Effects of high maternal oxygen concentrations on the fetus
When necessary, 100% O2 may be given to a parturient to improve fetal oxygenation; however, maternal hyperoxygenation may have a harmful effect on the developing fetal vascular beds. For more than a century, research has shown that, as a result of the harmful effects of free O2 radicals and oxidative stress, O2 can be toxic, particularly to the vascular beds of the central nervous system, the eye, and pulmonary circulation. It is also now clear that preterm infants are more susceptible to O2 toxicity than are full-term infants. Several factors are known to affect severity of injury related to O2 toxicity (Box 187-1).
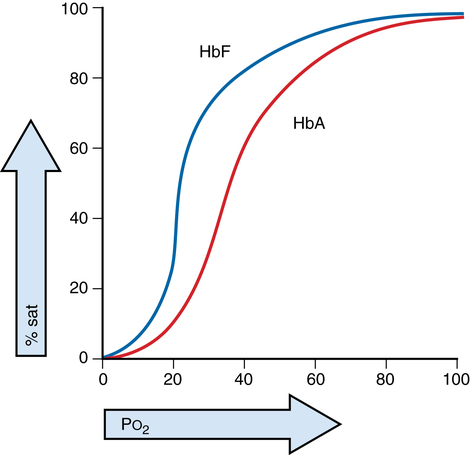
Within the fetomaternal circulation, the highest possible partial pressure gradient of O2 that can be delivered to the fetus in utero is limited by the fetomaternal gas-exchange mechanisms (Figure 187-1). The placenta is 15 times less efficient at gas exchange than is the lung; however, the unloading of O2 to the fetus is enhanced by several biochemical mechanisms.