Educational Aspects of Emergency Department Procedures
Learning to perform emergency department (ED) procedures is a complex and highly individualized educational process. No longer is the maxim of “see one, do one, teach one” an acceptable educational practice.1 For many emergency medicine (EM) physicians, residency training may be the primary source of instruction on a wide range of common and uncommon procedures.2 A variety of modalities and educational tools exist to aid medical educators in initial training and long-term skill retention.
Concepts in Procedural Skill Training
Formal Education
Chapman described a set of eight steps to use as a framework for procedural learning (Box 69-1).3 These steps incorporate the different stages of learning and are important to understand when teaching a procedural skill. This framework is best thought of as a longitudinal approach to teaching procedures over time. It includes focused preparation and memorization before any attempt at performance and progresses to actual practice with repeated feedback and assessment of competency. This outline is closely linked to theories of motor skill acquisition in which learners progress from cognition (understanding the task through explanation and demonstration) to integration (performing the task deliberately and with feedback) and finally to automation (increased speed, efficiency, and precision of the procedure).4
A practical synthesis of these theories for general practice has been described in a four-step process often used to teach procedural skills in a shorter time frame, such as in a simulation session or brief skills course.5 In this approach, an expert teacher demonstrates the skill at regular speed without detailed explanation. Next, the educator performs the procedure slowly and with detailed commentary. Third, the learner verbalizes the skill steps back to the teacher. Finally, the learner performs the procedure, with detailed discussion of each step before performing it.
Traditional lecture formats (small or large group) are often used for initial skill teaching (Figs. 69-1 and 69-2). However, there are other methods to introduce a skill concept. Using the four-step method, demonstration and deconstruction could be performed individually by the learner before a teaching session with standard texts, video, or other designated online resource.5,6 Once the learner has progressed to actual practice of the skill, expert assistance and feedback are crucial to progression and mastery and may be the most important feature in some types of skill acquisition.1 Feedback is not only informative but also motivational and should be directed externally (i.e., at the correct motor steps) rather than internally (i.e., at the individual’s particular movements).7 Learner-centered feedback should be delivered by expert tutors who slowly decrease their support as a trainee’s proficiency increases.8
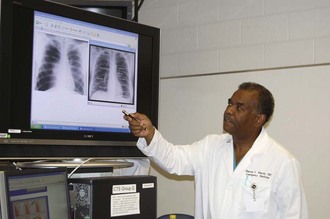
Figure 69-1 Formal lecture to teach a new procedure.

Procedural Training at the Bedside
Training at the bedside remains a common and important way to teach residents. Learners should go through formal training in the procedure before attempting it on a live patient. The clinical setting (Fig. 69-3B) should allow adequate time to discuss the procedure in detail. The teacher and learner should review the indications, contraindications, equipment, procedural steps, critical actions, and complications. The resident should be able to verbalize the steps involved in the procedure. This review may be provided either outside the patient’s room or at the bedside, depending on the patient and the clinical scenario. The teacher should observe the learner as she or he performs the procedure and provide guidance and assistance when needed (see Fig. 69-3C). After the procedure, the teacher should examine the patient and assess the adequacy of the procedure, discuss problems that occurred during the procedure, offer suggestions for improvement, and provide a review of postprocedural care (see Fig. 69-3D).

The learner should be encouraged to engage the patient while practicing the procedure. In an article on bedside teaching, Monrouxe and colleagues suggested having students explain what they are doing to the patient in lay language because patients like to be involved in teaching so that they can learn more about their condition.9 Explaining the procedure to the patient as it is performed can help consolidate the steps in the learner’s mind and make the patient feel that he or she is an active part of the teaching process.
As part of bedside learning, newly deceased patients—those who have not expressly given consent for use of their bodies—have historically been used to practice procedures. In 1994, a survey of program directors of EM and critical care training programs found that 63% of EM programs allow procedures to be performed on newly dead patients.10 Additionally, in a survey involving theoretical clinical scenarios, lay people responded that they would agree to after-death procedures on themselves in 75% of cases and on their relatives in 69% of cases with prior consent. Without prior consent, they would allow such procedures 40% of the time on themselves and 50% on their family members.11
Despite this apparent acceptance of performing invasive procedures on the newly dead by both educators and members of the public, this practice may be limited by certain debated ethical concerns.12–16 There are many alternatives for procedural teaching if bedside teaching on a live, consenting patient is not feasible. Learning on newly deceased patients is not a necessary part of medical education and may, with its attendant ethical pitfalls, be easily avoided without detrimental effect on residents in training.
Educational Alternatives for Practicing Procedures
Simulation
We are now well into the information age, and medical simulation is taking an increasingly important role in medical education. An invaluable teaching tool, medical simulation can be used to improve a learner’s competence and confidence, expose a learner to rare, but potentially lifesaving procedures, and decrease the rate of procedural errors. With a simulator, learners have the opportunity to practice every procedure that they need to know under a variety of different conditions. Modern human patient simulators have been developed or are currently under development for endotracheal intubation, chest compression, electrical cardioversion, cricothyroidotomy, chest tube insertion, pericardiocentesis, diagnostic peritoneal lavage, emergency thoracotomy, lumbar puncture, skin suturing, insertion of peripheral venous and arterial catheters, insertion of central venous lines, and more.17 Many studies have demonstrated the efficacy and applicability of simulation with regard to procedural education.18–20 A panel consisting of members from the Society for Academic Emergency Medicine (SAEM) Simulation Interest Group of the SAEM Technology in Medical Education Committee made the recommendation that “simulation-based training should prioritize procedures infrequently encountered in clinical practice and commonly performed procedures that possess a potential risk to a patient when performed by the less skilled practitioner.” Two main types of simulators are in common use.
Task Trainers
Procedures can be simulated by using task trainers to teach procedures when available (Fig. 69-4). Each task trainer is a model designed to teach one specific procedure. Models are available for many procedures, including cardiopulmonary resuscitation, peripheral venipuncture, arterial puncture, intraosseous infusion, umbilical vessel catheterization, central line catheterization, lumbar puncture, endotracheal intubation, needle thoracostomy, urinary catheter placement, suturing, and emergency childbirth. They are limited by their inability to perfectly imitate the qualities of human tissue, to simulate force and tactile feedback, and to simulate complications. For example, chest tube task trainers do not bleed when the skin is cut into.

High-Fidelity Simulation
High-fidelity simulation is designed to mimic a real-life medical scenario, including the procedures, decision-making skills, and possible permutations that may occur (Fig. 69-5).21 This requires a high-fidelity mannequin, an instructor, a script, a scenario, and a debriefing. The instructor’s responsibility is to create an environment that resembles reality as closely as possible.17 Even though the script is standardized, the software and mannequin can take into account the unpredictable actions of participants, including simulating complications that would occur if certain decisions were made in a real-life scenario. The instructor may redirect participants to take an action that will result in a predetermined response. The debriefing process is also an important learning opportunity in which mistakes can be discussed and alternative courses of action can be explored.

In a review of simulation technology, Reznek and associates wrote that to be an effective teaching tool,17 a simulator must provide both educationally sound and realistic feedback to a user’s questions, decisions, and actions.
Cadaver Laboratories
Fresh cadavers are ideal for teaching procedures. To clarify, these are the bodies of individuals who have given consent for their bodies to be used for teaching. The advantage of using a fresh cadaver is that it more clearly resembles the tissue properties and pliability of a live human. The disadvantages are cost, limited availability, and potential risk for transmission of disease.22
Preserved cadavers are also an option if they are more readily available at your institution. A cadaver laboratory offers the advantage of a standardized reproducible laboratory experience under the guidance of an instructor and with no risk to the patient.23 Disadvantages of preserved cadavers are that they do not bleed and they suffer from tissue adherence because of the preservation process, so though excellent for learning the anatomy of procedures, they may not completely simulate the in vivo experience.24
Long-Term Skill Retention and Uncommon Procedures
When teaching procedures, long-term skill retention is the goal because decay of procedural skills over time is natural. Information is lost from short-term memory through decay and interference, but fortunately, once committed to long-term memory, it is virtually permanent.25,26 This is analogous to certain learned skills that are retained indefinitely, such as riding a bicycle. These skills are never forgotten because of a process called overlearning. Allowing learners to practice and execute movements actively during learning results in better recall than when they learn from a passive demonstration.27,28 The exact number of times that a trainee must practice a particular skill is unknown, but certain factors have been shown to have an impact on skill retention: quality of the initial instruction, methodology of instruction and testing or evaluation, overlearning, retrieval conditions, length of the interval between training and actual practice, and individual learner and procedure qualities.29
Procedural learning curves are often steep, with novices showing the greatest improvement in skill initially and a plateau effect for more experienced practitioners.29 A study of intubation skills using different task trainers and models found that learners had a success rate of only 50% when performing the skill for the first time on a new trainer but that after 10 to 12 trials on the same trainer, success levels reached a plateau of approximately 80%.30 This same study also found that trainees learned more quickly after successful intubations than after failed ones, and the authors suggested that varying methods of practicing a skill slows learning but leads to increased retention and application to new settings.
Limited research has investigated the long-term practical retention of procedural skills. For most ED procedures, which are rarely overlearned, practice is required to maintain these skills.3 Kovacs and colleagues demonstrated that airway management skills decline early after initial training but that performance may be maintained effectively with independent practice and periodic feedback.31 A study of central line insertion found increased competence 3 months after a simulation-based training course, although there was a slight regression from the immediate posttest performance scores.32 Similarly, Boet and coworkers found improved cricothyroidotomy skills at 6 and 12 months after simulator case instruction, although again there was regression from the immediate post-learning scores.33 A chief limitation of these and other similar studies is that longitudinal skill retention is often not measured in actual clinical practice, but on simulators or task trainers, so the long-term effect of specific procedural skill teaching sessions on translation to performance on patients in real clinical situations remains unclear.29
Training for Uncommon Procedures
The rate of performance of certain resuscitative procedures in recent years has declined because of several factors. For some procedures, such as ED thoracotomy, critical analyses of patient outcomes after ED thoracotomy have identified narrow conditions for decreased mortality (most notably penetrating trauma to the chest), which has virtually eliminated performing this procedure on victims of blunt trauma.34,35 Chang and associates reported a significant decline in the rate of cricothyroidotomies performed on trauma patients following the beginning of a new EM residency training program.36 They attributed this to several possible causes, including the widespread application of rapid-sequence intubation techniques, the presence of supervisory EM faculty 24 hours a day, and diminished concern regarding orotracheal intubation of patients whose cervical spines have not been radiographically cleared. Competition for procedures between EM residents and those from other specialties has increased; in fact, a survey of EM residency directors found that overall, emergency clinicians perform only 50% of 10 index procedures in the ED.37,38
Previous studies of EM residency trainees have confirmed the thought that certain emergency procedures are performed infrequently during the training years.39–41 A 2008 paper on developing technical expertise in EM procedures via simulation identified several “high-risk, low-frequency” ED procedures: cricothyroidotomy, transvenous cardiac pacing, pericardiocentesis, vaginal delivery, and pediatric resuscitation (medical and trauma).42 They suggested that because the correlation between simulator competence and actual practice ability is unknown, models or simulated scenarios that provide real-life situational learning should be encouraged and studied as bridges to actual practice. Wong and coworkers found that learners who participated in a cricothyroidotomy training session involving the use of video instruction and mannequin practice achieved 96% success rates within 40 seconds by the fifth attempt (with a skill and time plateau for all subsequent attempts).43 Although the exercise was performed on a mannequin, adding a time constraint as part of the metric of success may be indicative of a more realistic situation. An animal procedure laboratory targeted to several uncommon procedures found that learners’ confidence and willingness to perform these skills increased significantly, and use of live animals—though not applicable to all settings—may also enhance the realism of task performance (Fig. 69-6).44

Teaching Key ED Procedures
Airway Management
Airway management is a frequently encountered procedure and critical skill to be mastered for any emergency physician (EP).45 Both uncomplicated and difficult airway scenarios can be expected throughout the course of an EM residency and career. EPs must be taught to proficiently use a wide range of devices, from extraglottic tools to direct laryngoscopy and video-assisted or fiberoptic intubation equipment.
Much of the literature on methods of teaching airway management focuses on manikins or specific airway task trainers and more realistic patient simulators. No studies have proved the superiority of one specific type of manikin (high or low fidelity) for teaching intubation,42 but they have been used to train learners on a wide variety of devices. A 1-year study of learners in a simulation center used manikins for initial stepwise teaching of uncomplicated intubations and then increased the difficulty of techniques and simulator scenarios.46 The authors found that when using this method, the ideal ratio of learners to teachers was 2 : 1 and that it took each trainee approximately 75 to 90 minutes to achieve skill proficiency. Other researchers have found that simulator airway training improves performance on cadavers and recommended simulation for difficult or more realistic airway training.47–49 Simulators have limitations in the teaching of airway skills. As one study noted, they were not effective in trainees’ identification or management of esophageal intubation.50
The type of airway device used to train novice intubators has also been studied. Use of a video-assisted laryngoscope or flexible fiberoptic scope may provide an excellent teaching environment in that both the learner and teacher can watch the procedure in real time on a video screen (Fig. 69-7).51 Educators can then give immediate feedback and guidance as the skill is being performed. Several studies have found superior acquisition and efficiency of intubating skills with video-assisted devices as compared with traditional direct laryngoscopy.52–55

Figure 69-7 Use of a video-assisted laryngoscope provides an excellent opportunity for learning airway skills.
Formal methods of instruction and feedback on airway management also have an impact on learners’ experiences and long-term skill retention. For simple airway techniques such as insertion of a laryngeal mask airway, the four-step method of skills teaching described earlier has not been found to be statistically different from the two-step (“see one, do one”) approach.56
Learners who receive both regular feedback and dedicated airway practice at standard intervals have significantly higher and more stable procedural skill retention over time.31 Another study of novice student learners found that an “experiential” group (trainees given autonomy to figure out the correct intubating technique on their own) had significantly higher long-term procedural success rates than did a group of students taught via a conventional stepwise approach.57 Similarly, another study of novice intubators found that learners presented with a variety of manikins had low success rates on their initial attempt on each but quickly changed their technique to fit the particular model and had rapid progression to proficiency thereafter.58
Lumbar Puncture
Although lumbar puncture is a common ED procedure, few trainees have a great deal of experience before residency.59 As with other EM skills, task trainers and simulators are available to aid in teaching and practice of this skill. A training program for EM residents consisting of a traditional lecture, video demonstration, and simulator practice demonstrated competence initially after completion and additionally at 6 months.60 A study of pediatric trainees demonstrated no difference at 7 months in lumbar puncture skills on a simulator or self-reported live-patient success after a dedicated procedure training program.61 Because pediatric residents often perform a low number of clinical lumbar punctures,62 it may be that EM trainees’ skill retention is related to a higher volume of real-life procedural opportunities.
Cricothyroidotomy
Perhaps the most-feared ED procedure, cricothyroidotomy is established as a “high-risk, low-frequency” critical skill.7 Because of obvious ethical issues and the rarity of the procedure—less than 1% of all airway interventions in a large trial—cricothyroidotomy has no opportunity for safe real-life practice while achieving competence.63 Before the advent of manikins and simulators, cadaver and animal models were used for skill training and remain a part of cricothyroidotomy education. An anesthesia-based study recommended that based on learner experience and feedback, cadaveric practice be a mandatory part of any educational curriculum for cricothyroidotomy.12 Anesthetized animals (or animal tracheas) are also used for training in this procedure, and animal practice has been shown to be accessible to novices and at least equivalent to conventional teaching in terms of speed, proficiency, and long-term (6-month) retention.64,65
With the ubiquity of nonliving models, much cricothyroidotomy training takes place on manikins or simulators. Animals and cadavers can be resource-intensive and are often limited by single use, whereas several different types of reusable synthetic “skins” allow multiple practice attempts on a simulator or task trainer. As with intubation, full-model, high-fidelity simulator scenarios, along with regular practice and feedback, are thought to best replicate real-life complex cases and promote long-term skill retention.33,43,66 Whether the four-step or two-step method of skills training is superior for this procedure is unknown. A study of medical students demonstrated no significant difference between these approaches in terms of speed or proficiency.6
Ultrasound-Guided Procedures
A full description of teaching methods for the wide range of ultrasound-guided procedures is beyond the scope of this chapter. This group of skills has been identified as a “high-frequency, low-risk” domain of expected competence.42 For a number of these procedures, simulators both specialized (i.e., a vaginal model with ectopic pregnancy or special trauma abdomen with free fluid) and general are of benefit for training. Learners express improved confidence and self-assessed skills after simulator-based ultrasound-guided invasive procedure education.67 Web-based resources for ultrasound-guided skills—videos and online instructional modules—have also been used as alternatives to traditional lecture.68
Chest Tubes
In centers with a lower incidence of penetrating trauma, it may be necessary to use task trainers and other alternatives to live patients to ensure that learners are exposed to an adequate number of insertions. Although live animal laboratories were used extensively in the past, these are falling out of favor because of ethical concerns at many institutions. One alternative is to use animal cadavers sacrificed for unrelated research purposes—such cadavers can be obtained by communicating with professionals at one’s home institution who do animal research. Another low-cost solution is to use grocery store pig ribs (Fig. 69-8). Lungs and pleura can be simulated with balloons or bags of saline. One group studied a model that they created and reported that proficiency by advanced trauma life support criteria was achieved by their learners.69 A study of junior doctors in the United Kingdom using the “SuperAnnie” chest tube task trainer showed that the teaching program, designed to teach technical skill before a procedure was first carried out on a patient, was effective in improving confidence and objectively measured skill levels.70

Central Lines
Central line insertion can be taught well with task trainers. Although they cannot simulate complications, an extensive discussion about pneumothorax, wire embolization, and accidental arterial catheterization can be held during teaching of the procedure. In a study of medical residents, central line insertion was taught in a 2-hour session involving didactic instruction, discussion, and training on Blue Phantom task trainers. Learners had significantly improved skills immediately after the session, although the authors did find that the instruction conferred no advantage over traditional learning in the longer term.71 Simulation can also be used to reinforce the use and steps of a central line–associated bloodstream infection prevention checklist to ensure that learning of the procedure is associated from the beginning with proper sterile technique and infection control measures such as hand washing.
Suturing
Even though suturing is one procedure that EM residents and students rotating through the department get plenty of exposure to, novice learners are often more comfortable throwing their first stitches in a simulated environment. Watching an instructional video alone can increase learners’ confidence in their skills,72 and using grocery store animal parts can be a very realistic simulation of human skin. Pigs’ feet and ears are most commonly used, cheap, and widely available. There are also synthetic skin simulators that are especially helpful in teaching advanced suturing skills such as approximating the vermilion border. It is important to discuss wound cleaning, choice of suture, and possible complications in addition to providing technical instruction. Suturing is often taught to large groups of learners, and one interesting study determined the ideal teacher-to-student ratio for suturing to be 1 : 4.73
Incision and Drainage
Incision plus drainage of an abscess is a relatively simple procedure and can easily be taught at the bedside. Abscesses are common, and even an inexperienced operator can perform incision and drainage successfully with appropriate step-by-step guidance. It is helpful to practice on simulation modules, which allows learners to approach the procedure with more confidence. Most simulations involve low-cost models created by instructors out of food-based substances such as tapioca pudding to simulate purulent material under simulated skin. One such model involving a maple syrup– and mayonnaise-filled balloon embedded in a chicken breast was found to be both a sonographically and physically accurate approximation of a typical skin abscess.74
Assessing Procedural Competency
Developing the skills necessary to perform a procedure independently is different for everyone, and successful learning depends on both the quality of each procedural experience and the number of procedures performed.75 If procedures have been taught or practiced incorrectly, experience is not a useful predictor of procedural competency. When a learner performs a manual skill incorrectly, even once, it is much more difficult to relearn the correct technique.22 If procedures are learned incorrectly without the benefit of guidance and remediation, the learner may inevitably take the role of instructor and pass these mistakes on to other learners through the teaching process.76 To avoid this, particularly in the beginning, learners should be observed closely and corrected when mistakes are made. In the words of Red Auerbach, the legendary coach of the Boston Celtics, “Practice does not make perfect; perfect practice makes perfect.”22
The actual number of procedures necessary to ensure competency is unknown. In the case of thoracotomy, a study by Chapman and colleagues failed to show a significant correlation between the clinician’s previous procedural experience and actual performance as assessed by written, computerized, or animal models. Similarly, knowledge of thoracotomy content and procedural steps did not predict procedural competency.77 Typically, the number of procedures performed previously is taken as being predictive of procedural competency. The findings by Chapman and associates, however, suggest that procedural competency cannot be predicted by numbers. Despite these findings, many hospitals use the number of procedures previously performed as a criterion for hospital credentialing and for granting the privilege to perform procedures independently.76 Some surgical residencies have adopted competency-based education and report success with the use of fresh cadavers as models to achieve rapid improvement in surgical skills.78
The EM Residency Review Committee and the Accreditation Council for Graduate Medical Education have devised a broad list of procedures for which competence should be achieved by all EM physicians, and it includes suggested numbers.79,80 It is up to the individual program to choose how to demonstrate and document competency, and no guidelines for this have been outlined. Direct observation, procedure workshops, and simulations are all used, but it is difficult to come up with a reliable, objective method of assessing competency, especially for procedures in which a bad outcome may be delayed. For example, most instructors are aware when a learner has poor intubation skills. Every step of this procedure is visible to an instructor and standardized, and a bad outcome is identifiable immediately. For other procedures, such as incision and drainage or suturing, the instructor may not be present, especially when the learner is more advanced, and a bad outcome would not necessarily be obvious until follow-up, which often does not occur in the ED.
Currently, no competency criteria for emergency procedures and resuscitations have been set by the American Board of Emergency Medicine (ABEM), and a minimum number of procedures has not been established. Nor has the ABEM established a mechanism for testing procedural competency and must rely on residencies to provide the necessary training, evaluation, and assurance of competency.81 Braen and Munger described the early efforts of the ABEM in evaluating procedural skills,81 but these were not implemented, primarily because of a lack of reliable equipment and resources to examine large pools of candidates in a high-stakes national examination. To standardize testing, there must be an assurance that examiners will be able to reliably evaluate candidates. Bullock and colleagues demonstrated good interrater reliability by both expert and nonexpert observers when they were given structured checklists to assess procedural skills.82 Custalow and associates likewise observed excellent interrater reliability among expert reviewers for the evaluation of critical step performance of saphenous vein cutdown, thoracotomy, and cricothyroidotomy.64 Surgical specialties use a variety of scoring systems, including the well-studied Objective Structured Assessment of Technical Skills, to evaluate learners’ proficiency, and perhaps the use of similar tools should be considered for EM.83,84
Ideally, a national procedural competency examination might incorporate animal, cadaver, and virtual reality simulation laboratories to evaluate candidates.85
Online Resources for Procedural Education
The Internet is an invaluable resource for educators and learners on EM procedures. Self-posting websites such as YouTube contain a wealth of videos on nearly every procedure imaginable, some with detailed step-by-step instructions. Many EM residency programs have developed their own bank of procedure websites for either internal or widespread consumption. Standard medical resources, such as the New England Journal of Medicine procedure videos or interactive texts and journal articles available through portals such as MDConsults, are widely available. Websites such as Procedures Consult (www.proceduresconsult.com) provide rich multimedia content that covers a wide variety of procedures and is intended to be used as a primary didactic source or as a refresher at the point of care. Other societies or groups dedicated to specific procedures, such as AirwayWorld (www.airwayworld.com), or general compendia, such as the online Multimedia Procedure Manual (emprocedures.com), are easily accessible at little or no cost. Since adult learners bring a variety of learning styles to each educational encounter, providing trainees with a list of appropriate online resources dedicated to the procedure being taught can lead to more frequent practice and self-directed education throughout the knowledge acquisition process.
References
1. Issenberg, SB, McGaghie, WC, Petrusa, ER, et al. Features and uses of high-fidelity medical simulations that lead to effective learning: a BEME systematic review. Med Teach. 2005;27:10–28.
2. Druck, J, Valley, MA, Lowenstein, SR. Procedural skills training during emergency medicine residency: are we teaching the right things? West J Emerg Med. 2009;10:152.
3. Chapman, DM. Use of computer-based technologies in teaching emergency procedural skills. Acad Emerg Med. 1994;1:404.
4. Reznick, RK, MacRae, H. Teaching surgical skills—changes in the wind. N Engl J Med. 2006;355:2664.
5. Wearne, S. Teaching procedural skills in general practice. Aust Fam Physician. 2011;40:63.
6. Greif, R, Egger, L, Basciani, RM, et al. Emergency skill training—a randomized controlled study on the effectiveness of the 4-stage approach compared to traditional clinical teaching. Resuscitation. 2010;81:1692–1697.
7. Wulf, G, Shea, C, Lewthwaite, R. Motor skill learning and performance: a review of influential factors. Med Educ. 2010;44:75.
8. Kneebone, R. Evaluating clinical simulations for learning procedural skills: a theory-based approach. Acad Med. 2005;80:549.
9. Monrouxe, LV, Reese, CE, Bradley, P. The construction of patients’ involvement in hospital bedside teaching encounters. Qual Health Res. 2009;19:918.
10. Burns, JP, Reardon, FE, Truog, RD. Using newly deceased patients to teach resuscitation procedures. N Engl J Med. 1994;331:1652.
11. Manifold, CA, Storrow, A, Rodgers, K. Patient and family attitudes regarding the practice of procedures on the newly deceased. Acad Emerg Med. 1999;6:110.
12. Breitmeier, D, Schulz, Y, Wilde, N, et al. [Cricothyroidotomy training on cadavers—experiences in the education of medical students, anaesthetists, and emergency physicians.]. Anaesthesiol Intensivmed Notfallmed Schmerzther. 2004;39:94.
13. Alden, AW, Ward, KL, Moore, GP. Should postmortem procedures be practiced on recently deceased patients? A survey of relatives’ attitudes. Acad Emerg Med. 1999;6:749.
14. Goldblatt, AD. Don’t ask, don’t tell: practicing minimally invasive resuscitation techniques on the newly dead. Ann Emerg Med. 1995;25:86.
15. Iserson, KV. Law versus life: the ethical imperative to practice and teach using the newly dead emergency department patient. Ann Emerg Med. 1995;25:91.
16. Moore, GP. Ethics seminars: the practice of medical procedures on newly dead patients—is consent warranted? Acad Emerg Med. 2001;8:389.
17. Reznek, M, Harter, P, Krummel, T. Virtual reality and simulation: training the future emergency physician. Acad Emerg Med. 2002;9:78.
18. Shukla, A, Kline, D, Cherian, A, et al. A simulation course on lifesaving techniques for third-year medical students. Simul Healthc. 2007;2:11.
19. Steadman, RH, Coates, WC, Huang, YM, et al. Simulation-based training is superior to problem-based learning for the acquisition of critical assessment and management skills. Crit Care Med. 2006;34:252.
20. Holcomb, JB, Dumire, RD, Crommett, JW, et al. Evaluation of trauma team performance using an advanced human patient simulator for resuscitation training. J Trauma. 2002;52:1078.
21. Seropian, MA. General concepts in full-scale simulation: getting started. Anesth Analg. 2003;97:1695.
22. Thomas, H, Jr. Teaching procedural skills: beyond “see one—do one.”. Acad Emerg Med. 1994;1:398.
23. Weaver, ME, Kyrouac, JP, Frank, S, et al. A cadaver workshop to teach medical procedures. Med Educ. 1986;20:407.
24. Chapman, DM, Rhee, KJ, Panacek, EA, et al. Cadavers as teachers [letter and response]. Ann Emerg Med. 1997;30:117.
25. Atkinson, RC, Schiffrin, RM. The control of short-term memory. Sci Am. 1971;225:82.
26. Shea CM, Shebilske WL, Worchel S, eds. Motor Learning and Control. Prentice Hall: Upper Saddle River, NJ, 1993:54.
27. Lee, TD, Hirota, TT. Encoding specificity principle in motor short-term memory for movement extent. J Mot Behav. 1980;12:63.
28. Cheong, J. The use of animals in medical education: a question of necessity vs. desirability. Theor Med. 1989;10:53.
29. Lammers, RL, Davenport, M, Korley, F, et al. Teaching and assessing procedural skills using simulation: metrics and methodology. Acad Emerg Med. 2008;15:1079–1087.
30. Plummer, JL, Owen, H. Learning endotracheal intubation in a clinical skills learning center: a quantitative study. Anesth Analg. 2001;93:656–662.
31. Kovacs, G, Bullock, G, Ackroyd-Stolarz, S, et al. A randomized controlled trial on the effect of educational interventions in promoting airway management skill maintenance. Ann Emerg Med. 2000;36:301–309.
32. Langham, TS, Rigby, IJ, Wlaker, IW, et al. Simulation-based training in critical resuscitation procedures improves residents’ competence. CJEM. 2009;11:535–539.
33. Boet, S, Borges, BC, Naik, VN, et al. Complex procedural skills are retained for a minimum of 1 yr after a single high-fidelity simulation training session. Br J Anaesth. 2011;107:533–539.
34. Branney, SW, Moore, EE, Feldhaus, KM, et al. Critical analysis of two decades of experience with postinjury emergency department thoracotomy in a regional trauma center. J Trauma. 1998;45:87–94. [discussion 94-95].
35. Cogbill, TH, Moore, EE, Millikan, JS, et al. Rationale for selective application of emergency department thoracotomy in trauma. J Trauma. 1983;23:453–460.
36. Chang, RS, Hamilton, RJ, Carter, WA. Declining rate of cricothyroidotomy in trauma patients with an emergency medicine residency: implications for skills training. Acad Emerg Med. 1998;5:247.
37. Slagel, SA, Skiendzielewski, JJ, Martyak, GG, et al. Emergency medicine and surgery resident roles on the trauma team: a difference of opinion. Ann Emerg Med. 1986;15:28–32.
38. Gallagher, EJ, Coffey, J, Lombardi, G, et al. Emergency procedures important to the training of emergency medicine residents: who performs them in the emergency department? Acad Emerg Med. 1995;2:630–633.
39. Hayden, SR, Panacek, EA. Procedural competency in emergency medicine: the current range of residency experience. Acad Emerg Med. 1999;6:728.
40. Dire, DJ, Kietzman, LI. A prospective survey of procedures performed by emergency medicine residents during a 36-month residency. J Emerg Med. 1995;13:831.
41. Ray, VG, Garrison, HG. Clinical procedures performed by emergency medicine resident physicians: a computer-based model for documentation. J Emerg Med. 1991;9:157.
42. Wang, EE, Quinones, J, Fitch, MT, et al. Developing technical expertise in emergency medicine—the role of simulation in procedural skill acquisition. Acad Emerg Med. 2008;15:1046–1057.
43. Wong, DT, Prabhu, AJ, Coloma, M, et al. What is the minimum training required for successful cricothyroidotomy? A study in mannequins. Anesthesiology. 2003;98:349–353.
44. Sanchez, LD, Delapena, J, Kelly, SP, et al. Procedure lab used to improve confidence in the performance of rarely performed procedures. Eur J Emerg Med. 2006;13:29–31.
45. Walls, RM, Murphy, MF. Manual of Emergency Airway Management, 3rd ed. Philadelphia: Lippincott, Williams & Wilkins; 2008.
46. Owen, H, Plummer, JL. Improving learning of a clinical skill: the first year’s experience of teaching endotracheal intubation in a clinical simulation facility. Med Educ. 2002;36:635.
47. Goldman, K, Steinfeldt, T. Acquisition of basic fiberoptic intubation skills with a virtual reality airway simulator. J Clin Anesth. 2006;18:173.
48. Kuduvalli, PM, Jervis, A, Tighe, SQ, et al. Unanticipated difficult airway management in anaesthetised patients: a prospective study of the effect of mannequin training on management strategies and skill retention. Anesthesia. 2008;63:364–369.
49. Goldmann, K, Ferson, DZ. Education and training in airway management. Best Pract Res Clin Anaesthesiol. 2005;19:717.
50. Olympio, MA, Whelan, R, Ford, RP, et al. Failure of simulation training to change residents’ management of oesophageal intubation. Br J Anaesth. 2003;91:312–318.
51. Walls, RM, Murphy, MF. Manual of Emergency Airway Management, 3rd ed. Philadelphia: Lippincott, Williams & Wilkins; 2008.
52. Herbstreit, F, Fassbender, P, Haberl, H, et al. Learning endotracheal intubation using a novel videolaryngoscope improves intubation skills of medical students. Anesth Analg. 2011;113:586–590.
53. Roppolo, LP, White, PF, Hatten, B, et al. Use of the TrachView videoscope as an adjunct to direct laryngoscopy for teaching orotracheal intubation. Eur J Emerg Med. 2012;19:196–199.
54. Berg, BW, Vincent, DS, Murray, WB, et al. Videolaryngoscopy for intubation skills training of novice military airway managers. Stud Health Technol Inform. 2009;142:34–36.
55. Boedeker, BH, Hoffman, S, Murray, WB. Endotracheal intubation training using virtual images: learning with the mobile telementoring intubating video laryngoscope. Stud Health Technol Inform. 2007;125:49.
56. Orde, S, Celenza, A, Pinder, M. A randomized trial comparing a 4-stage to 2-stage teaching technique for laryngeal mask insertion. Resuscitation. 2010;81:1687.
57. Ti, LK, Chen, FG, Tan, GM, et al. Experiential learning improves the learning and retention of endotracheal intubation. Med Educ. 2009;43:654–660.
58. Plummer, JL, Owen, H. Learning endotracheal intubation in a clinical skills learning center: a quantitative study. Anesth Analg. 2001;93:656.
59. Lammers, RL, Temple, KJ, Wagner, MJ, et al. Competence of new emergency medicine residents in the performance of lumbar punctures. Acad Emerg Med. 2005;12:622–628.
60. Conroy, SM, Bond, WF, Pheasant, KS, et al. Competence and retention in performance of the lumbar puncture procedure in a task trainer model. Simul Healthc. 2010;5:133–138.
61. Gaies, MG, Morris, SA, Hafler, JP, et al. Reforming procedural skills training for pediatric residents: a randomized, interventional trial. Pediatrics. 2009;124:610–619.
62. Kilbane, BJ, Adler, MD, Trainor, JL. Pediatric residents’ ability to perform a lumbar puncture: evaluation of an educational intervention. Pediatr Emerg Care. 2010;26:558.
63. Sagarin, MJ, Barton, ED, Chng, YM, et al. Airway management by US and Canadian emergency medicine residents: a multicenter analysis of more than 6,000 endotracheal intubation attempts. Ann Emerg Med. 2005;46:328–336.
64. Custalow, CB, Kline, JA, Marx, JA, et al. Emergency department resuscitative procedures: animal laboratory training improves procedural competency and speed. Acad Emerg Med. 2002;9:575–586.
65. Hill, C, Reardon, R, Joing, S, et al. Cricothyrotomy technique using gum elastic bougie is faster than standard technique: a study of emergency medicine residents and medical students in an animal lab. Acad Emerg Med. 2010;17:666–669.
66. John, B, Suri, I, Hillermann, C, et al. comparison of cricothyroidotomy on manikin vs. simulator: a randomized cross-over study. Anaesthesia. 2007;2:1029–1032.
67. Woo, MY, Frank, J, Lee, AC, et al. Effectiveness of a novel training program for emergency medicine residents in ultrasound-guided insertion of central venous catheters. CJEM. 2009;11:343–348.
68. Chenkin, J, Lee, S, Huynh, T, et al. Procedures can be learned on the Web: a randomized study of ultrasound-guided vascular access training. Acad Emerg Med. 2008;15:949–954.
69. Ching, AC, Wachtel, TL. A simple device to teach tube thoracostomy. J Trauma. 2011;69:1564.
70. Hutton, IA, Kenealy, H, Wong, C. Using simulation models to teach junior doctors how to insert chest tubes: a brief and effective teaching module. Intern Med J. 2008;38:887.
71. Smith, C, Huang, GC, Newman, LR, et al. Simulation training and its effect on long-term resident performance in central venous catheterization. Simul Healthc. 2010;5:146.
72. Sudhir A, Plautz, C, Woods WA. A novel approach to “see one, do one”: video instruction for suturing workshops [abstract D42:6]. Presented at the Sixth European Congress on Emergency Medicine, Stockholm, 2010.
73. Dubrowski, A, MacRae, H. Randomised, controlled study investigating the optimal instructor:student ratios for teaching suturing skills. Med Educ. 2006;40:59–63.
74. Heiner, JD. A new simulation model for skin abscess identification and management. Simul Healthc. 2010;5:238–241.
75. Hayden, SR, Panacek, EA. Procedural competency in emergency medicine: the current range of residency experience. Acad Emerg Med. 1999;6:728.
76. Chapman, DM, Cavanaugh, SH. Using receiver operating characteristics (ROC) analysis to establish the previous experience threshold for critical-procedural competency. Acad Med. 1996;71:S7.
77. Chapman, DM, Marx, JA, Honigman, B, et al. Emergency thoracotomy: comparison of medical student, resident, and faculty performances on written, computer, and animal-model assessments. Acad Emerg Med. 1994;1:373.
78. Martin, M, Vashisht, B, Frezza, E, et al. Competency-based instruction in critical invasive skills improves both resident performance and patient safety. Surgery. 1998;124:313.
79. 2007 Model of the Clinical Practice of Emergency Medicine. Available online at http://www.acgme.org/acWebsite/RRC_110/110_clinModel.pdf. [Accessed August 2011].
80. Accreditation Council for Graduate Medical Education. Emergency Medicine Guidelines—Procedures and Resuscitations. Available online at http://www.acgme.org/acWebsite/RRC_110/110_guidelines.asp. [Accessed August 2011].
81. Braen, GR, Munger, BS. Evaluation of procedural skills [commentary]. Acad Emerg Med. 1994;1:325.
82. Bullock, G, Kovacs, G, Macdonald, K, et al. Evaluating procedural skills competence: inter-rater reliability of expert and non-expert observers. Acad Med. 1999;74:76.
83. Martin, JA, Regehr, G, Reznick, R, et al. Objective structured assessment of technical skills (OSATS) for surgical residents. Br J Surg. 1997;84:273.
84. Khan, MS, Bann, SD, Darzi, AW, et al. Assessing surgical skill using bench station models. Plast Reconstr Surg. 2007;120:793–800.
85. Chapman, DM. Definitively defining the specialty of emergency medicine: issues of procedural competency. Acad Emerg Med. 1999;6:678.