[level-membership-for-basic-science-category]
Chapter 12 Cough, Cold, and Allergy
Antitussives




Moa (Mechanism of Action)
 Antitussives are cough suppressants. There are two ways to inhibit coughing: centrally and peripherally.
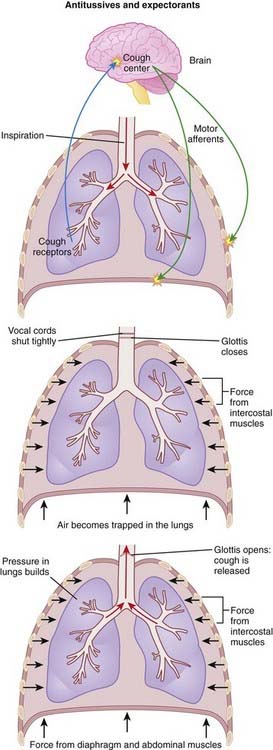
Antitussives are cough suppressants. There are two ways to inhibit coughing: centrally and peripherally. Cough is normally produced through the stimulation of sensory receptors of the glossopharyngeal and vagus nerves, innervating the mucous membranes of the lower pharynx, larynx, trachea, and smaller airways of the respiratory system. The receptors then transmit the signal to the cough center in the brain, which then triggers a reflex motor response that results in contraction of the muscles to close the glottis (vocal cords) and contraction of the muscles of expiration. The result is a sudden increase in intrathoracic pressure, followed by relaxation of the vocal cords, resulting in rapid expulsion of air (Figure 12-1).
Cough is normally produced through the stimulation of sensory receptors of the glossopharyngeal and vagus nerves, innervating the mucous membranes of the lower pharynx, larynx, trachea, and smaller airways of the respiratory system. The receptors then transmit the signal to the cough center in the brain, which then triggers a reflex motor response that results in contraction of the muscles to close the glottis (vocal cords) and contraction of the muscles of expiration. The result is a sudden increase in intrathoracic pressure, followed by relaxation of the vocal cords, resulting in rapid expulsion of air (Figure 12-1).









Important Notes
 Dextromethorphan was developed in an attempt to create a cough suppressant with the efficacy of codeine but with none of the central nervous system (CNS) side effects such as euphoria. Dextromethorphan therefore has little or no ability to induce euphoria and therefore is available without a prescription and without pharmacist consultation in most jurisdictions.
Dextromethorphan was developed in an attempt to create a cough suppressant with the efficacy of codeine but with none of the central nervous system (CNS) side effects such as euphoria. Dextromethorphan therefore has little or no ability to induce euphoria and therefore is available without a prescription and without pharmacist consultation in most jurisdictions.







Evidence
Over-the-Counter Preparations for Acute Cough
 A 2008 Cochrane review (25 trials, N = 3492 participants) assessed the effects of over-the-counter (OTC) cough preparations for acute cough. Six trials in adults had variable results for antitussives versus placebo. Of the two trials involving expectorants, one showed benefit versus placebo whereas the other did not. In children, antitussives (two trials), antihistamines (two trials), antihistamine-decongestant combinations (two trials), and antitussive-bronchodilator combinations were no more effective than placebo. No trials were found of expectorants, but one trial showed benefit of a mucolytic versus placebo.
A 2008 Cochrane review (25 trials, N = 3492 participants) assessed the effects of over-the-counter (OTC) cough preparations for acute cough. Six trials in adults had variable results for antitussives versus placebo. Of the two trials involving expectorants, one showed benefit versus placebo whereas the other did not. In children, antitussives (two trials), antihistamines (two trials), antihistamine-decongestant combinations (two trials), and antitussive-bronchodilator combinations were no more effective than placebo. No trials were found of expectorants, but one trial showed benefit of a mucolytic versus placebo.

Expectorants


Moa (Mechanism of Action)










Important Notes



Evidence
Over-the-Counter Preparations for Acute Cough
 A 2008 Cochrane review (25 trials, N = 3492 participants) assessed the effects of OTC cough preparations for acute cough. Of the two trials involving expectorants, one showed benefit versus placebo whereas the other did not. In children, no trials were found of expectorants, but one trial showed benefit of a mucolytic versus placebo.
A 2008 Cochrane review (25 trials, N = 3492 participants) assessed the effects of OTC cough preparations for acute cough. Of the two trials involving expectorants, one showed benefit versus placebo whereas the other did not. In children, no trials were found of expectorants, but one trial showed benefit of a mucolytic versus placebo.
Decongestants




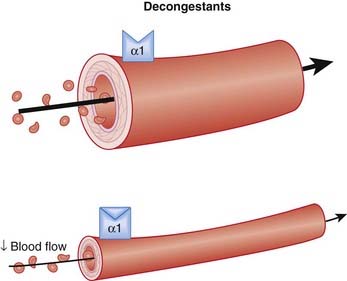
Moa (Mechanism of Action) (Figure 12-2)







Pharmacokinetics



Contraindications
 Concomitant use with monoamine oxidase inhibitors (MAOIs): Monoamine oxidase breaks down amines such as norepinephrine. Concomitant use of MAOIs with indirect-acting decongestants such as pseudoephedrine that increase norepinephrine can lead to excess norepinephrine and hypertensive crisis. MOAIs are used to treat depression and are not commonly used because newer agents have replaced them.
Concomitant use with monoamine oxidase inhibitors (MAOIs): Monoamine oxidase breaks down amines such as norepinephrine. Concomitant use of MAOIs with indirect-acting decongestants such as pseudoephedrine that increase norepinephrine can lead to excess norepinephrine and hypertensive crisis. MOAIs are used to treat depression and are not commonly used because newer agents have replaced them.
Side Effects









Important Notes
 Rhinitis medicamentosa is an uncomfortable complication of topical decongestant use. However, because it is a simple pharmacodynamic phenomenon, patients should inevitably improve once receptor densities have returned to their predrug state. This typically takes 1 to 2 weeks, and in the intervening period the patient may benefit from oral decongestants to get through the periods of severe congestion.
Rhinitis medicamentosa is an uncomfortable complication of topical decongestant use. However, because it is a simple pharmacodynamic phenomenon, patients should inevitably improve once receptor densities have returned to their predrug state. This typically takes 1 to 2 weeks, and in the intervening period the patient may benefit from oral decongestants to get through the periods of severe congestion.

Evidence
Nasal Congestion in the Common Cold
 A 2009 Cochrane review (seven trials, all in adults) assessed the efficacy of nasal decongestants in reducing symptoms of nasal congestion in adults and children with the common cold. There was a 6% decrease in subjective symptoms after a single oral dose of decongestant versus placebo. From a clinical standpoint, this is a small difference. With repeated use over 3 to 5 days, the benefit decreased to 4%. Only two trials reported safety measures, but in these two trials there was a small increased risk of insomnia versus placebo.
A 2009 Cochrane review (seven trials, all in adults) assessed the efficacy of nasal decongestants in reducing symptoms of nasal congestion in adults and children with the common cold. There was a 6% decrease in subjective symptoms after a single oral dose of decongestant versus placebo. From a clinical standpoint, this is a small difference. With repeated use over 3 to 5 days, the benefit decreased to 4%. Only two trials reported safety measures, but in these two trials there was a small increased risk of insomnia versus placebo.FYI Notes
 Ephedrine is structurally related to the amphetamines. The main difference from a pharmacologic perspective is that ephedrine and pseudoephedrine have less effect on the CNS. Ephedrine is also used to raise heart rate and blood pressure, most commonly in anesthetized patients. It is given intravenously for this indication.
Ephedrine is structurally related to the amphetamines. The main difference from a pharmacologic perspective is that ephedrine and pseudoephedrine have less effect on the CNS. Ephedrine is also used to raise heart rate and blood pressure, most commonly in anesthetized patients. It is given intravenously for this indication.


H1 Antagonists




Moa (Mechanism of Action)
 Histamine is mainly synthesized in mast cells and basophils of the immune system, enterochromaffin-like cells in gastric mucosa, and certain neurons that release it as a neurotransmitter.
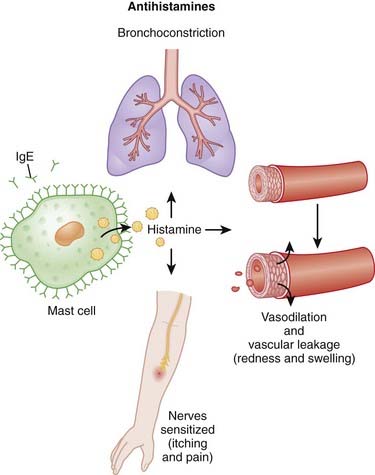
Histamine is mainly synthesized in mast cells and basophils of the immune system, enterochromaffin-like cells in gastric mucosa, and certain neurons that release it as a neurotransmitter. Histamine plays a key role in allergic reactions, also known as immunoglobulin E (IgE)–mediated hypersensitivity reactions. The role of histamine in the immune response is largely mediated by H1 receptors. Classic hallmarks of an immune response that is mediated by H1 include the following (Figure 12-3):
Histamine plays a key role in allergic reactions, also known as immunoglobulin E (IgE)–mediated hypersensitivity reactions. The role of histamine in the immune response is largely mediated by H1 receptors. Classic hallmarks of an immune response that is mediated by H1 include the following (Figure 12-3):






Pharmacokinetics









Side Effects


Important Notes
 Two factors appear to play a role in distinguishing sedating from nonsedating antihistamines. Aside from the pharmacokinetic property of being able to cross into the CNS, some antihistamines also antagonize serotonin (5-HT2) receptors. For the agents that cross into the CNS, this contributes further to their sedating properties.
Two factors appear to play a role in distinguishing sedating from nonsedating antihistamines. Aside from the pharmacokinetic property of being able to cross into the CNS, some antihistamines also antagonize serotonin (5-HT2) receptors. For the agents that cross into the CNS, this contributes further to their sedating properties.





Evidence
For the Common Cold
 A 2003 Cochrane review (32 trials, N = 8930 participants) assessed the effects of antihistamines in reducing nasal symptoms in patients with common cold. First-generation antihistamines were found to have a small effect on rhinorrhea and sneezing, but this was not considered to be clinically significant. First-generation agents also were associated with the side effect of sedation. Combinations of antihistamines and decongestants were not found to be effective in young children.
A 2003 Cochrane review (32 trials, N = 8930 participants) assessed the effects of antihistamines in reducing nasal symptoms in patients with common cold. First-generation antihistamines were found to have a small effect on rhinorrhea and sneezing, but this was not considered to be clinically significant. First-generation agents also were associated with the side effect of sedation. Combinations of antihistamines and decongestants were not found to be effective in young children.





Mast Cell Stabilizers


Moa (Mechanism of Action)
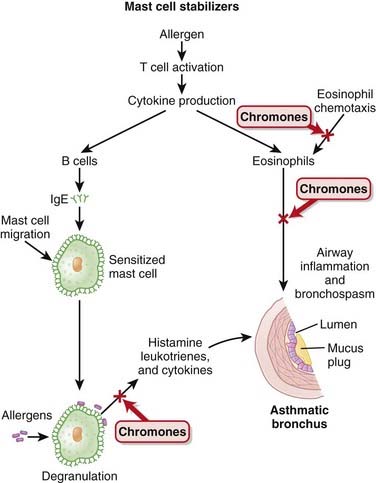
 The degranulation of mast cells and eosinophils is an important step in the response to an allergen. Degranulation leads to release of a variety of proinflammatory factors, including histamine, leukotrienes, and various cytokines. These factors then act on tissues to elicit the classic signs of an allergic reaction.
The degranulation of mast cells and eosinophils is an important step in the response to an allergen. Degranulation leads to release of a variety of proinflammatory factors, including histamine, leukotrienes, and various cytokines. These factors then act on tissues to elicit the classic signs of an allergic reaction.













Evidence
Sodium Cromoglycate versus Placebo in Pediatric Asthma
 A 2008 Cochrane review (23 trials, N = 1026 participants) examined the efficacy of sodium cromoglycate versus placebo in prophylactic treatment of pediatric asthma. Most of the studies had small sample sizes, and most were crossover studies, thus limiting confidence in the results. The authors concluded that there is insufficient evidence to be certain about the beneficial effects of sodium cromoglycate for this indication and in this population.
A 2008 Cochrane review (23 trials, N = 1026 participants) examined the efficacy of sodium cromoglycate versus placebo in prophylactic treatment of pediatric asthma. Most of the studies had small sample sizes, and most were crossover studies, thus limiting confidence in the results. The authors concluded that there is insufficient evidence to be certain about the beneficial effects of sodium cromoglycate for this indication and in this population.Sodium Cromoglycate versus Inhaled Corticosteroids in Chronic Asthma
 A 2006 Cochrane review (17 trials, N = 1279 children; eight trials, N = 321 adults) compared inhaled corticosteroids with sodium cromoglycate in adults and children with chronic asthma. In children and adults, sodium cromoglycate was inferior to inhaled corticosteroids with respect to use of rescue bronchodilators and improved performance on pulmonary function tests. Sodium cromoglycate was also inferior with respect to improvement of symptoms, although in adults these improvements were significant only in crossover trials and not in those of parallel design. There were no differences in adverse effects between inhaled corticosteroids and sodium cromoglycate in either children or adults.
A 2006 Cochrane review (17 trials, N = 1279 children; eight trials, N = 321 adults) compared inhaled corticosteroids with sodium cromoglycate in adults and children with chronic asthma. In children and adults, sodium cromoglycate was inferior to inhaled corticosteroids with respect to use of rescue bronchodilators and improved performance on pulmonary function tests. Sodium cromoglycate was also inferior with respect to improvement of symptoms, although in adults these improvements were significant only in crossover trials and not in those of parallel design. There were no differences in adverse effects between inhaled corticosteroids and sodium cromoglycate in either children or adults.
[/level-membership-for-basic-science-category][not-level-membership-for-basic-science-category]
Chapter 12 Cough, Cold, and Allergy
Antitussives
Moa (Mechanism of Action)
Antitussives are cough suppressants. There are two ways to inhibit coughing: centrally and peripherally. Cough is normally produced through the stimulation of sensory receptors of the glossopharyngeal and vagus nerves, innervating the mucous membranes of the lower pharynx, larynx, trachea, and smaller airways of the respiratory system. The receptors then transmit the signal to the cough center in the brain, which then triggers a reflex motor response that results in contraction of the muscles to close the glottis (vocal cords) and contraction of the muscles of expiration. The result is a sudden increase in intrathoracic pressure, followed by relaxation of the vocal cords, resulting in rapid expulsion of air (Figure 12-1).Important Notes
Dextromethorphan was developed in an attempt to create a cough suppressant with the efficacy of codeine but with none of the central nervous system (CNS) side effects such as euphoria. Dextromethorphan therefore has little or no ability to induce euphoria and therefore is available without a prescription and without pharmacist consultation in most jurisdictions.Evidence
Over-the-Counter Preparations for Acute Cough
A 2008 Cochrane review (25 trials, N = 3492 participants) assessed the effects of over-the-counter (OTC) cough preparations for acute cough. Six trials in adults had variable results for antitussives versus placebo. Of the two trials involving expectorants, one showed benefit versus placebo whereas the other did not. In children, antitussives (two trials), antihistamines (two trials), antihistamine-decongestant combinations (two trials), and antitussive-bronchodilator combinations were no more effective than placebo. No trials were found of expectorants, but one trial showed benefit of a mucolytic versus placebo.Expectorants
Moa (Mechanism of Action)
Important Notes
Evidence
Over-the-Counter Preparations for Acute Cough
A 2008 Cochrane review (25 trials, N = 3492 participants) assessed the effects of OTC cough preparations for acute cough. Of the two trials involving expectorants, one showed benefit versus placebo whereas the other did not. In children, no trials were found of expectorants, but one trial showed benefit of a mucolytic versus placebo.Buy Membership for Basic Science Category to continue reading. Learn more here
[/not-level-membership-for-basic-science-category]
