[level-membership-for-dermatology-category]
Dermatomyositis

Specific investigations








First-line therapies
 Sunscreens
Sunscreens Topical corticosteroids
Topical corticosteroids Antimalarials – hydroxychloroquine or chloroquine
Antimalarials – hydroxychloroquine or chloroquine Combination antimalarial therapy
Combination antimalarial therapy Systemic corticosteroids
Systemic corticosteroids Immunosuppressive agents – methotrexate, azathioprine
Immunosuppressive agents – methotrexate, azathioprine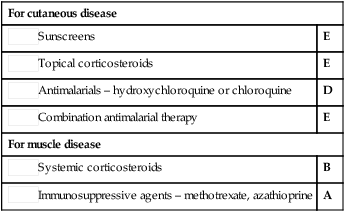
Second-line therapies
 Topical calcineurin inhibitors (tacrolimus or pimecrolimus)
Topical calcineurin inhibitors (tacrolimus or pimecrolimus) Methotrexate
Methotrexate Mycophenolate mofetil
Mycophenolate mofetil Intravenous immunoglobulin
Intravenous immunoglobulin Other immunosuppressive agents – cyclophosphamide, chlorambucil, mycophenolate mofetil, cyclosporine, tacrolimus
Other immunosuppressive agents – cyclophosphamide, chlorambucil, mycophenolate mofetil, cyclosporine, tacrolimus Intravenous immunoglobulin
Intravenous immunoglobulin Rituximab
Rituximab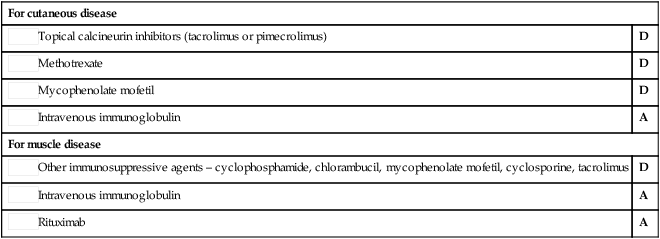
Third-line therapies
 Dapsone for cutaneous disease
Dapsone for cutaneous disease Thalidomide for cutaneous disease
Thalidomide for cutaneous disease Anti-estrogen medication for cutaneous disease
Anti-estrogen medication for cutaneous disease Diltiazem for calcinosis
Diltiazem for calcinosis Etanercept
Etanercept Infliximab
Infliximab Total body irradiation
Total body irradiation Rituximab for cutaneous disease
Rituximab for cutaneous disease Leflunomide
Leflunomide Sirolimus
Sirolimus Stem cell transplantation
Stem cell transplantation[/level-membership-for-dermatology-category][not-level-membership-for-dermatology-category]
Dermatomyositis
Specific investigations
Buy Membership for Dermatology Category to continue reading. Learn more here
[/not-level-membership-for-dermatology-category]
