Combined spinal-epidural blockade
Applied anatomy
The essence of a CSE block is single-shot administration of intrathecal anesthetic or analgesic agents along with placement of a catheter into the epidural space. The applied anatomy of a CSE block is the same as that for subarachnoid and epidural blockade (see Chapter 123, Epidural Anesthesia, Figure 123-1).
Contraindications
Contraindications for CSE block are the same as those for all neuraxial blocks (Table 124-1).
Table 124-1
Absolute and Relative Contraindications to Neuraxial Anesthesia/Analgesia
| Absolute | Relative |
| Patient refusal Bacteremia/sepsis Increased intracranial pressure Infection at needle insertion site Shock or severe hypovolemia Coagulopathy or therapeutic anticoagulation* |
Preexisting neurologic disease Severe psychiatric disease or dementia Aortic stenosis Left ventricular outflow tract obstruction Various congenital heart conditions (absolute contraindication if severe) Deformities or previous surgery of the spinal column |











Equipment and technique
CSE blockades are typically performed via a needle-through-needle technique with traditional epidural and spinal needles (Figure 124-1). When the needle-through-needle technique is performed, a sterile field is created at the procedure site, the skin and subcutaneous tissue are infiltrated with a local anesthetic agent, and an epidural needle is inserted into the ligamentum flavum. Loss of resistance with air or saline is used to identify the epidural space. A spinal needle is then advanced through the epidural needle into the subarachnoid space. The spinal needle must be longer than the epidural needle to allow dural puncture, projecting 13 to 17 mm beyond the tip of the epidural needle. Following the appearance of cerebrospinal fluid, the intrathecal anesthetic or analgesic agent is injected, and the spinal needle is removed. Finally, a catheter is advanced through the epidural needle into the epidural space, and the epidural needle is removed.
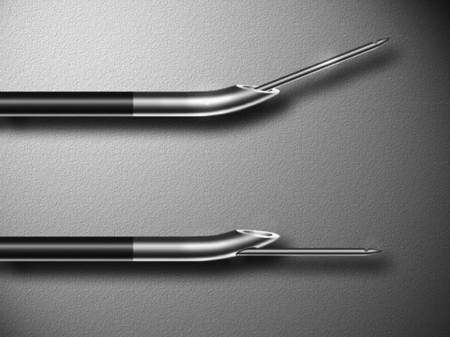
Other CSE techniques include the use of specially designed CSE epidural needles that include a guide for the spinal needle alongside the outer wall of the epidural needle or a guide incorporated into the epidural needle wall (Figure 124-1). These guided needles make it possible to place an epidural catheter before intrathecally administering drugs. However, many anesthesiologists believe that these specially designed needles offer little advantage.





