Chapter 17 Immune Modifiers
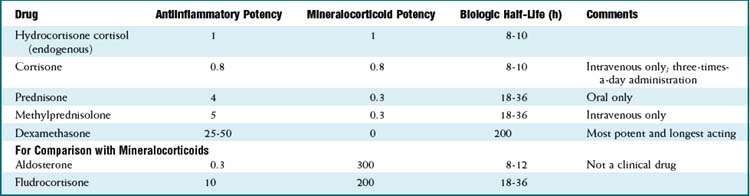
Systemic Steroids


MOA (Mechanism of Action)
 Cortisol is the endogenous glucocorticoid and is synthesized from cholesterol. The hypothalamus secretes corticotropin-releasing hormone (CRH), which stimulates the anterior pituitary to release adrenocorticotropic hormone (ACTH), which acts on the adrenal glands to produce cortisol.
Cortisol is the endogenous glucocorticoid and is synthesized from cholesterol. The hypothalamus secretes corticotropin-releasing hormone (CRH), which stimulates the anterior pituitary to release adrenocorticotropic hormone (ACTH), which acts on the adrenal glands to produce cortisol.

 Steroids exert their actions in a broad range of tissues, and therefore there are many effects of glucocorticoids:
Steroids exert their actions in a broad range of tissues, and therefore there are many effects of glucocorticoids:
 Catabolism
Catabolism



Pharmacokinetics


















Side Effects
















Important Notes
 The baseline secretion of cortisol in the body is 10 to 20 mg. In periods of stress (illness, trauma, inflammation, infection), the secretion increases.
The baseline secretion of cortisol in the body is 10 to 20 mg. In periods of stress (illness, trauma, inflammation, infection), the secretion increases.



Advanced
 Prophylactic antibiotics against Pneumocystis pneumonia (also called Pneumocystis jiroveci pneumonia or Pneumocystis carinii pneumonia [PCP]) are administrated to patients on long-term moderate- to high-dose steroids because of the risk of acquiring this infection when immunosuppressed. Human immunodeficiency virus (HIV) infection is the most common risk factor for PCP
Prophylactic antibiotics against Pneumocystis pneumonia (also called Pneumocystis jiroveci pneumonia or Pneumocystis carinii pneumonia [PCP]) are administrated to patients on long-term moderate- to high-dose steroids because of the risk of acquiring this infection when immunosuppressed. Human immunodeficiency virus (HIV) infection is the most common risk factor for PCP
Evidence
 Systemic steroids and adult asthma: A systematic review in 2009 concluded that the available studies were frequently underpowered. However, some general conclusions and recommendations were made: steroids administered in the emergency department reduce hospitalizations; steroids accelerate improvements in lung function; there was no benefit in using doses larger than 50 to 100 mg prednisone equivalent; and no benefit was seen when steroids were administered for longer than 5 to 10 days total.
Systemic steroids and adult asthma: A systematic review in 2009 concluded that the available studies were frequently underpowered. However, some general conclusions and recommendations were made: steroids administered in the emergency department reduce hospitalizations; steroids accelerate improvements in lung function; there was no benefit in using doses larger than 50 to 100 mg prednisone equivalent; and no benefit was seen when steroids were administered for longer than 5 to 10 days total.

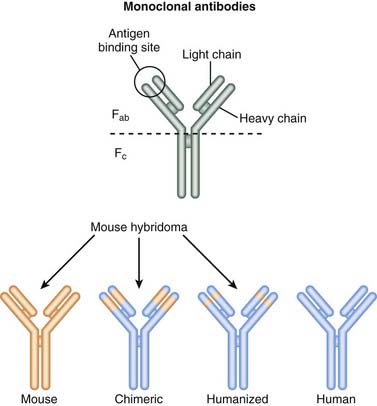
Introduction to Monoclonal Antibodies
Newer technologies are enabling the animal (usually mouse) portion of the antibody to be less and less, so that the resulting antibody is mostly human and therefore not destroyed by the patient’s own immune system for being a foreign antibody by human antimurine antibodies (HAMAs). Chimeric (human-mouse combination) antibodies contain fewer mouse regions than full mouse antibodies. Humanization involves replacing most of the mouse antibody with equivalent human regions while keeping only the variable, antigen-specific regions intact. Humanized mAbs have more human regions than chimeric mAbs do. Finally, fully human mAbs that contain no mouse regions are now being created (Figure 17-1).
Fusion Proteins
Use of Monoclonal Antibodies
The list of uses for mAbs is growing, but the major categories are as follows:
 Cancer: Cancer cells express unique antigens that can be directly targeted for destruction. Furthermore, there are growth factors that stimulate cancer cell growth that can also be inhibited.
Cancer: Cancer cells express unique antigens that can be directly targeted for destruction. Furthermore, there are growth factors that stimulate cancer cell growth that can also be inhibited. Immunosuppressants:
Immunosuppressants:



Naming Monoclonal Antibodies


Targets










Notes
Table 17-2 will not be fully inclusive by the time it is published because of the rapid growth of this area of medicine. Some drugs listed may not yet be approved for use.
| Name | Type | Target |
|---|---|---|
| Rituximab | Chimeric | CD20 on B lymphocytes |
| Ocrelizumab | Humanized | CD20 on B lymphocytes |
| Ofatumumab | Human | CD20 on B lymphocytes |
| Tositumomab | Mouse |
EGF, epidermal growth factor; HER2, human epidermal growth factor receptor 2; 131I, iodine-131; IgE, immunoglobulin E; IL, interleukin; 111In, indium-111; PSA, prostate-specific antigen; TNF, tumor necrosis factor; 90Y, yttrium-90.
B-Cell Biologics
Description
B-cell biologics specifically target B-cell lymphocytes for either destruction or suppression.



MOA (Mechanism of Action)
 Drugs that target B cells cause either destruction of the cells or interference with their ability to mount an immune response.
Drugs that target B cells cause either destruction of the cells or interference with their ability to mount an immune response. As a B cell–depleting agent (destruction of B cells):
As a B cell–depleting agent (destruction of B cells):




 As an immunomodulator (inhibitor of B cells):
As an immunomodulator (inhibitor of B cells):
 B-cell depletion (through the cytotoxic actions described previously) is an effective method of blunting a pathologic inflammatory response.
B-cell depletion (through the cytotoxic actions described previously) is an effective method of blunting a pathologic inflammatory response.




Pharmacokinetics
 The half-life of rituximab can be variable when treating tumor. The drug will become bound and removed from circulation when a high number of CD20 receptors are present, effectively decreasing the drug concentration and half-life. Therefore at the start of cancer therapy the half-life is around 75 hours, whereas at the end of therapy it can be as long as 200 hours.
The half-life of rituximab can be variable when treating tumor. The drug will become bound and removed from circulation when a high number of CD20 receptors are present, effectively decreasing the drug concentration and half-life. Therefore at the start of cancer therapy the half-life is around 75 hours, whereas at the end of therapy it can be as long as 200 hours.
Indications












Contraindications


Side Effects
Early







Important Notes
 CD20 antigen is not expressed by either plasma cells or B-lymphoid stem cells; therefore rituximab does not reduce total immunoglobulin (Ig) serum concentrations.
CD20 antigen is not expressed by either plasma cells or B-lymphoid stem cells; therefore rituximab does not reduce total immunoglobulin (Ig) serum concentrations.
Advanced
 B cell–depleting and B cell–nondepleting strategies have both been used for treatment of autoimmune diseases.
B cell–depleting and B cell–nondepleting strategies have both been used for treatment of autoimmune diseases. Future therapies:
Future therapies:
 BAFF (B-cell activating factor), also called BlyS (B-lymphocyte stimulator), prolongs the survival of B cells, stimulates maturation, and promotes survival of autoreactive B. Anti-BAFF antibodies (belimumab) or BAFF receptor fusion proteins (briobacept) are being investigated for treating RA and SLE.
BAFF (B-cell activating factor), also called BlyS (B-lymphocyte stimulator), prolongs the survival of B cells, stimulates maturation, and promotes survival of autoreactive B. Anti-BAFF antibodies (belimumab) or BAFF receptor fusion proteins (briobacept) are being investigated for treating RA and SLE.




T-Cell Biologics
Description
T-cell biologics specifically target T-cell lymphocytes for either destruction or suppression.







MOA (Mechanism of Action)
 The roles and activities of T cells are extremely diverse and complicated. Their contributions to disease are currently incompletely understood, and this section is a very simplified explanation of a very complicated system. This area of medicine is changing quickly, as is the understanding of these disease processes.
The roles and activities of T cells are extremely diverse and complicated. Their contributions to disease are currently incompletely understood, and this section is a very simplified explanation of a very complicated system. This area of medicine is changing quickly, as is the understanding of these disease processes.CD3
 CD3 is the defining marker for T cells. Therefore, all T cells express CD3. As a result, drugs that target CD3 have the potential to influence all subtypes of T cells and are therefore nonspecific. They will influence proinflammatory as well as antiinflammatory T cells and also target activated and nonactivated T cells.
CD3 is the defining marker for T cells. Therefore, all T cells express CD3. As a result, drugs that target CD3 have the potential to influence all subtypes of T cells and are therefore nonspecific. They will influence proinflammatory as well as antiinflammatory T cells and also target activated and nonactivated T cells.




CD25 (IL-2 Receptor)

Autoimmune Diseases
 Increased CD25 (IL-2 receptor) expression has been demonstrated in many autoimmune diseases. Suppression or antagonism of IL-2 has resulted in reduced inflammation in many of these diseases.
Increased CD25 (IL-2 receptor) expression has been demonstrated in many autoimmune diseases. Suppression or antagonism of IL-2 has resulted in reduced inflammation in many of these diseases. Important source of apparent conflict:
Important source of apparent conflict:







CD28 (CTLA-4)
Autoimmune Diseases






CD11a (LFA-1)
 CD11a is important for interactions between the integrin LFA-1 and cell adhesion molecule intercellular adhesion molecule 1 (ICAM-1). Integrins are proteins that facilitate the attachment of cells to other cells or to extracellular matrices. Once attached, the cell can transmigrate from the blood into the tissue, across the endothelial barrier.
CD11a is important for interactions between the integrin LFA-1 and cell adhesion molecule intercellular adhesion molecule 1 (ICAM-1). Integrins are proteins that facilitate the attachment of cells to other cells or to extracellular matrices. Once attached, the cell can transmigrate from the blood into the tissue, across the endothelial barrier.





Indications










Side Effects
 With all classes of drugs, the risk of immunosuppression leading to infection is an ever-present side effect.
With all classes of drugs, the risk of immunosuppression leading to infection is an ever-present side effect.
CD3
 With OKT3 only, cytokine release syndrome: a massive inflammatory response caused by binding to the T cells combined with Fc receptor cross-linking.
With OKT3 only, cytokine release syndrome: a massive inflammatory response caused by binding to the T cells combined with Fc receptor cross-linking.
 The syndrome is attributed to increased serum levels of cytokines, particularly the production of TNF.
The syndrome is attributed to increased serum levels of cytokines, particularly the production of TNF.


Evidence
Abatacept and Rheumatoid Arthritis
 A Cochrane review in 2009 (seven studies, 2908 patients) found that patients treated with abatacept, compared with placebo, were more likely (relative risk [RR] 2.21) to achieve clinical benefit as measured by the ACR50, an index of pain, disability, and number of affected joints. The number needed to treat (NNT) was 5. The risk of side effects was low (RR 1.05) compared with placebo, and the harms were assessed to be not significant except for increased infections assessed at 12 months.
A Cochrane review in 2009 (seven studies, 2908 patients) found that patients treated with abatacept, compared with placebo, were more likely (relative risk [RR] 2.21) to achieve clinical benefit as measured by the ACR50, an index of pain, disability, and number of affected joints. The number needed to treat (NNT) was 5. The risk of side effects was low (RR 1.05) compared with placebo, and the harms were assessed to be not significant except for increased infections assessed at 12 months.
Mixed Biologics


MOA (Mechanism of Action)
CD52 (CAMPATH-1)






















Side Effects









Tumor Necrosis Factor (TNF)–α Inhibitors




MOA (Mechanism of Action)
 TNF-α is mostly produced by macrophages but is also produced by other inflammatory cells. It binds to TNF receptors (called TNFRs), which are present on many different cells of the immune system.
TNF-α is mostly produced by macrophages but is also produced by other inflammatory cells. It binds to TNF receptors (called TNFRs), which are present on many different cells of the immune system.
 The inflammatory cascades are very complicated. TNF-α is believed to exert its proinflammatory actions by promoting:
The inflammatory cascades are very complicated. TNF-α is believed to exert its proinflammatory actions by promoting:















Side Effects










Important Notes
 Anti-TNF therapy for RA is considered a biologic DMARD, which, as previously noted, stands for disease-modifying antirheumatic drug. DMARDs slow the progression of joint destruction. Use of DMARDs is in contrast to “symptom-only” therapy, which would include analgesics (such as acetaminophen or NSAIDs), in that symptom-only therapy does not slow the progression of the disease.
Anti-TNF therapy for RA is considered a biologic DMARD, which, as previously noted, stands for disease-modifying antirheumatic drug. DMARDs slow the progression of joint destruction. Use of DMARDs is in contrast to “symptom-only” therapy, which would include analgesics (such as acetaminophen or NSAIDs), in that symptom-only therapy does not slow the progression of the disease.
Advanced
 TNF is active when three monomers bind together into a trimeric unit and bind to two different receptors: TNFR1 and TNFR2. These receptors are also called p55 and p75, respectively.
TNF is active when three monomers bind together into a trimeric unit and bind to two different receptors: TNFR1 and TNFR2. These receptors are also called p55 and p75, respectively.

Evidence
Rheumatoid Arthritis
Monotherapy versus Methotrexate, and Monotherapy versus Combination Therapy
 A 2008 systematic review of DMARD therapy for RA concluded that anti-TNF monotherapy was similar in efficacy to treatment with methotrexate alone, whereas the combination of an anti-TNF agent with methotrexate reduced disease activity more and slowed radiographic progression to a greater extent than did anti-TNF monotherapy or methotrexate alone. These findings were similar to those of a Cochrane review in 2009 that examined all biologic DMARDs in the treatment of RA.
A 2008 systematic review of DMARD therapy for RA concluded that anti-TNF monotherapy was similar in efficacy to treatment with methotrexate alone, whereas the combination of an anti-TNF agent with methotrexate reduced disease activity more and slowed radiographic progression to a greater extent than did anti-TNF monotherapy or methotrexate alone. These findings were similar to those of a Cochrane review in 2009 that examined all biologic DMARDs in the treatment of RA.Infliximab (with or without Methotrexate) versus Placebo (Plus Methotrexate)
 A Cochrane review in 2002 (two trials, 529 patients) found that after 6 months, response rates were significantly improved with all infliximab doses compared with controls. The NNT with infliximab to achieve an American College of Rheumatology (ACR) 20, 50, or 70 response (these are different measures of response based on disability, pain, and number of affected joints) in patients with refractory RA under specialist care ranged from 2.94 to 3.33 for ACR 20, up to 5.88 to 12.5 for ACR 70. Withdrawals because of adverse events and withdrawals for other reasons were not statistically significantly different in patients receiving infliximab than in controls.
A Cochrane review in 2002 (two trials, 529 patients) found that after 6 months, response rates were significantly improved with all infliximab doses compared with controls. The NNT with infliximab to achieve an American College of Rheumatology (ACR) 20, 50, or 70 response (these are different measures of response based on disability, pain, and number of affected joints) in patients with refractory RA under specialist care ranged from 2.94 to 3.33 for ACR 20, up to 5.88 to 12.5 for ACR 70. Withdrawals because of adverse events and withdrawals for other reasons were not statistically significantly different in patients receiving infliximab than in controls.




Antimetabolites



MOA (Mechanism of Action)
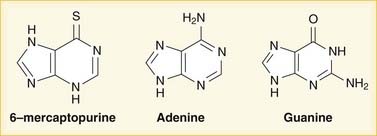
 Purines and pyrimidines are the two types of bases used in DNA and RNA. Purines are guanine (G) and adenine (A); pyrimidines are cytosine (C), thymine (T), and uracil (U). Uracil (U) is found only in RNA, whereas thymine (T) is only in DNA. The bases are all attached to a single phosphate group, making them monophosphates.
Purines and pyrimidines are the two types of bases used in DNA and RNA. Purines are guanine (G) and adenine (A); pyrimidines are cytosine (C), thymine (T), and uracil (U). Uracil (U) is found only in RNA, whereas thymine (T) is only in DNA. The bases are all attached to a single phosphate group, making them monophosphates.
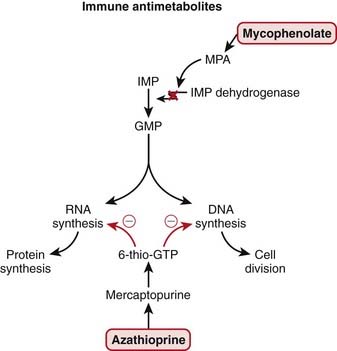
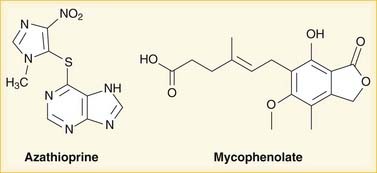
 Mycophenolate is hydrolyzed to mycophenolic acid (MPA), which inhibits IMP dehydrogenase and thereby prevents GMP production. GMP is a required base for both DNA and RNA, and without it, DNA and RNA synthesis is reduced (Figure 17-2).
Mycophenolate is hydrolyzed to mycophenolic acid (MPA), which inhibits IMP dehydrogenase and thereby prevents GMP production. GMP is a required base for both DNA and RNA, and without it, DNA and RNA synthesis is reduced (Figure 17-2).
 Regardless of the exact mechanism of action on DNA and RNA:
Regardless of the exact mechanism of action on DNA and RNA:
 Reduced DNA synthesis results in reduced proliferation of cells. As a general rule, rapidly dividing cells are more sensitive to drugs that influence cell division. These include the following:
Reduced DNA synthesis results in reduced proliferation of cells. As a general rule, rapidly dividing cells are more sensitive to drugs that influence cell division. These include the following:

 Two features of antimetabolites that make them a little more specific to inhibiting the immune system include:
Two features of antimetabolites that make them a little more specific to inhibiting the immune system include:



Pharmacokinetics
Azathioprine
 Azathioprine is metabolized quickly (half-life of 10 minutes) but has many active metabolites; therefore blood level measurements of the parent drug do not provide useful information.
Azathioprine is metabolized quickly (half-life of 10 minutes) but has many active metabolites; therefore blood level measurements of the parent drug do not provide useful information. Azathioprine is metabolized by the liver to mercaptopurine; mercaptopurine metabolism occurs via a couple different enzymes, one of which is xanthine oxidase, an enzyme that is important in the disease gout; allopurinol, a xanthine oxidase inhibitor used to treat gout, results in dramatically increased levels of active metabolites. This is an important drug interaction.
Azathioprine is metabolized by the liver to mercaptopurine; mercaptopurine metabolism occurs via a couple different enzymes, one of which is xanthine oxidase, an enzyme that is important in the disease gout; allopurinol, a xanthine oxidase inhibitor used to treat gout, results in dramatically increased levels of active metabolites. This is an important drug interaction.
 Another important enzyme that metabolizes mercaptopurine is thiopurine methyltransferase (TPMT); the TPMT activity rate is very important because TPMT catalyzes a reaction to produce an inactive metabolite and is therefore felt to be a strong predictor for myelosuppression and hepatotoxicity. Patients with low TPMT activity develop higher levels of 6-thio-GTP and are therefore more susceptible to acute bone marrow suppression and liver damage. TPMT activity is genetically determined, and tests for TPMT activity levels are available.
Another important enzyme that metabolizes mercaptopurine is thiopurine methyltransferase (TPMT); the TPMT activity rate is very important because TPMT catalyzes a reaction to produce an inactive metabolite and is therefore felt to be a strong predictor for myelosuppression and hepatotoxicity. Patients with low TPMT activity develop higher levels of 6-thio-GTP and are therefore more susceptible to acute bone marrow suppression and liver damage. TPMT activity is genetically determined, and tests for TPMT activity levels are available.



Side Effects

















Important Notes
 In treatment of autoimmune diseases, steroids are generally the first-line immunosuppressants employed because they act quickly; however, there are many side effects related to prolonged steroid use, and therefore nonsteroid immunosuppressants are generally preferred for long-term immunosuppression. Antimetabolites are used therefore for long-term “steroid-sparing” immunosuppression.
In treatment of autoimmune diseases, steroids are generally the first-line immunosuppressants employed because they act quickly; however, there are many side effects related to prolonged steroid use, and therefore nonsteroid immunosuppressants are generally preferred for long-term immunosuppression. Antimetabolites are used therefore for long-term “steroid-sparing” immunosuppression.
Advanced
 Azathioprine is converted to mercaptopurine; however, azathioprine is felt to be a more effective immunosuppressant than mercaptopurine because of increased intracellular uptake. Intracellular levels of the metabolite 6-thio-GTP need to be high for the drugs to be effective, and azathioprine appears to be taken up specifically by lymphocytes.
Azathioprine is converted to mercaptopurine; however, azathioprine is felt to be a more effective immunosuppressant than mercaptopurine because of increased intracellular uptake. Intracellular levels of the metabolite 6-thio-GTP need to be high for the drugs to be effective, and azathioprine appears to be taken up specifically by lymphocytes.




Calcineurin Inhibitors


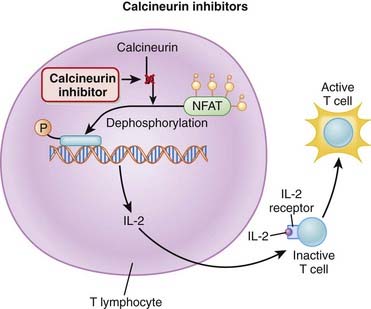
MOA (Mechanism of Action)
 These drugs act on T cells (a type of lymphocyte). T cells are involved in cell-mediated immunity (as opposed to humoral immunity, which is mediated by B lymphocytes).
These drugs act on T cells (a type of lymphocyte). T cells are involved in cell-mediated immunity (as opposed to humoral immunity, which is mediated by B lymphocytes).





Pharmacokinetics
 Cyclosporine has a narrow therapeutic index. Levels must be frequently measured to help reduce the probability of side effects.
Cyclosporine has a narrow therapeutic index. Levels must be frequently measured to help reduce the probability of side effects.



Indications




Side Effects












Important Notes
 In patients with kidney transplants (a population of patients who regularly receive calcineurin inhibitors), it can be diagnostically difficult to determine if declining renal function is a result of rejection (which would be managed by increasing the dose or adding immunosuppressive drugs) or of toxicity of the immunosuppressive drugs (which would be managed by lowering the dose or stopping the drugs).
In patients with kidney transplants (a population of patients who regularly receive calcineurin inhibitors), it can be diagnostically difficult to determine if declining renal function is a result of rejection (which would be managed by increasing the dose or adding immunosuppressive drugs) or of toxicity of the immunosuppressive drugs (which would be managed by lowering the dose or stopping the drugs).Advanced
 Less common side effects include the following:
Less common side effects include the following:
 Haemolytic uremic syndrome is characterized by microangiopathic anemia, thrombocytopenia, and acute renal failure. Simply thought of, it is a process whereby platelets are consumed into intravascular aggregates, causing a meshwork of clots that lyse red blood cells and the floating intracellular debris plugs up the glomeruli and tubules, resulting in kidney failure.
Haemolytic uremic syndrome is characterized by microangiopathic anemia, thrombocytopenia, and acute renal failure. Simply thought of, it is a process whereby platelets are consumed into intravascular aggregates, causing a meshwork of clots that lyse red blood cells and the floating intracellular debris plugs up the glomeruli and tubules, resulting in kidney failure.










Target of Rapamycin (mTOR) Inhibitors


MOA (Mechanism of Action)
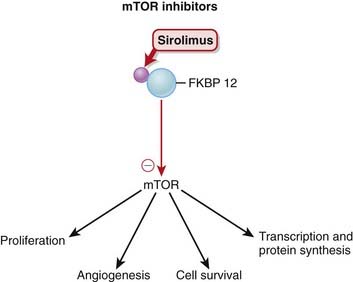
 mTOR (mammalian target of rapamycin) is a serine-threonine protein kinase activated by several growth factors after receptor binding.
mTOR (mammalian target of rapamycin) is a serine-threonine protein kinase activated by several growth factors after receptor binding. Sirolimus binds a protein called FKBP 12 (FKBP stands for FK506 binding protein) in the cytoplasm. The drug-protein complex then binds and inhibits mTOR (Figure 17-6).
Sirolimus binds a protein called FKBP 12 (FKBP stands for FK506 binding protein) in the cytoplasm. The drug-protein complex then binds and inhibits mTOR (Figure 17-6).







Pharmacokinetics








Side Effects






Important Notes
 Sirolimus is not nephrotoxic, a very significant advantage over calcineurin inhibitors, especially when being used in the setting of renal transplant, when every effort is made to protect the new transplanted kidney. Calcineurin inhibitors, which are also used in renal transplant patients, are nephrotoxic.
Sirolimus is not nephrotoxic, a very significant advantage over calcineurin inhibitors, especially when being used in the setting of renal transplant, when every effort is made to protect the new transplanted kidney. Calcineurin inhibitors, which are also used in renal transplant patients, are nephrotoxic.Advanced
 Sirolimus first binds FKBP (FK506 binding protein), the protein that FK506 (tacrolimus) binds to. However, the drug-protein complex when bound to sirolimus acts differently than when bound to tacrolimus. Therefore the two drugs act on the same protein in the body but in a different way.
Sirolimus first binds FKBP (FK506 binding protein), the protein that FK506 (tacrolimus) binds to. However, the drug-protein complex when bound to sirolimus acts differently than when bound to tacrolimus. Therefore the two drugs act on the same protein in the body but in a different way.











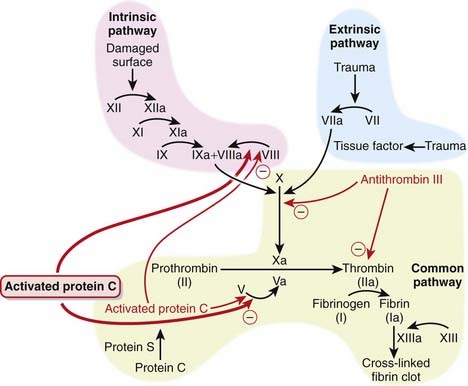
Activated Protein C
Description
Activated protein C is part of the coagulation cascade but is used as an antiinflammatory.

MOA (Mechanism of Action)











Pharmacokinetics
 Activated protein C is metabolized by plasma proteases: 80% is eliminated within 13 minutes, and 98% is cleared within 2 hours. This is important because patients with septic shock sometimes require surgery, and activated protein C needs to be discontinued 2 hours before surgery. Furthermore, if bleeding occurs while a patient is on activated protein C, then the anticoagulant effect can be reversed within 2 hours.
Activated protein C is metabolized by plasma proteases: 80% is eliminated within 13 minutes, and 98% is cleared within 2 hours. This is important because patients with septic shock sometimes require surgery, and activated protein C needs to be discontinued 2 hours before surgery. Furthermore, if bleeding occurs while a patient is on activated protein C, then the anticoagulant effect can be reversed within 2 hours.





Evidence
 In two large RCTs (the PROWESS and ADDRESS studies) comparing activated protein C with placebo, a mortality benefit (absolute risk reduction of 6.1%) was demonstrated in patients who were very sick (APACHE score greater than 25) and treated with activated protein C. However, there was no mortality benefit in patients who were less sick (APACHE score less than 25).
In two large RCTs (the PROWESS and ADDRESS studies) comparing activated protein C with placebo, a mortality benefit (absolute risk reduction of 6.1%) was demonstrated in patients who were very sick (APACHE score greater than 25) and treated with activated protein C. However, there was no mortality benefit in patients who were less sick (APACHE score less than 25).FYI
 APACHE stands for Acute Physiology and Chronic Health Evaluation, and the APACHE scoring system is used to describe severity of illness of patients admitted to the intensive care unit. The score ranges from 0 to 71 and is based on 17 physiologic parameters such as heart rate, white blood count, and Pco2.
APACHE stands for Acute Physiology and Chronic Health Evaluation, and the APACHE scoring system is used to describe severity of illness of patients admitted to the intensive care unit. The score ranges from 0 to 71 and is based on 17 physiologic parameters such as heart rate, white blood count, and Pco2.


Glatiramoids

MOA (Mechanism of Action)















Important Notes
 CIS is characterized by a single demyelinating event, an attack that is suggestive of MS. These attacks include typical MS symptoms, such as sudden loss of vision. CIS is a recognized precursor to development of MS, although not all patients with CIS will go on to develop this disease. This has made it difficult to determine whether CIS patients should be initiated on this very expensive therapy, which includes daily injections, for an indeterminate amount of time.
CIS is characterized by a single demyelinating event, an attack that is suggestive of MS. These attacks include typical MS symptoms, such as sudden loss of vision. CIS is a recognized precursor to development of MS, although not all patients with CIS will go on to develop this disease. This has made it difficult to determine whether CIS patients should be initiated on this very expensive therapy, which includes daily injections, for an indeterminate amount of time.
Advanced
 A new class of drugs has emerged in the fight against MS. The integrin inhibitors prevent the movement of lymphocytes from blood vessels into the brain. α4β1 Integrin is expressed on the surface of activated lymphocytes and acts on a receptor on the luminal surface of vascular endothelium, vascular cell adhesion molecule (VCAM).
A new class of drugs has emerged in the fight against MS. The integrin inhibitors prevent the movement of lymphocytes from blood vessels into the brain. α4β1 Integrin is expressed on the surface of activated lymphocytes and acts on a receptor on the luminal surface of vascular endothelium, vascular cell adhesion molecule (VCAM).





