Chapter 5 Impact of Age on Pharmacology
Fetus
A teratogen is defined as any agent that can cause malformations in a developing fetus.

 Size of drug
Size of drug

The risk of a drug causing harm to the fetus is categorized using the system in Table 5-1, which is largely based on the evidence (or, most commonly, lack of evidence) of harm.
 Note that relatively few drugs are at the extreme ends of the spectrum (either safe or absolutely contraindicated); this is typically because of a lack of good evidence. It is understandably difficult to conduct controlled trials in this population.
Note that relatively few drugs are at the extreme ends of the spectrum (either safe or absolutely contraindicated); this is typically because of a lack of good evidence. It is understandably difficult to conduct controlled trials in this population.

TABLE 5-1 Risk Categories and Descriptions for Use of Drugs in Pregnancy
| Risk Category | Description |
|---|---|
| A | Controlled studies in humans fail to demonstrate risk to the fetus in the first trimester or later trimesters, and the possibility of fetal harm appears remote. |
| B | Either animal reproduction studies have not demonstrated a fetal risk but there are no controlled studies in pregnant women, or animal reproduction studies have shown an adverse effect (other than a decrease in fertility) that was not confirmed in controlled studies in women in the first trimester (and there is no evidence of risk in later trimesters). |
| C | Either studies in animals have revealed adverse effects on the fetus (teratogenic or embryocidal or other) and there are no controlled studies in women, or studies in women and animals are not available. Drugs should be given only if the potential benefit justifies the potential risk to the fetus. |
| D | There is positive evidence of human fetal risk, but the benefits in pregnant women may be acceptable despite the risk (e.g., if the drug is needed in a life-threatening situation or for a serious disease for which safer drugs cannot be used or are ineffective). |
| X | Studies in animals or human beings have demonstrated fetal abnormalities or there is evidence of fetal risk based on human experience or both, and the risk of the use of the drug in pregnant women clearly outweighs any possible benefit. The drug is contraindicated in women who are or may become pregnant. |
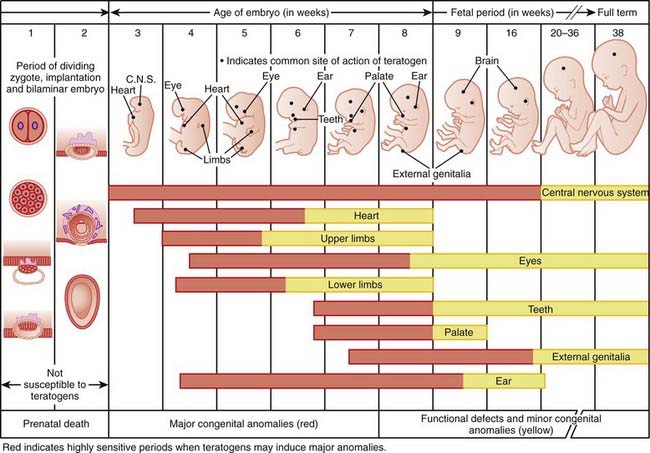
Timing of exposure is also important and is correlated with the stages of fetal development (Figure 5-1).
 First 14 days: Typically this is all or none, meaning that exposure results in death of the embryo or has no effect. The common feature of these two extremes is that they go undetected; if the embryo dies the patient does not realize she was ever pregnant.
First 14 days: Typically this is all or none, meaning that exposure results in death of the embryo or has no effect. The common feature of these two extremes is that they go undetected; if the embryo dies the patient does not realize she was ever pregnant.
 Day 61 onward: Exposure does not typically result in major structural malformations unless blood supply has been disrupted. However, from this point onward the major concern is fetotoxicity.
Day 61 onward: Exposure does not typically result in major structural malformations unless blood supply has been disrupted. However, from this point onward the major concern is fetotoxicity.

Neonates, Infants, and Children
Pharmacokinetics
Absorption
 Neonates typically have reduced peristalsis, although gastrointestinal (GI) motility can be unpredictable among neonates. Slowed peristalsis delays gastric emptying and drug absorption.
Neonates typically have reduced peristalsis, although gastrointestinal (GI) motility can be unpredictable among neonates. Slowed peristalsis delays gastric emptying and drug absorption. Neonates have a higher pH in the stomach, beginning life with an essentially neutral pH and, after a period of instability, gradually developing more acidic levels until they reach adult values at around the age of 2. This increased pH can have several potential effects:
Neonates have a higher pH in the stomach, beginning life with an essentially neutral pH and, after a period of instability, gradually developing more acidic levels until they reach adult values at around the age of 2. This increased pH can have several potential effects:




Distribution





Metabolism
 Drug metabolism is impaired at birth and gradually increases with time. The neonate is not born with a full complement of CYP450 enzymes but gradually acquires these enzymes through the first few weeks and months of life.
Drug metabolism is impaired at birth and gradually increases with time. The neonate is not born with a full complement of CYP450 enzymes but gradually acquires these enzymes through the first few weeks and months of life. Enzymes involved in glucuronidation take longer to develop, typically several months, and may not be fully operational for the first few years of life.
Enzymes involved in glucuronidation take longer to develop, typically several months, and may not be fully operational for the first few years of life.
 Chloramphenicol and the “gray baby” syndrome is a classic example of the consequences of impaired glucuronidation in neonates. If dosage of this antibiotic is not appropriately determined, the drug can accumulate, leading to several serious outcomes (including a gray color) and potentially even death in the newborn.
Chloramphenicol and the “gray baby” syndrome is a classic example of the consequences of impaired glucuronidation in neonates. If dosage of this antibiotic is not appropriately determined, the drug can accumulate, leading to several serious outcomes (including a gray color) and potentially even death in the newborn.Excretion
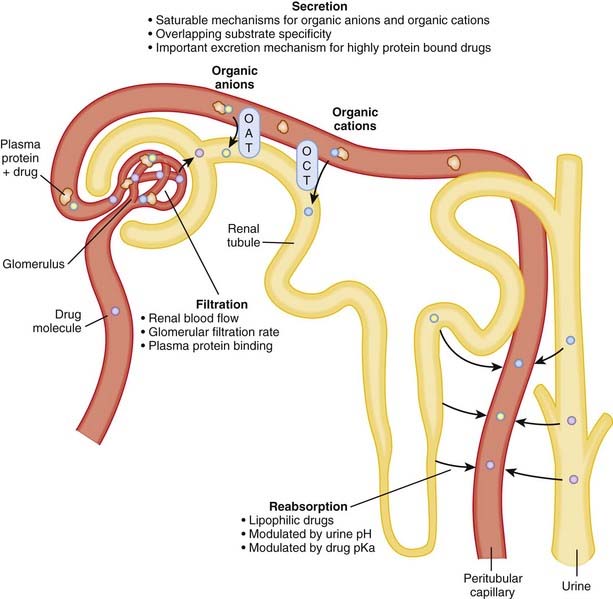
 Renal function in infants is significantly reduced in the first year of life compared with that in adults. Full-term babies are born with only 30% of normal glomerular filtration rate, and in preterm babies this number is even lower. These differences can lead to dramatic increases in the elimination half-lives of drugs that rely on the kidneys for clearance.
Renal function in infants is significantly reduced in the first year of life compared with that in adults. Full-term babies are born with only 30% of normal glomerular filtration rate, and in preterm babies this number is even lower. These differences can lead to dramatic increases in the elimination half-lives of drugs that rely on the kidneys for clearance.








Elderly
Pharmacokinetics
As with the very young, the impact of age on the very old is broken down here using the ADME system.
Absorption


Distribution
 Humans tend to dry out with age, so the elderly have a lower proportion of total body water than adults. Conversely, the elderly have a higher proportion of body fat. This means that hydrophilic drugs have a higher plasma concentration, and lipophilic drugs have a lower concentration, than in adults.
Humans tend to dry out with age, so the elderly have a lower proportion of total body water than adults. Conversely, the elderly have a higher proportion of body fat. This means that hydrophilic drugs have a higher plasma concentration, and lipophilic drugs have a lower concentration, than in adults.
Metabolism
Compared with adults, the elderly have impaired hepatic metabolic function for some drugs. This is because of a combination of a reduction in liver mass, hepatic blood flow, and activity of phase 1 enzymes (Box 5-2). Drugs that are metabolized by phase 2 enzymes appear to be less affected by advancing age.



Pharmacodynamics
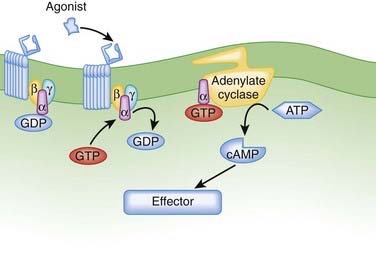
 Reduced cardiac β receptor activity. Although findings for receptor density have not been consistent, coupling of β1 adrenoceptors to G proteins appears to be impaired with age. Remember from the introductory pharmacodynamics chapter that G proteins mediate the cellular actions of a receptor (Figure 5-3).
Reduced cardiac β receptor activity. Although findings for receptor density have not been consistent, coupling of β1 adrenoceptors to G proteins appears to be impaired with age. Remember from the introductory pharmacodynamics chapter that G proteins mediate the cellular actions of a receptor (Figure 5-3).
Summary and Clinical Context
 Elderly patients are far more likely to be taking multiple medications, predisposing them to drug interactions.
Elderly patients are far more likely to be taking multiple medications, predisposing them to drug interactions.

The combination of all these limitations has increased focus on the issue of appropriate prescribing in the elderly. Lists of inappropriate drugs used in elderly patients have been generated and updated by several groups. One of the early lists consisted of the Beers criteria; some examples of the most harmful drugs from this list are in Table 5-2.
TABLE 5-2 List of Drugs That Are Inappropriate for Elderly Patients (Beers Criteria)
| Drug | Class | Description of Concern |
|---|---|---|
| Indomethacin | NSAID | CNS side effects worse than other NSAIDs |
BZD, Benzodiazepine; CNS, central nervous system; GI, gastrointestinal; NSAID, nonsteroidal antiinflammatory drug; t1/2, half-life; TCA, tricyclic antidepressant.