abnormalities. Moderate uremia may result in disturbances ranging from mild encephalopathy to mild chronic delirium or psychosis. In some patients, intellectual dysfunction, deafness, and neuropathy, unresponsive to optimal dialysis, may improve after successful transplantation [Brown et al., 1987; Fennell et al., 1984]. Hypophosphatemia (especially serum phosphate <1.0 mg/dL) is associated with delirium. A combination of aluminum binders, dialysis, and poor diet (often the consequence of anorexia in patients with chronic renal failure) may also provoke mental status changes. Neurologic dysfunction, ranging from confusion to nonketotic hyperosmolar coma, may occur as the result of using dialysate with a high glucose concentration.
Uremic Peripheral Polyneuropathy (Neuropathy of Chronic Renal Failure)
Peripheral neuropathy, first reported more than 40 years ago [Hegstrom et al., 1962], occurs in 65 percent of patients with end-stage kidney disease [Krishnan et al., 2006a]. Asbury and colleagues [1963] provided the earliest detailed description. Somatic and autonomic nerves may be involved [Jedras et al., 2001a]. Risk for neuropathy is not limited to any particular etiologic category of chronic renal failure. As with other neurologic complications, duration and severity of chronic renal failure (e.g., degree of loss of glomerular filtration) are the most important determinants of occurrence and severity of neuropathy [Jurcic et al., 1998]. In patients with congenital or early-childhood onset of chronic renal failure, clinical manifestations of neuropathy have been detected as early as 8 years of age [Oh et al., 1978]. However, few well-documented childhood cases have been reported [Patten, 1984]. Although the term uremic neuropathy is commonly employed, the pathogenesis is complex and remains poorly understood [Krishnan et al., 2005, 2006b]. It may be preferable to refer to the condition as neuropathy of chronic renal failure. Onset of this condition is usually insidious. It is not known how early in the course of the development of neuropathy electrophysiologic abnormalities can be detected.
Subclinical nerve conduction slowing is a not uncommon finding of patients with ESRD [Ackil et al., 1981]. Electrophysiologic abnormalities consistent with neuropathy are ultimately detectable in as many as two-thirds of adults with long-standing chronic renal failure, whether or not dialysis has been initiated [Hassan et al., 2003]. Occasionally, the onset of neuropathy is fulminant, suggesting the possibility of a nonuremic etiology [Asbury et al., 1963; Kondo et al., 1997]. Males are more likely to manifest sensorimotor uremic neuropathy than females, and may develop somatic neuropathy in association with uremia of milder degree and briefer duration, but females are more likely to manifest autonomic neuropathy [Asbury et al., 1963; Jedras et al., 2001b]. A “restless legs” syndrome is among the most common presenting complaints of sensorimotor neuropathy, associated with an unpleasant sensation of “crawling skin” or a “dull ache” of legs that is worse in the evening. Dysesthesias tend to be relieved by leg movement. More convenient and sustained relief may be achieved with clonazepam. Pruritus, which is complained of by as many as two-thirds of patients who have had long-term dialysis for ESRD, may also be a sign of neuropathy in some cases. This is more likely in individuals who also complain of paresthesias, many of whom are found to have neurophysiologic symptoms and additional clinical evidence of neuropathy [Jedras et al., 1998].
Hearing is an important modality to be monitored in individuals with chronic renal disease, particularly young children whose educational achievements, safety, and enjoyment of life may be influenced by dysfunction. Brainstem auditory-evoked response abnormalities observed in individuals with chronic renal failure include progressively more delayed latencies beyond wave I as individuals are followed over time. The most prominent finding in individuals with evidence for peripheral neuropathy may be prolongation of the I–II interpeak latency [Rossini et al., 1984].
Loss of deep tendon reflexes (especially the ankle jerk), diminished vibratory sensation, and weakness of great toe extension, is among the earliest signs of uremic neuropathy. Paradoxical heat sensation, the tendency to identify a low-temperature stimulus as “hot” (as may be seen in a particular form of shellfish intoxication), is also a sensitive early sign of uremic polyneuropathy. This phenomenon, which appears to be an early manifestation of uremic polyneuropathy, was found in 42 percent of such individuals in one series. It appears to correlate not only with the degree of cold hypoesthesia, but also very significantly with the serum creatinine level [Yosipovitch et al., 1995]. Thermal discrimination threshold, as well as vibration discrimination threshold testing, has been the subject of at least one small study in children with end-stage renal failure, but the results were inconclusive [de Beaufort et al., 1989]. As with other neuropathic forms of weakness, distal wasting of muscle is an important clinical sign that distinguishes neuropathic from myopathic causes of weakness (which may occur in chronic renal failure). Early in the course of illness it may be difficult to discern, either because wasting may be masked by obesity (due to inactivity, excessive caloric intake, or steroid use) or by excessive dependent fluid retention (due to inactivity, fluid shifts, or autonomic dysfunction). Fully developed uremic neuropathy is a distal, symmetric polyneuropathy that involves both sensory and motor modalities in a length-dependent fashion. The greatest abnormality is detected in functions subserved by large, long, peripheral nerve fibers. The legs are usually more severely affected than the arms [Nielsen, 1971a, b]. In most patients, uremic neuropathy so closely resembles nutritional, diabetic, or alcoholic neuropathies as to be clinically indistinguishable. Diminished sensitivity to all sensory modalities in a glove-stocking distribution gradually develops. Pressure palsies, to which chronic renal failure/neuropathic renal disease patients are particularly subject, may alter the expected distribution of abnormalities [Bolton et al., 1971].
Other forms of dysesthesia, nocturnal calf cramps, distal weakness, and atrophy may develop and vary considerably in severity [Tyler, 1976]. In adolescents and adults on dialysis for ESRD, sudomotor changes and postural hypotension are common consequences of autonomic neuropathy if it develops [Yildiz et al., 1998]. It is unknown how frequently autonomic neuropathy develops in children [Bach et al., 1979]. Delayed gastric emptying was found in 69 percent of 32 individuals with chronic renal failure in one series. Half of those with abnormal gastric emptying reported no gastrointestinal symptoms, although complaints referable to peripheral or other autonomic nerve dysfunction were often found. Delayed gastric emptying occurred independently of age, sex, duration of disease, blood urea nitrogen (BUN), creatinine, or Helicobacter pylori infection. In this series, treatment with oral cisapride and erythromycin proved beneficial to gastrokinesis [Alimchandani and Pai-dhungat, 1997]. Successful renal transplantation may simultaneously and rapidly reverse both sympathetic and parasympathetic autonomic dysfunction that has developed in adult patients with ESRD [Yildiz et al., 1998]. Hearing loss, common in ESRD, may be the result of uremic axonal neuropathy, although other incompletely cleared endogenous or administered ototoxic substances may contribute to this and other neuropathic abnormalities. Uremic anemia might also contribute to the development of deafness [Shaheen et al., 1997a].
Cardiovascular autonomic neuropathy (CAN) of very high prevalence has been reported in a study from Nigeria [Sanya and Ogunniyi, 2004]. In this group, 65 percent of 60 individuals with chronic nondiabetic renal failure were found to have CAN involving both the parasympathetic and sympathetic divisions. Thus, 39 percent had significant impairment of all heart rate reflex tests, and 28 percent had significant impairment of tests involving the blood pressure response to hand gripping. Clinical evidence for autonomic neuropathy in this group included constipation (60 percent), hyposialism (51 percent), and hypohidrosis (33 percent). Evidence for peripheral neuropathy included sensory loss (50 percent) and numbness (40 percent). Among the tested biochemical parameters, only serum creatinine concentration correlated significantly with the presence of autonomic neuropathy.
Uremic polyneuropathy is initially subclinical, or perhaps is overlooked or misinterpreted in children. Typical electrophysiologic abnormalities include slow motor nerve conduction velocities with reduced distal latencies and compound muscle action potentials of greater degree in the median, peroneal, and tibial nerves than in the ulnar nerves. Widespread reduction of sensory nerve conduction velocities and action potentials is found. Abnormalities of somatosensory-evoked potentials (including N9, N13, and N20 latencies and amplitudes) are commonly encountered, as are findings suggesting central and peripheral axonopathy. “H” reflex testing appears to be one important way in which screening may be undertaken for uremic polyneuropathy. Sensitivity of 44 percent and specificity of 87 percent, with positive predictive value of 66 percent and negative predictive value of 76 percent, have been documented [Mendoza-Guevara et al., 1997]. Abnormal leg F-waves, foot vibration detection thresholds, and sural nerve sensory action potential amplitude are among the most sensitive diagnostic tests for uremic neuropathy [Hassan et al., 2003; Jurcic et al., 1998; Makkar and Kochar, 1994]. If available, Von Frey hairs are excellent devices for assessment of peripheral nerve dysfunction. Quantitative assessment of vibratory sensation with a large tuning fork or especially a vibrometer (Somedic AB, Sweden) may be as sensitive as nerve conduction velocity testing in diagnosing uremic neuropathy [Hilz et al., 1995].
Electrophysiologic evidence for phrenic nerve dysfunction is found in many patients with ESRD and can be predicted by the prolonged peroneal nerve conduction velocities, as was first pointed out in 1995 [Zifko et al., 1995]. Gender differences do not exist for electrophysiologic manifestations of parasympathetic (e.g., electrocardiographic RR interval variation) autonomic testing, although males more frequently manifest abnormal sympathetic skin responses [Jedras et al., 1998, 2001]. Changes found on biopsy are often more severe than anticipated on the basis of the conduction velocity results [Jennekens et al., 1971]. Pathologic features of uremic neuropathy are similar to those seen in other nutritional or toxic neuropathies, and include primary axonopathy with secondary segmental demyelination and remyelination, all emphasized in distal portions of large, long nerve trunks. Muscle biopsy may indicate loss of type 2 fibers [Dyck et al., 1971; Savazzi et al., 1980].
The mechanisms of nerve injury in association with end-stage kidney disease remain incompletely understood. They are not related to urea or creatinine concentrations and, except for “burning feet,” do not involve deficiencies of vitamins or magnesium. Failure of certain energy-dependent axonal/ perikaryonal functions, including ion pumps, axoplasmic transport, and neurofilament synthesis, have been alleged as causes of axonopathy [Dyck et al., 1971; Nielsen, 1973]. Because “middle molecules” are removed more efficiently by peritoneal dialysis and because peripheral neuropathy is less common in peritoneal dialysis than in hemodialysis, deleterious effects of these compounds have been implicated. Sugar alcohols that accumulate in chronic renal failure (e.g., myoinositol) may also play a role [Oh et al., 1978]. Diminished occurrence of neuropathy in children managed without aluminum salt exposure suggests that aluminum may have played a role in uremic neuropathy [Elzouki et al., 1994]. The membrane depolarization in individuals with ESRD and neuropathy is manifested by reduction in threshold electrotonus, superexcitability, and increased refractoriness to stimulation. The chronic depolarization of axons has been ascribed to hypokalemia, although it has been suggested that abnormality of the axonal membrane Na+/K+ pump may account for neuropathy in end-stage kidney disease. Recent investigation has supported that hypothesis [Krishnan et al., 2005, 2006a]. Nerve stimulation under ischemic conditions has provided results suggesting that the hyperkalemia hypothesis may not entirely explain the dysfunction, but that some other dialyzable factor may play a role in the axonal dysfunction, particularly H+ ions that may block Na+ ion conductance [Krishnan et al., 2006b].
After renal transplantation, some patients develop neuropathy as a manifestation of graft-versus-host disease [Kondo et al., 1997]. Burning dysesthesia of the feet was formerly more common than at present and was likely due to dialysis-induced depletion of thiamine [Bolton, 1980]. Some patients with ESRD develop combined system degeneration owing to vitamin B12 deficiency [Kondo et al., 1997]. With vitamin B supplementation, these latter two causes of neuropathy have become rare. Many patients with uremic neuropathy become stable or slowly improve with long-term hemodialysis, although little, if any, improvement is seen after a single dialysis pass [Laaksonen et al., 2002]. Mild neuropathy may remit, but severe neuropathy seldom does. It is possible that increased hours of dialysis or initiation of peritoneal dialysis may provide benefit in some severe cases [el Aklouk et al., 2004]. Worsening of electrophysiologic but not clinical manifestations of neuropathy may be detected in patients who have had more than 10 years of hemodialysis [Jurcic et al., 1998].
Successful renal transplantation usually, but not invariably, leads to complete amelioration of neuropathy in 6–12 months, even in patients with severe neuropathy [Hodson, 1978; Nielsen, 1974a]. Improvement of motor conduction velocity can be documented within days [Oh et al., 1978] or months [Nielsen, 1974b] of transplantation. Sympathetic and parasympathetic autonomic dysfunctions remit fairly promptly after successful transplantation [Yildiz et al., 1998]. Femoral neuropathy is a rare complication of the transplant surgery itself [Probst et al., 1982; Yazbeck et al., 1985]. The potential ameliorative effects of erythropoietin administration are under investigation [Hassan et al., 2003].
It is noteworthy that, while renal failure may secondarily produce autonomic dysfunction, the reverse sequence may occur. The neurodevelopmental disorder, familial dysautonomia (FD), a condition with numerous and protean manifestations, may produce renal dysfunction as a consequence of cardiovascular lability with supine hypertension and orthostatic hypotension. FD also is associated with chronic volume depletion. By age 25, nearly half of individuals with FD have developed an advanced stage of chronic renal disease. Dialysis for these individuals is associated with greater than usual complications due to dialysis and poorer outcome as a result of that intervention. However, renal transplantation has been associated with good functional graft survival for at least 24 months, as well as associated symptomatic and functional improvements, including lower supine blood pressure and increased response to antihypertensive drugs [Rekhtman et al., 2010].
Uremic Myopathy (Myopathy of Chronic Renal Failure)
Uremic myopathy, not easily distinguished from other causes of weakness in individuals with uremic conditions, was first described in 1967 [Serratrice et al., 1967]. The prevalence of muscle weakness in chronically dialyzed individuals is estimated to be approximately 50 percent [Clyne, 1996]. The prevalence is probably higher in adults than children. Despite considerable subsequent attention to this common consequence of ESRD, the pathogenesis is still incompletely understood, and the definition and diagnostic features of the term “uremic myopathy” remain somewhat controversial. Diagnosis of uremic myopathy is often made on the basis of loss of endurance or ability for muscular exercise without muscle physiological testing or biopsy. Physical examination (excepting evidence of proximal weakness and fatigability), muscle enzymes, and electromyography tend to be normal in individuals bearing the diagnosis of uremic myopathy. If muscle biopsy is abnormal, it usually shows only nonspecific fiber atrophy [Campistol, 2002].
Weakness is a common and an important source of morbidity in patients with chronic renal failure, especially those on long-term dialysis. The limitations that weakness may place on normal activities may produce one of the most significant negative impacts of chronic renal disease on quality of life. Untoward weight gain from a variety of causes may occur in renal patients and produce a vicious cycle of weakness-engendered inactivity, weight gain, and weight-related exacerbation of weakness. The effects of this cycle and its associated rate of functional decline may be worsened by mood disturbance or by such frequently encountered intermittent causes of exacerbation of muscular weakness as hypokalemia. Anemia, a common problem in dialyzed individuals, may contribute to muscular weakness, but it does not appear that clinically significant weakness is entirely correctable by blood transfusion [Painter and Moore, 1994]. In individuals with chronic advanced renal failure or ESRD, uremic neuropathy, uremic osteodystrophy, or corticosteroids may also contribute to weakness. Corticosteroid myopathy tends to have a much more acute onset than uremic myopathy. The particularly abrupt and severe onset of so-called acute care myopathy may occur in patients with chronic renal failure. The wide variety of other conditions that may cause acute weakness must also be considered in patients with chronic renal disease with rapidly worsening weakness, including toxic, infectious, or inflammatory diseases of muscle [Berretta et al., 1986].
Although chronic and progressive muscular weakness may, in part, be the secondary consequence of “uremic” neuropathy (which has already been considered), neuropathy is an inadequate explanation for the changes that are found in muscle. There is evidence for contributions of vasculopathy, and furthermore, there is evidence of primary disease of muscle [do Prado et al., 1998]. Uremic vasculopathy is another cause of secondary myopathy of smooth or striated muscles. Vascular myopathy is a necrotic process that has been ascribed to severe hyperparathyroidism with calcification of blood vessels, rather than representing a consequence of autonomic neuropathy. This process may result in impaired muscle capillary oxygen transfer [Bardin, 2003]. Uremic myopathy is a particularly striking condition in children with chronic renal failure. The changes observed on muscle biopsy include atrophy, type grouping, lipidosis, glycogen depletion, and mitochondrial proliferation [do Prado et al., 1998]. These changes clearly indicate the effects of multiple causes, some of which may be primary to the muscle itself. As with many other myopathic conditions, proximal leg weakness is the predominant finding of uremic vasculopathy. Secondary hyperparathyroidism and the associated hyperphosphatemia contribute to this vascular calcification, which may involve the coronary arteries and produce coronary vascular disease, the “silent killer” of uremic patients. It has been suggested that excessive use of calcium-containing phosphate binders may increase the likelihood of uremic vasculopathy [Bardin, 2003]. Utilization of calcium-free and (for reasons noted earlier) aluminum-free phosphate binders is likely an important advance in the avoidance, not only of renal osteodystrophy, but also of uremic vascular myopathy. Caution may need to be exercised in the use of vitamin D derivatives, as well, because they may enhance hypercalcemia [Bardin, 2003].
Cardiomyopathy may be suspected in uremic individuals who demonstrate reduced cardiochronotropic response to exercise. It must be remembered that cardiovascular dysfunction with cardiac failure and ischemic heart disease, with or without associated neurological complications such as stroke, represent the leading causes of death (40 percent of deaths in chronically dialyzed individuals in the United States) and very important causes of disability in individuals with ESRD [Masry and Smogorzewski, 1996]. These risks are not the result of age-related risk for cardiovascular disease. They are risks sustained by young, as well as much older, patients with ESRD. It remains unclear as to what interventions may ameliorate risk of uremic myopathy, as there are few data. Successful renal transplantation, for obvious reasons, is the most effective intervention. Avoidance of secondary hyperparathyroidism and optimization of the approach to dialysis appear to be of particular importance. Some individuals may benefit from carnitine supplementation. Improvement of nutritional status, correction of anemia, and aerobic exercise training may be beneficial [Campistol, 2002; Ahmad et al., 1990]. Reviews of uremic myopathy are available [Bardin, 2003; Campistol, 2002].
Complications of Transplantation
The quality of life, including certain aspects of neurologic function, of patients with ESRD is generally improved after transplantation. Dialysis-associated complications are avoided, and neuropathy usually improves. Higher cortical functions may also improve, including memory, concentration, vigilance, and even intelligence [Fennell et al., 1986; Rasbury et al., 1983]. Transplantation improves head growth and psychomotor development of some children with ESRD [Kohaut et al., 1985; So et al., 1987]. Survival has improved with donor-related but not cadaver transplantation [Vollmer et al., 1983]. Transplantation is not helpful in some diseases that affect the nervous system and the kidney, such as Fabry’s disease or oxalosis. Two major forms of encephalopathy (congenital uremic encephalopathy and progressive dialysis encephalopathy), once well established, do not improve after transplantation [Fennell and Rasbury, 1980]. For reasons noted earlier, the prevalence of progressive dialysis encephalopathy has been sharply reduced. It has not been clear why patients with congenital nephroses exhibit poor development, although emerging data suggest that ischemic brain injury may play a role and that transplantation may reduce the risk for this complication.
A recent study considered 33 children aged 6–11, most of whom had Finnish-type congenital nephrosis, who underwent prior successful transplantation for ESRD before 5 years of age [Valanne et al., 2004]. It was found that more than half of these children had brain-imaging evidence for cerebrovascular border zone ischemia, whereas a smaller number had evidence for major arterial territory infarctions. It appeared that the longer the latency to transplantation for individuals with severe congenital nephrosis, the more likely that they would manifest changes suggesting brain ischemia. Clinical histories of hemodynamic crises were documented in approximately 40 percent of these cases, and within the limits of the study, there was no clear evidence that prematurity, perinatal complications, or sepsis accounted for the imaging abnormalities. Transplantation entails risk for a particular set of neurologic complications. These complications can be divided into those related to graft failure and those related to immunosuppression. Immunosuppressive complications can be divided further into those related to the immunosuppressed state (in combination with chronic antigenic stimulation by the graft) and those related to immunosuppressive drugs [Ram Prasad et al., 1987].
Graft Failure or Rejection
A characteristic rejection encephalopathy with seizures occurs in children [Bates et al., 1986]. Rejection encephalopathy is clinically indistinguishable from hypertensive encephalopathy [Gross et al., 1982]. It is always important to check serum magnesium levels in patients with a recent or long-term kidney graft who manifest seizures because magnesium stores may be low in the pretransplantation epoch, and after transplantation tubular reabsorption of magnesium may initially be inadequate, despite maintenance of adequate glomerular filtration rate [Heering et al., 1996].
Infection
Infection is uncommon during the first month after transplantation. There is no evidence of difference in infection risk with immunosuppression due to either cyclosporine or tacrolimus [Woo et al., 1997]. When early infection does occur, it is usually fulminant bacterial infection with Staphylococcus aureus or by Gram-negative organisms. After the first month, subacute and chronic meningoencephalitides or abscesses are more likely to develop. The pathogens are usually opportunistic organisms, such as Listeria, Toxoplasma, Cryptococcus, or Aspergillus. Infection with pneumococci, mycobacteria, Pneumocystis, Nocardia, Histoplasma, Candida, or Mucor occurs less commonly [Barmeir et al., 1981; Cohen and Raps, 1995; Hodson et al., 1978; Rifkind et al., 1967; Rubin et al., 1981; Tilney et al., 1982]. Of these, the agents that may present late (6 months or more after transplantation) tend to be Nocardia or Toxoplasma.
Listeria and Toxoplasma gondii are among the most common causes of meningoencephalitis in transplant recipients. Fever is not necessarily a prominent element in the presentation of infection with these agents. Listeria should be suspected if profound CSF monocytosis is found [Holden et al., 1980; Lechtenberg et al., 1979]. Toxoplasma infection may produce myocardial involvement, and clinical features that closely resemble systemic cytomegalovirus infection [Schmidt et al., 1995]. Brain abscess, which develops in slightly more than 1 percent of kidney transplant patients, is most often caused by Nocardia but may also be due to infection with Aspergillus or Listeria [Lechtenberg et al., 1979; Rubin et al., 1981]. Characteristic febrile pulmonary involvement may distinguish these and other opportunistic agents (e.g., Gemella, Ochroconis gallopavum) that may cause brain abscess from tumor [Murray et al., 1975; Rifkind et al., 1967; Selby et al., 1997; Wang et al., 2003].
Disseminated histoplasmosis may present in a myriad of ways, particularly as mass lesions of the brain or spinal cord. CSF may be normal, and, as with other fungal infections, biopsy may be necessary to confirm the diagnosis [Livas et al., 1995]. Cryptococcal or candidal septic-metastatic mycotic encephalitis may occur [Schwechheimer and Hashemian, 1995]. Cerebral or rhinocerebral aspergilloma has had a very poor outlook [Cuccia et al., 2000], but with early diagnosis the combination of surgical removal and aggressive antifungal therapy is occasionally curative [Mrowka et al., 1997]. Cerebral cysticercosis produces ring-enhancing lesions in transplant recipients, and should be considered in the southwestern United States and in many developing countries, as well as in migrants from such endemic areas [Gordillo-Paniagua et al., 1987]. These various opportunistic agents carry a mortality of 46–86 percent. They are often difficult to diagnose, with brain abscess presenting in many instances as personality change or withdrawal. Given the gravity of these infectious conditions, early biopsy of brain lesions should be considered. Treatment usually involves discontinuation of immunosuppression and reinstitution of dialysis [Selby et al., 1997; Wang et al., 2003].
Disseminated infection with rapidly growing mycobacteria is a rare condition, and one that may occur in kidney transplant recipients, as well as individuals with chronic renal failure who have not received a kidney transplant with associated immunosuppression. The condition is also seen in individuals with collagen vascular disease. It initially involves skin. In these various categories, 90 percent survival has been documented if appropriate antimicrobial therapy is provided. A second at-risk group includes individuals with cell-mediated immunodeficiency, lymphoma, or leukemia. In that group, survival is only 10 percent, despite appropriate antimicrobial treatment [Ingram et al., 1993].
Until recently, the more common viral pathogens have included Epstein–Barr, herpes simplex, and varicella zoster viruses [Peterson and Ferguson, 1984]. The risk for cytomegalovirus infection is increased by both cyclosporine and tacrolimus [Woo et al., 1997]. Epstein–Barr virus may cause particularly malignant lymphoproliferative mononucleosis with encephalopathy and can lead to fatal multisystem failure. Acyclovir treatment with termination of immunosuppression may be life-saving. Cytomegalovirus has been associated with systemic infection, encephalitis, retinitis, polyneuropathy, transverse myelitis, and graft loss [Bale et al., 1980; Chow, 1989; Spitzer et al., 1987].
Hepatitis C virus not uncommonly infects dialyzed patients with ESRD prior to transplantation. In such preinfected patients, few observable effects are noted either before or after transplantation with immunosuppression. However, infection with hepatitis C virus acquired during or after transplantation may provoke, with unusual rapidity, a fulminant hepatitis with or without cirrhosis. Hepatic encephalopathy develops in as many as half of these cases. Discontinuation of azathioprine, as well as cyclosporine and prednisolone in some cases, may be required to improve the ascites, jaundice, and encephalopathy. In some instances, discontinuation may be tolerated without change in graft function [Ok, 1998].
Progressive multifocal leukoencephalopathy and spongiform encephalopathy have been described in adult transplant recipients but not in children [ZuRhein and Varakis, 1974]. Pneumocystis is the most common protozoal cause of CNS infection after transplantation. Other rare pathogens include Leishmania, Strongyloides, Sporothrix, and Schistosoma [Gullberg et al., 1987; Tsanaclis and de Morais, 1986]. Tuberculosis is always a consideration, especially when no other pathogen is identified. Evaluation of CSF should always be carefully considered in transplant recipients with otherwise unexplained lethargy.
Tumor
Renal transplant recipients have a 1.6–24 percent risk for malignancy, risk that may be 10-fold greater than the normal population [Tyler and Tyler, 1984; Groothof, 2004]. Skin cancer (Kaposi’s sarcoma or malignant melanoma) and non-Hodgkin’s malignant lymphoma have been the most common forms of cancer. Evidence for graft-related transmission of Kaposi’s sarcoma has been reported from Saudi Arabia. The investigators found that 43 percent of 270 kidney recipients had evidence of transmitted cancers, including 9 instances where cancer was removed from renal allografts immediately prior to transplantation [Shaheen, 1997b]. Lymphoproliferative disorders are far more common in children than in adults who have received renal allografts, and constitute the majority of neoplasms for which these children are at risk [Tyler and Tyler, 1984]. The risk for reticulum cell sarcoma is increased 35-fold by transplantation. Any of these forms of malignancy may involve the CNS. The risk for CNS glioma is also markedly increased after renal transplantation. The occurrence of these tumors may be related to reduced immune surveillance, chronic graft-related antigenic stimulation, oncogenic viruses (e.g., Epstein–Barr virus), or oncogenic effects of immunosuppressive drugs. Cyclosporine, azathioprine, and prednisone all appear to increase the risk of lymphoma [van Diemen-Steenvoorde et al., 1986; Wilkinson et al., 1989].
In a high percentage of children undergoing transplantation who develop lymphoma, the neoplasm remains confined to the CNS. However, it is very rapidly progressive and poorly responsive to standard therapy for non-Hodgkin’s lymphoma or acyclovir. Reduction or cessation of immunosuppression may be beneficial in some lymphoproliferative cases, but in most instances even this makes little difference to the grim outlook for this condition [Dean et al., 1997; Mirra et al., 1981]. Diagnosis may be difficult because changes observed on scans may resemble those produced by abscess or by such drugs as asparaginase or PEG-l-asparaginase [Bushara and Rust, 1997]. Persistent space-occupying lesions are more likely to be tumor than opportunistic abscess in patients without pulmonary infection or fever. Thrombotic changes induced by such compounds as asparaginase are transient and do not enhance with administration of a contrast agent. In some cases, tumors and abscesses coexist and biopsy is frequently indicated. Precious stereotaxic biopsy material is best analyzed with a combination of immunohistochemistry and polymerase chain reaction. Benign polyclonal immune cell infiltrates may obscure tiny clones of malignant cells, unless great care is taken in analyzing the specimen [Dean et al., 1997].
Stroke
Massive cerebral hemorrhages have been reported after renal transplantation [Schwechheimer and Hashemian, 1995]. The risk for vascular calcification in brain and in heart, the “silent killer” of adult uremic patients, is likely influenced by the complex interactions of hyperparathyroidism, hyperphosphatemia, osteodystrophy, and use of calcium-containing phosphate binders and of vitamin D derivatives [Bardin, 2003].
Drugs
Drug-related complications include hypertension, immunosuppression, oncogenesis, and direct neurotoxicity. Hypertension severe enough to lead to hypertensive encephalopathy may result from corticosteroid or cyclosporine therapy. This complication usually occurs shortly after transplantation; acute graft rejection or renal artery thrombosis must be excluded. Immunosuppressive and oncogenic effects of drugs have already been considered. Cyclosporine, perhaps because it has been in use the longest, is the calcineurin inhibitor most commonly cited as producing neurologic side effects, including paresthesias, neuralgia, peripheral neuropathy, ataxia, tremor, stupor, coma, confusion, insomnia, psychosis, hallucinations, sympathetic overactivation, headaches, or seizures [Arns, 1994; Peces et al., 1996]. One or more of these neurologic side effects is experienced by 10–38 percent of patients who receive cyclosporine [Beckstein, 2000]. In most instances, the side effects disappear with dose reduction. The association of cyclosporine with reversible posterior leukoencephalopathy-associated seizures, stupor, and other findings has been considered in a previous section. The substrate for encephalopathy may include cyclosporine-induced vascular endothelial injury [Teshima et al., 1996].
There is evidence that tacrolimus, a more potent immunosuppressant than cyclosporine, may also have an even greater tendency to engender neurotoxicities of the same variety as that associated with cyclosporine use [Parvex et al., 2001; Primavera et al., 2001]. Either cyclosporine or tacrolimus may increase the risk of seizures or make it more difficult to control epilepsy in renal transplant recipients. Tacrolimus has been associated with a post-transplantation encephalopathy that includes MRI-discernible changes in gray and white matter. This syndrome may subside without discontinuation of tacrolimus. A similar condition arose with sirolimus. It is not as yet known exactly what role the various drugs employed to prevent rejection of an implanted kidney play in these peculiar syndromes [Parvex et al., 2001].
Enzyme-inducing antiepileptic drugs may reduce expected serum levels of calcineurin-inhibiting immunosuppressive drugs. Corticosteroids, such as methylprednisolone, employed for graft-versus-host disease prophylaxis may produce headache, psychosis, bone demineralization, or spinal cord compression owing to extradural fat accumulation. Corticosteroids may interfere with myelination of the early developing brain [Polinsky et al., 1987]. Tacrolimus, an inhibitor of cytokine and T-cell function, may provoke tremor, headache, hyperkalemia, insomnia, confusion, lethargy, neuropathy, or hypertension.
Administration of the CD3 monoclonal antibody, orthoclone OKT3, to prevent renal allograft rejection may variously provoke headache, fever, vomiting, a flulike syndrome, hypotension, seizure, or aseptic meningitis in as many as one-third of patients. These changes may be severe and include obtundation or coma. Prompt investigation should exclude such alternative causes as CNS infection [Beaman et al., 1985; Capone and Cohen, 1991; Fernandez et al., 1993; Morris and Low, 1999; Shihab et al., 1993a]. OKT3-related encephalopathy has been associated with a cytokine release syndrome that involves elevation of concentrations of several CSF cytokines, including tumor necrosis factor and interleukin-6. Cerebral infarction may occur. Brain edema may develop and lead to brain herniation and death [Agarwal et al., 1993; Reiss et al., 1993; Shihab et al., 1993a, b]. OKT3 may produce a state of akinetic mutism [Pittock et al., 2003], transient hemiparesis [Osterman et al., 1993], or blindness or optic disc swelling with abducens palsies due to increased intracranial pressure [Strominger et al., 1995].
Diseases Affecting Both Kidney and Nervous System
These illnesses can be divided into four general categories:
The inflammatory/vascular illnesses, which are considered first in this section, include thrombotic thrombocytopenic purpura, hemolytic-uremic syndrome, and other thrombocytopenic microangiopathies. In addition, the hepatorenal syndrome, Henoch–Schönlein syndrome, and familial amyloidosis are reviewed. Systemic lupus erythematosus, polyarteritis nodosa, and Wegener’s granulomatosis are examples of other illnesses that produce inflammatory changes in both nervous and renal systems. The details of these illnesses are covered in Chapter 86.
Thrombotic Thrombocytopenic Purpura
Thrombotic thrombocytopenic purpura (TTP) was first described by Moschcowitz, who noted, in a 16-year-old girl, the unusual and fatal combination of fever, hemolytic anemia, renal and cardiac failure, and neurologic dysfunction with widespread hyaline thrombosis of small blood vessels [Moschowitz, 1924]. Adams’ masterful elucidation of the cerebral pathology was added in 1948 [Adams et al., 1948]. Subsequently, many hundreds of cases labeled thrombotic thrombocytopenic purpura have been reported. Formerly, clinical diagnosis required at least two major (thrombocytopenia, Coombs-negative microangiopathic anemia, or neurologic dysfunction) and two minor (fever, renal dysfunction, or circulating thrombi) manifestations [Bukowski, 1982], permitting the diagnosis to be made in the absence of either renal or neurological dysfunction. The absence, until recently, of a specific biomarker for the condition engendered some confusion concerning the boundaries between TTP and a number of other microangiopathic conditions, collectively termed thrombotic microangiopathies. The overlap was especially uncertain concerning the distinction of TTP from hemolytic-uremic syndrome (HUS).
The microangiopathic pathologic similarities of HUS and TTP were recognized from the start. Kidney tropism without prominent neurologic abnormalities, onset before 10 years of age, and absence of associated fever were the common findings that permitted most cases of HUS to be readily distinguished from TTP [Silverstein, 1968]. It became clear, however, that a minority of cases thought to be HUS (because kidney manifestations predominated) presented after 10 years of age, whereas other cases with a predominant phenotype closely resembling TTP occurred in small children.
A recent retrospective pathologic study has demonstrated that TTP and HUS are pathologically distinct entities [Rust 2010a, b]. In cases severe enough to prove fatal, TTP-associated thrombi are platelet-rich and are found in heart, pancreas, kidney, adrenal, and brain, in decreasing order of severity. HUS-associated thrombi are fibrin-/red cell-rich, and tend largely to be confined to the kidney [Hosler et al., 2003]. Other studies have found that TTP thrombi are found in the brains and kidneys of 50–75 percent of individuals with fatal TTP. These thrombi contained von Willebrand factor multimers. It has long been recognized that patients with TTP have ultra-large von Willebrand factor multimers in circulation [Bell et al., 1991; Berkowitz et al., 1979; Chow et al., 1998]. Brain thromboses of TTP occur in small arterioles, capillaries, and venules, and are associated with microinfarction. Small petechial hemorrhages may be widely scattered in gray matter [Adams, 1964]. These advances have also provided diagnostic tests that reliably designate most heritable TTP cases, as well as most individuals with acquired (autoimmune) TTP [Raife, 2003]. On the basis of recent advances, thrombotic microangiopathies have been reclassified, as is shown in Box 102-3. Other, as yet incompletely understood, symptomatic thrombotic microangiopathies with a TTP-like phenotype – conditions that tend to afflict adults and have predominantly neurologic manifestations – are now considered under their own headings in the new classification scheme for thrombotic microangiopathies.
Box 102-3 Thrombotic Microangiopathies










(From MacWhinney JB, et al. Thrombotic thrombocytopenic purpura in childhood. Blood 1962;19:181.)
Signs and symptoms of acute TTP usually evolve quickly and quite noticeably over 7–10 days. Skin purpura is the initial manifestation in more than 90 percent of patients. Fever usually develops early in the course of the illness. Hemorrhage (retinal, choroidal, nasal, gingival, gastrointestinal, and genitourinary), pallor, abdominal pain, arthralgia, or pancreatitis may also develop. Neurologic findings are seen in most cases, and include fatigue, confusion, headache, and varying degrees of dysfunction of vision or language. Significant laboratory findings include microangiopathic hemolytic anemia, thrombocytopenia, elevated lactate dehydrogenase, proteinuria, and microscopic hematuria. CSF chemistry, cell counts, and pressure are usually normal [Adams, 1964]. Other findings commonly associated with disseminated intravascular coagulopathy are not usually found. MRI of brain is often normal. Single-photon emission tomographic images may indicate diminished cerebral blood flow [Fiorani et al., 1995].
As has been suggested, plasma exchange may be a more efficacious treatment than plasma infusion. In a controlled, prospective, double-blind, crossover, multicenter TTP treatment trial [Rock et al., 1991], at least 80 percent survival was found for plasma exchange, compared with 60 percent survival for patients randomized to plasma infusion. A more recent report suggests that the benefits of plasma exchange are related to infusion of larger volumes of plasma or better clearance of toxins, antibodies, multimers, or immune complexes, compared with plasma infusion [Lawlor et al., 1997]. Plasma infusions carry risk for transmission of infections, including hepatitis and possibly human immunodeficiency virus. Most TTP patients have been treated with seven or eight exchanges (requiring blood from 200 or more donors), after which at least 60 percent of patients who had a more severe form of TTP experienced relapse [Bell et al., 1991].
Most cases of TTP are monophasic, but 11–28 percent of patients experience one or more recurrences. In some instances, chronic TTP develops [Bell et al., 1991; Rock et al., 1991; Tsai and Shulman, 2003]. Relapses occur weeks to years after initial remission. For severe or recurrent cases, plasmapheresis and plasma infusion are useful, but the combination of both (plasma exchange) using fresh-frozen, platelet-poor plasma appears to be the most beneficial form of therapy, sometimes in combination with corticosteroids [Moake, 1990]. Plasmapheresis may remove the large von Willebrand factor multimers and circulating antibodies, whereas infused fresh-frozen plasma may contribute ADAMTS13 and circulating antioxidants (e.g., prostacyclin), and may also dilute ADAMTS13-inhibiting IgG.
Hemolytic-Uremic Syndrome
HUS is a Coombs-negative thrombocytopenic microangiopathy, the onset of which is typically in early childhood. Two-thirds of all cases occur in children younger than 3 years of age, and few cases occur after 5 years of age [Gianviti et al., 2003; Rust 2010b]. HUS may occur in the neonate and occasionally occurs in adults, especially in the elderly. Manifestations tend to be much more focal than those of TTP. Table 102-3 provides a classification of causes of HUS. In addition to microangiopathic hemolytic anemia, the characteristic and serious finding is that of acute renal failure, which is usually severe. If there are neurologic manifestations, they are usually mild. As has been noted, however, there is an area of clinical overlap between HUS and TTP. TTP occasionally occurs in neonates, and HUS occasionally occurs in adults, especially the elderly. HUS in the elderly may have a different pathogenesis from childhood cases because the disease of the elderly tends not to respond well to therapies that are effective in childhood cases [Blackall and Marques, 2004; Karlsber et al., 1997].
| Former | Current |
|---|---|
| Classic infantile (D+) | Classic infantile (D+) |
| Postinfectious (D+ or D−) | Postinfectious (D+ only) |
| Familial | D+ familial D− familial H-factor positive subgroup H-factor negative subgroup |
| Immunologic | Sporadic D+ subgroup D− subgroup |
| Secondary | Subdivided into sporadic or familial categories |
| Endocrine | Subdivided into sporadic or familial categories |
Neurologic manifestations of HUS – most commonly, behavioral changes, motor seizures, stroke, and varying degrees of encephalopathy – are seen in 30–40 percent of patients. Blindness, ataxia, hemiparesis, and decerebrate rigidity have also been reported [Kaplan et al., 1971; Martin et al., 1990; Sheth et al., 1986]. The occurrence of neurologic abnormalities predicts a worse outcome with enhanced risk for ESRD or death [Garg et al., 2003]. It is not always clear whether such neurologic changes are the result of cerebral microangiopathy or are secondary to metabolic disturbances and hypertension. MRI of brain may disclose focal areas of infarction with swelling and, in some cases, hemorrhage, especially in such areas as the internal capsule and deep gray nuclei [Jeong et al., 1994]. Children in whom neurologic signs develop are more likely to die or to have residual hypertension or chronic renal dysfunction [Palomeque Rico et al., 1993; Sheth et al., 1986]. Clinical features suggestive of HUS are noted in Box 102-4.









Treatment
Investigations have been undertaken concerning the efficacy of administering preparations containing inert adsorptive surfaces that are capable of binding circulating verocytotoxin, thereby preventing attachment to endothelial surfaces where they can engender injury. SYNSORB-Pk ingestion was among the first approaches tried [Joh, 1997] but appears to have been abandoned. Other preparations are undergoing evaluation [Armstrong et al., 1995].
Improved supportive therapy, including transfusion, dialysis, and careful management of fluids, electrolytes, and hypertension, has reduced mortality from 50 percent half a century ago to what is variously estimated as 0–30 percent mortality, with recent pooled data suggesting roughly 10 percent [Garg et al., 2003; Gianantonio et al., 1973; Kaplan et al., 1976]. Adult mortality is much higher, probably because adult HUS more often occurs as a complication of much more severe systemic illnesses than are encountered in childhood HUS cases. Therapeutic options include anticoagulation, administration of antiplatelet or antioxidant agents, thrombolysis (streptokinase), plasmapheresis/plasma exchange, or infusions of plasma, prostacyclin, or gamma globulin [Bitzan et al., 2010; Palermo et al., 2009; Michael et al., 2009].
None of these various approaches has well-established efficacy (beyond that achieved by excellent supportive care). Plasma manipulations appear to be less beneficial in HUS than in TTP [Misiani et al., 1982; Moake, 1991; Powell et al., 1984]. Trials of gamma globulin are in progress, and preliminary results are promising. Although it is undertaken in some adults with HUS, anticoagulation in childhood cases entails a certain risk in an illness that is frequently complicated by both bleeding and hypertension. Moreover, it does not appear to be beneficial, even when combined with administration of oral antiplatelet agents. It is probably contraindicated [Proesmans et al., 1980]. HUS-associated renal failure usually persists for several weeks. Dialysis is required in 30–50 percent of patients and is indicative of a poorer prognosis [Garg et al., 2003; Martin et al., 1990]. Renal transplantation is necessary in severe HUS, amounting to approximately 25 percent of all childhood cases.
Vasculitic Diseases with Neurologic-Renal Presentations
Extended consideration of the various inflammatory disorders is to be found in Chapters 85, 86, 90 and 95.
Hepatorenal Syndrome
Hepatorenal syndrome is a widely accepted but controversial designation for the functional, potentially reversible renal failure that occurs in patients with various forms of liver failure [Bataller et al., 1998; Van Roey and Moore, 1996]. It is divided into two types, each with established diagnostic criteria [Arroyo et al., 1996]. Type 1 includes patients whose rapidly deteriorating renal function with hyponatremia and hyperkalemia develops in association with acute severe hepatic dysfunction (from various causes) or severe hepatic cirrhosis (chiefly alcoholic). It is usually fulminant and carries a high risk for death. Encephalopathy develops in most type 1 cases. Type 2 includes patients that manifest the combination of less severe liver and renal disease. Encephalopathy is less common in type 2 cases. Some form of hepatorenal syndrome develops in as many as 20 percent of patients who are in their first year of acute or subacute hepatic failure. It occurs in 40 percent of those who have experienced at least 5 years of chronic hepatic failure.
Cases of type 1 hepatorenal syndrome are rare in childhood. Half of all such cases occur in the wake of acute viral hepatitis with hepatic failure. It may also occur after other causes of liver failure (native or graft), particularly if portal hypertension is present and has produced gastrointestinal bleeding [Evans et al., 1995]. Liver necrosis (sometimes centrilobular) and fatty infiltration of the liver may be found [Shida et al., 1996]. Some cases occur after liver transplantation in children who had chronic liver disease due to biliary atresia. One case has been reported in a 3-year-old child with α1-antitrypsin deficiency. This child died with hepatorenal syndrome after developing hemorrhagic shock and encephalopathy, disseminated intravascular coagulopathy, metabolic acidosis, and nonketotic hypoglycemia [Shida et al., 1996]. Severe hepatorenal syndrome may also develop in children with hereditary fructose intolerance [Ali et al., 1993], Wilson’s disease, liver malignancy, or autoimmune hepatitis, after shunting procedures for bleeding varices [Evans et al., 1995], or after administration of medications such as nonsteroidal anti-inflammatory drugs (NSAIDs) or minocycline [Arroyo et al., 1983; Boudreaux et al., 1993]. Spontaneous bacterial peritonitis may provoke the hepatorenal syndrome.
Understanding of the pathophysiology of hepatorenal syndrome remains incomplete, and the available theories are controversial. Renal failure probably occurs as the result of severe renal cortical arterial and arteriolar vasoconstrictive ischemia. Some believe that this is in response to the release of hepatic substances that variously provoke vasoconstriction or vasodilatation. Some believe that vasopressin, renin-angiotensin, or catecholamines may provoke intense selective vasoconstriction with ensuing renal failure [Neuschwander-Tetri, 1994]. Doppler ultrasonography has demonstrated increased renal vascular resistance in as many as 40 percent of patients with nonazotemic liver disease [Maroto et al., 1994; Sacerdoti et al., 1993]. Renal dysfunction subsequently develops in more than half of these at-risk individuals, half of whom in turn develop hepatorenal syndrome [Platt et al., 1994]. An inverse correlation has been observed between plasma-activated cytokine levels and improvement in renal function after treatment of hepatorenal syndrome with liver transplantation [Burke et al., 1993].
In patients who develop encephalopathy, it has been found that the cerebral circulation is also compromised by intense selective cerebral vasoconstriction [Better, 1983]. It is not known why the sustained vasoconstrictive sympathetic response may be so selective for vessels subserving kidney and brain circulation, whereas capacitance vessels in many other vascular beds dilate. Increased renal secretion of regional vascular modulators may enhance the vasoconstriction and produce additional deleterious effects on glomerular capillary ultrafiltration [Van Roey and Moore, 1996]. Systemic hypotension frequently accompanies the onset of hepatorenal syndrome and may be due to the opening of portosystemic shunts with resulting splanchnic bed dilatation, accompanied by blood pooling in that and possibly in other portions of the systemic circulation.
Clinical features of hepatorenal syndrome include ascites, jaundice, and low arterial blood pressure, despite increased plasma volume. Hepatomegaly is usually not present. A pre-existing poor nutritional state is not uncommon. Laboratory findings often include hyponatremia, hyperkalemia, low urinary sodium clearance, low plasma but high urine osmolarity, high plasma renin activity, increased plasma norepinephrine, and moderately increased blood urea nitrogen and creatinine. Patients who develop acute encephalopathy with hepatorenal syndrome, probably due to severe cerebral vasoconstriction, may be found to have extensive symmetric ischemic brain injury suggestive of parasagittal infarction [Shida et al., 1996].
A wide variety of drug and circulating volume treatments aimed at reversing the systemic vasodilatation and renal or cerebral vasoconstriction have failed or resulted in only modest improvement in survival. Misoprostol, a prostaglandin E1 analog, has been touted as a treatment for hepatorenal syndrome, as well as for a wide variety of other toxic or inflammatory forms of hepatic or renal disease [Davies et al., 2001].
The use of systemic vasoconstrictors (terlipressin, ornipressin) with albumin has resulted in recovery of renal function in many patients, or recovery of sufficient degree and duration of function to permit liver transplantation or a hepatic shunt procedure to be performed [Moreau, 2002; Ortega et al., 2002]. Liver transplantation has greatly improved the survival rate [Restuccia et al., 2004]. However, the limited availability of grafts and the hesitancy to use them in the setting of a grave disease associated with so many predisposing medical conditions have limited the usefulness of this option. Transjugular intrahepatic portosystemic shunts have promise in management of hepatorenal syndrome [Angeli, 2004]. Among patients who experience hepatic recovery or have successful liver transplantation, approximately 7 percent develop ESRD [Gonwa et al., 1991].
Amyloidosis
Amyloidoses are divided into the heredofamilial (primary) type and those that constitute the secondary (reactive) group. Primary amyloidoses comprise a heterogeneous collection of conditions, many of which are rare and restricted to particular mutations shared by small isolated communities of individuals [Benson, 2003]. Identification of the specific gene defect underlying a particular familial form of amyloidosis is of importance for selection of therapy, prognostication, and genetic counseling [Benson, 2003]. Reactive amyloidoses are associated with a wide variety of provocative circumstances, most of which are encountered only in adults. These include inflammatory arthritides or vasculitides, dialysis, and myeloma-associated immunoglobulin light chain deposition. Box 102-5 lists selected amyloid-related disorders. Many forms of heredofamilial amyloidosis are chiefly cutaneous or do not involve the neurologic and renal systems. However, progressive nephrosis and neurologic disease (CNS tissues, nerve, or muscle) are among the most common manifestations of either primary or secondary amyloidoses. Cardiac and gastrointestinal abnormalities are also common. Dysfunction in these various organ systems is the consequence of serositis and vasculitis associated with deposition of the insoluble beta-pleated sheet fibrils (low-molecular-weight peptides) that were long ago misnamed amyloid. Arterial and arteriolar wall deposition in affected organ systems is more common than capillary or venous.










Of the numerous amyloid proteins associated with disease in humans, seven produce neurologic disease. Their genetic loci are shown in Table 102-4. As can be seen, most patients present in mid- or late adulthood with dementia or stroke, and many have little or no renal abnormality. Amyloid-β precursor protein may account for some aspects of the progressive dementia seen in Alzheimer’s disease and Down syndrome, although this assertion remains controversial. CNS amyloid deposition in such individuals results in amyloid angiopathy that may produce visual disturbances (small or large, irregular, poorly reactive pupils; internal ophthalmoplegia; blindness), nerve deafness, bland or hemorrhagic cerebral infarction, dementia, seizures, polyneuropathy, weakness, or muscle wasting [Benson, 2002; Revesz, 2003; Rousset et al., 2000; Suhr et al., 2003]. The precursor protein is expressed in kidney and is a low-concentration constituent of normal urine. The concentration of this soluble protein increases in certain forms of renal tubulopathy associated with a variety of metabolic diseases. Autosomal-dominant familial amyloidotic polyneuropathy (type I amyloidosis) is most likely to occur in Portuguese, Spanish (including Majorcan), Swedish, or Japanese kindreds. More than 80 identified missense mutations in the transthyretin gene produce variant transthyretins that account for various disease manifestations [Date et al., 1997; Falk et al., 1997; Uyama et al., 1997].
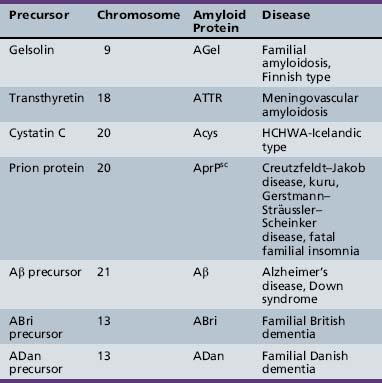
One amyloidosogenic mutation (Val121Ile) is found in about 3 percent of American blacks. This condition may present as lower-extremity polyneuropathy at some point between the second and fourth decades of life. Individuals may develop fatal meningovascular angiopathy associated with early loss of short-term memory and, in the advanced state, with cerebral hemorrhage. Subsequently, hearing loss, autonomic or craniofacial polyneuropathy, ataxia, and pyramidal tract signs may be noted. Individuals with this condition may have abnormalities of kidney, liver, heart, gastrointestinal system, lungs, skin, and ovaries [Benson, 2002; Rousset et al., 2000]. Treatment with early liver transplantation may improve neurologic manifestations, but cardiac and renal function may deteriorate somewhat after liver transplantation [Suhr et al., 2003]. Chronic uremia may induce oxidative endothelial vascular damage that facilitates amyloid deposition and worsens the vasculopathy of various organ systems that this disease promotes.
A Hungarian variety of transthyretin gene mutation tends to be clinically restricted to the nervous system. Severe meningocerebrovascular changes are associated with memory disturbance, psychomotor deterioration, ataxia, hearing loss, migrainous headaches with vomiting and episodic disorientation, tremor, and nystagmus. Motor decline is associated with the development of pyramidal signs. Sleep disturbances and facial tics may be found. Peripheral nerve, heart, and kidney function are usually normal, despite amyloid deposition, and vision remains normal [Garzuly et al., 1996]. Another autosomal-dominant amyloidosis is termed hereditary cerebral (Icelandic type, type VI) amyloidosis. Mutations of codon 68 of cystatin C gene on chromosome 20 result in production of ACys. Affected normotensive young Icelandic adults have presented with hemorrhagic strokes that may recur or cause death. These are due to the particular tendency for the formation of heavy amyloid deposits on small arteries or arterioles of brain, although vessels of the kidney, spleen, lymph nodes, salivary glands, and seminal vesicles may be involved. Individuals who do not develop strokes may experience progressive middle-age onset of dementia [Olafsson et al., 1996].
Finnish-type (type V) amyloidosis is the result of mutations in the chromosome 9 gene that encodes gelsolin, a regulatory protein. This condition also occurs in Danish and Czech kindreds. There is disturbance of amyloid genesis but also of fusin proteolysis. The pathway that is involved with this disturbance is responsible for the production of Pme117-encoded fibrils, which are precursors for the biogenesis of melanosomes [Huff et al., 2003]. Individuals with this condition may have droopy-appearing eyes and protruding lips. Peculiar corneal “lattice” deposits may be seen. Neurologic abnormalities include peripheral or cranial neuropathy and progressive vasculopathy of blood vessels subserving brain, spine, and sensory ganglia. Homozygous Finnish-type amyloidosis due to the ASN187 gelsolin mutation produces severe nephrotic syndrome. This syndrome may progress to ESRD, owing to heavy glomerular deposits of gelsolin-derived amyloid, especially in tubular epithelium.
Among individuals of Middle Eastern ancestry, especially Sephardic Jews and Armenians, as well as North African Jews and others, familial Mediterranean fever is the most important cause of secondary (i.e., AA) amyloidosis. This autosomal-recessive condition results from one of a number of mutations in the MEFV gene [International FMF Consortium, 1997; French FMF Consortium, 1997]. These mutations are common in the Middle East, where disease prevalence may be as high as 1:2600 and gene frequency as high as 1:50, especially in the Near Middle East. At least 30 different mutations of the MEFV gene on chromosome 16p13.3 have been linked to this disease [Aldea et al., 2004]. Typical recurrent manifestations develop between 4 months and 16 years of age, and if untreated, persist throughout life. They include short episodic attacks of fever, abdominal or unilateral chest pain, erysipelas-like erythema, organomegaly, and serositis (pleuritic and arthritic). Without adequate treatment, secondary amyloidosis often develops, especially when there is a family history of amyloidosis. Affected persons are at risk for the development of the most devastating consequence of this condition: amyloidotic renal failure progressing to ESRD and associated neurologic and other complications.
It remains unclear as to what factors, in addition to having one of the MEFV gene mutations, governs risk for and severity of the amyloidotic complication [Yalçinkaya et al., 2000] However, it is well known that the risk for this eventuality is reduced by as much as 95 percent if chronic colchicine therapy is undertaken after early diagnosis [Aldea et al., 2004; Hojberg and Mertz, 1995]. If amyloidosis does develop, the 5-year risk for chronic renal failure ranges from 50 percent (type I amyloidosis) to over 80 percent (type II amyloidosis). Henoch–Schönlein purpura and polyarteritis nodosa may develop, as well as symptomatic thyroid and gastrointestinal amyloid deposition. Neurologic manifestations result either from CNS vasculitis or secondary to chronic renal failure [Kavukcu et al., 1995; Rawashdeh and Majeed, 1996; Saatci et al., 1993, 1997; Tinaztepe et al., 1993].
Another severe form of autosomal-dominant familial secondary amyloidosis has been described in Spain, wherein intermittent bouts of joint pain occur. Progressive AA amyloidosis-associated renal failure may develop and is unresponsive to colchicine. All patients with this condition are heterozygotes for the newly described H4784 MEFV gene mutation. It is currently uncertain whether this condition ought to be classified with familial Mediterranean fever or with the newly described group of inherited autoinflammatory periodic syndromes seen in association with other gene mutations, including TNFRSFIA and CIAS1/PYPAF1/NALPO3 [Aldea et al., 2004]. There are a number of additional secondary or reactive forms of amyloidosis. One that has clinical similarities to Portuguese familial amyloidosis is Muckle–Wells syndrome. Like familial Mediterranean fever, it is an AA amyloidosis. Presentation may be in the second decade with corticosteroid-resistant nephrotic syndrome. Neurologic abnormalities include bilateral inner ear deafness and recurrent urticaria. Other findings are arthralgia, aphthosis, amyloid goiter, and skeletal abnormalities. Skin and joint abnormalities respond to immunosuppressive therapies, including cyclophosphamide [Berthelot et al., 1994; Fuger et al., 1992; Schwarz et al., 1989; Throssell et al., 1996].
Various chronic infectious or inflammatory conditions can provoke secondary amyloidosis. Examples include juvenile rheumatoid arthritis, systemic lupus erythematosus, granulomatous bowel disease, Takayasu’s disease, tuberculosis, leprosy, osteomyelitis, and inadequately treated chronic suppurative infections, such as subacute bacterial endocarditis. Hematuria, proteinuria, abnormal urinary sediment, diminished renal function, or hypertension may indicate the development of renal amyloidosis. However, such manifestations are not uncommonly the result of infectious glomerulonephritis or the administration of nephrotoxic drugs [Herbert et al., 1995; Kavukcu et al., 1995; Sieniawska et al., 1996; Tinaztepe, 1995]. A wide range of neurologic abnormalities may be seen in individuals with one or another of these secondary amyloidoses. Vasculopathy may result in neurologic consequences due to bland or infectious cardiogenic emboli, cerebral amyloid angiopathy, Takayasu’s disease, or hypertensive encephalopathy [Sousa et al., 1993]. Close collaborative investigation and management of such complex patients by pediatric neurologists and nephrologists, rheumatologists, and infectious disease specialists is of great value in arriving at an accurate diagnosis. Decreased urinary excretion of glycosaminoglycans may be a marker for renal involvement in the amyloidoses. This finding is thought to be the result of:
Selective Tubular Dysfunction
Important examples of diseases that produce neurologic dysfunction in association with proximal renal tubular acidosis are listed in Box 102-6. Those associated with distal renal tubular acidosis are listed in Box 102-7. Intense scrutiny is being directed at the molecular genetics and mechanisms of these various conditions, resulting in a rapidly evolving increase in understanding and a rich banquet of clinical and scientific data. Only a brief review can be provided here. Additional information can be obtained through the Online Mendelian Inheritance in Man (OMIM) database.


































Proximal Renal Tubular Acidosis
Detection of the characteristic urinary pattern of elevation of the concentrations of multiple amino acids, glucose, phosphate, bicarbonate, calcium, and protein is an especially convenient method of confirming proximal renal tubular acidosis. Characteristically, urine is often dilute, despite the elevated concentrations of various solutes, owing to a concentrating defect that is secondary to hypokalemia. Additional findings in most cases include stable but a mildly reduced level of serum bicarbonate (15–20 mEq/L) and appropriate urine acidity on an early morning void (pH >5.3) [McSherry, 1981]. Further diagnostic clues include normal anion gap acidosis, hypophosphatemia, and hypomagnesemia. Hypokalemia and bicarbonaturia worsen after administration of alkali. Renal Fanconi’s syndrome may occur as a primary familial disorder that may produce syndromes associated with carnitine wasting due to the failure or inadequacy of the proximal tubular carnitine reabsorption. Such a process occurs in a number of heritable metabolic proximal tubulopathic conditions, and may occur as the result of toxic effects of valproic acid. Some neurologic problems may be worsened by a proximal renal tubular leak. Carnitine loss in infantile renal Fanconi’s syndrome has been associated with poor muscle development and abnormal intramuscular lipid deposition. Hypokalemic muscle weakness is an important potential complication of alkali or thiazide treatment of proximal renal tubular acidosis from any cause. Individuals with inherited hyperkalemic periodic paralysis who have Fanconi’s syndrome may be vulnerable to an attack of their condition, owing to those same interventions.
Various secondary forms of renal Fanconi’s syndrome that may occur in the setting of various heritable metabolic disorders will be considered in this section (see Box 102-6), which also manifest neurologic abnormalities in addition to and not directly dependent on the presence of Fanconi’s syndrome. In most of these metabolic conditions, Fanconi’s syndrome tends to be mild to moderate. In some of these diseases, most commonly nephropathic cystinosis, disease tends to progress to chronic renal failure. Almost all of these heritable metabolic conditions are autosomal-recessive. Exceptions include X-linked recessive Lowe’s syndrome and maternally inherited mitochondropathies. Secondary renal Fanconi’s syndrome may also result from endocrinopathies and intoxications, and in association with fructose 1,2 bisphosphatase deficiency, carnitine palmitoyl transferase deficiency type I, and complex IV mitochondropathies. These various heritable metabolic conditions are considered elsewhere in these volumes and will not be reviewed here. It is important to note the manner in which assessment of renal tubular function may prove quite valuable for diagnostic purposes. Other renal findings of use for diagnosis of metabolic conditions are noted in Box 102-8.
Box 102-8 Renal Findings of Diagnostic Importance in Hereditary Metabolic Encephalopathies




















Nephropathic cystinosis will be considered since it is not included elsewhere. Obviously, any disease that causes severe generalized proximal renal tubular acidosis, including familial Fanconi’s syndrome, may result in neurologic abnormalities when severe disturbances of potassium, glucose, or acid–base balance occur. This is particularly the case when poorly compensated chronic renal failure or ESRD develops. The occurrence of seizures in a patient with proximal renal tubular acidosis may be due to hypocalcemia or hypomagnesemia [Heering et al., 1996].
Nephropathic Cystinosis
Nephropathic cystinosis, caused by a defective lysosomal membrane transport protein, is the most common identifiable cause of renal Fanconi’s syndrome in children. This autosomal-recessive condition occurs almost exclusively in white individuals. The defective gene has been mapped to a 1-cM region of chromosome 17p13. Continued work, including the cloning of the responsible gene and studies of immortalized proximal tubule cells expressing the defect, should provide important information concerning the biology of lysosomal transport proteins [Jean et al., 1996; McDowell et al., 1996; Peters et al., 1997; Racusen et al., 1995; Stec et al., 1996].
Before renal transplantation was available, it was thought that neurologic abnormalities occurred only as consequences of renal dysfunction. With the prolonged survival that renal transplantation affords, it has become clear that the infantile and juvenile forms may be associated with visual, intellectual, and motor abnormalities that result from cystine accumulation in the eye (cornea, conjunctiva, retina) or brain (choroid plexus, cortex). Accumulation in the cornea causes progressive keratopathy. Recurrent corneal erosions may prove troublesome [Elder and Astin, 1994]. Cysteamine supplementation to deplete cystine does not influence the course of corneal keratopathy [Thoene, 1995]. Other neurologic consequences develop at various ages from childhood to adulthood. They may include headache; autonomic abnormalities (heat intolerance, hyperthermia, abnormal sweating); poor vision and deficient visual memory; short, raspy, repetitive speech; tremor; pyramidal or extrapyramidal motor defects; and weakness [Gahl et al., 1988; Jonas et al., 1987; Levine and Paparo, 1982]. Selective impairment of visual processing, such as inability to rotate figures mentally, is a frequent finding, despite the typically normal intelligence and primary sensory function of these patients. Abnormality of tactile recognition with astereognosis has been discerned in some patients. These higher cortical deficits must be considered in the educational planning for children with this disorder. These subtle deficits are the likely basis of some of the school difficulties experienced by children with nephropathic cystinosis. In some instances, the general level of intelligence may be slightly below that of parents or siblings. Intellectual deficits may be static or slowly progressive [Ballantyne et al., 1997; Colah and Trauner, 1997; Scarvie et al., 1996; Williams et al., 1994].
Some patients experience much more severe and strikingly progressive neurologic complications. Cystinosis-related encephalopathy is an entity characterized initially by manifesting cerebellar and pyramidal signs, with ensuing mental deterioration, and then development of pseudobulbar or bulbar palsy with a prominent swallowing disorder. Adults with nephropathic cystinosis may have strokelike episodes with coma and hemiplegia. In either of these clinical groupings, MRI abnormalities may be discerned [Broyer et al., 1996; Van Lierde et al., 1994]. These abnormalities correspond to demonstrable pathologic changes within the nervous system, which include nonobstructive hydrocephalus; calcification of the basal ganglia, periventricular zone, and internal capsule; and demyelination of the internal capsule and brachium pontis. Evidence suggests that cysteamine may reverse cystinosis-related encephalopathy, improve the radiologic appearance of brain, and prevent paroxysmal episodes [Broyer et al., 1996].
As has been noted in the section on uremic myopathy, approximately one-quarter of patients with long-standing nephropathic cystinosis develop distal lipid inclusion myopathy, and perhaps all such patients have subclinical electrophysiologic abnormalities. This result may be the direct effect of cystine toxicity, although carnitine deficiency and other potential causes may also contribute. It remains unclear whether replenishment of muscle carnitine with oral supplementation is beneficial [Gahl et al., 1993]. Patients with cystinosis-related myopathy develop weakness and wasting of small hand muscles, facial weakness, and muscular dysphagia. However, they retain sensation and tendon reflexes. Distal motor unit potentials may have reduced amplitude and duration, and biopsies may indicate a vacuolar myopathy of lysosomal origin [Charnas et al., 1994]. Cystine depletion with cysteamine has been advocated [Vester et al., 2000]. One case of anesthetic-induced malignant hyperthermia has been reported in a child with cystinosis, possibly related to myopathic changes [Purday et al., 1995]. Additional heritable diseases that may result in a combination of neurologic and renal manifestations are listed in Table 102-5.
Table 102-5 Syndromes with Kidney Malformation and Neurologic Disease
| Syndrome (Inheritance) | Kidney | Neurologic |
|---|---|---|
| Bardet–Biedl (AR) | Congenital glomerulonephritis Hypertension |
Mental retardation Visual abnormalities |
| Beckwith/Wiedemann (Sp) | Renal dysplasia RT |
Mental retardation |
| Cat’s eye | Renal agenesis | Mental retardation Visual abnormalities |
| Cockayne’s (AR) | Renal dysplasia Hypertension |
Mental retardation Deafness Ataxia Peripheral neuropathy |
| Fanconi’s pancytopenia (AR) | Renal hypoplasia Renal dysplasia |
Mental retardation Cranial neuropathy Deafness |
| Fraser’s (AR) | Renal agenesis | Mental retardation |
| Johanson–Blizzard | Renal dysplasia Hydronephrosis |
Mental retardation Deafness |
| Joubert’s | Renal cysts | Cerebellar dysplasia |
| Klippel–Feil (Sp) | Renal dysplasia | Cranial neuropathy Neural tubule defects Cervical dysplasia |
| Meckel–Gruber (AR) | Renal dysplasia | Neural tubule defects CNS migrational abnormalities |
| Melnick–Fraser (AD) | Renal hypoplasia Renal dysplasia |
Deafness |
| MURCS | Renal agenesis | Cervical dysplasia Deafness |
| Orofaciodigital I | Polycystic kidneys | Mental retardation CNS migrational abnormalities Hydrocephalus Encephalopathy |
| Pallister–Hall (Sp) | Renal dysplasia | Tumors CNS migrational abnormalities NE |
| Partial trisomy 10S | Renal dysplasia | Mental retardation CNS migrational abnormalities |
| Rubinstein–Taybi | Renal dysplasia | Mental retardation |
| Schinzel–Giedion | Hydronephrosis | Mental retardation Deafness Encephalopathy |
| Short-rib polydactyly II | Renal dysplasia Polycystic kidneys |
Cervical dysplasia CNS migrational abnormalities |
| Townes’ | Renal hypoplasia Hydronephrosis |
Deafness |
| Triploidy/mixoploidy | Renal dysplasia Polycystic kidneys |
Mental retardation CNS migrational abnormalities Neural tubule defects Hydrocephalus |
| Trisomy 9 mosaic | Deafness | Mental retardation CNS migrational abnormalities Neural tubule defects |
| Trisomy 18 | Hydronephrosis Polycystic kidneys |
Mental retardation CNS migrational abnormalities Neural tubule defects Hydrocephalus |
| Tuberous sclerosis (AD) | Tumors | Tumors Mental retardation Encephalopathy |
| Turner’s | Renal dysplasia Hypertension |
Mental retardation Deafness |
| Zellweger’s (AR) | Renal cysts | Mental retardation CNS migrational abnormalities |
AD, autosomal-dominant; AR, autosomal-recessive; CNS, central nervous system; MURCS, Müllerian duct renal and cervical vertebral defects; Sp, sporadic.

