CHAPTER 115 Basic Principles of Cranial Surgery for Brain Tumors
Preoperative Evaluation and Management
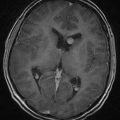
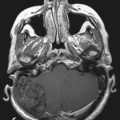
Preoperative Imaging Interpretation
Timing of Surgery
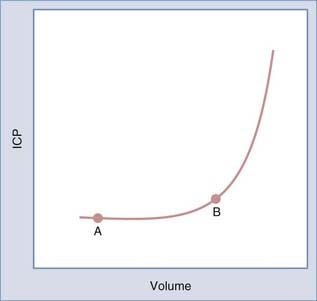
The timing of surgery is dictated by the type of symptoms and their pace. Progressive symptoms over a short period indicate that the tumor and edema are expanding faster than the brain is able to compensate. Recognition of this situation is critical because such patients are at risk for rapid deterioration. The Monro-Kellie principle, introduced to neurosurgery by Cushing, states that changes in brain volume cause reciprocal changes in the blood and cerebrospinal fluid (CSF) compartments within the rigid cranial sphere to maintain intracranial pressure (ICP) within a normal range.1 As brain volume increases secondary to a mass such as a tumor, a compensatory decrease in CSF or blood volume occurs to maintain ICP within the normal range. As the tumor expands, ICP increases slowly until there is no further displaceable volume (i.e., CSF or blood). At this point, further increases in brain volume result in an accelerated increase in ICP. The relationship between volume and pressure is depicted by the volume-pressure curve in Figure 115-1. As a tumor grows and expands, a patient moves along the curve from point A to point B. During this time, compensatory changes occur, including displacement of CSF and blood, as well as compression of normal brain tissue, to maintain ICP in the normal range. At point B, the ability of the brain to further compensate is limited. Thus, a small additional increase in volume results in a larger increase in pressure. It is important to recognize patients who are approaching point B on the volume-pressure curve because they are at risk for a rapid increase in ICP with small additional increases in volume. This rapid increase in ICP can lead to rapid neurological decline.


Surgical Preparation
In general, patients respond within 24 hours of beginning steroid treatment. This clinical improvement parallels the increased compliance measured in patients 24 hours after beginning steroids. Investigative studies in patients and animals indicate that dexamethasone decreases tumor capillary permeability and tumor blood volume.2–4 These actions alter the configuration of the volume-pressure curve such that further increases in tumor volume result in a smaller increase in ICP.
Positioning
Positioning is an important but often overlooked part of the surgical procedure. The four body positions are supine, lateral, prone, and sitting. Sitting is rarely used today. In the past, the sitting position was used primarily for pineal tumors, but it has now been replaced by the prone Concorde position (see Chapter 126 for pineal tumors).
 A frontotemporal craniotomy is a standard approach to intrinsic tumors located in the frontal or temporal lobes. It is also used for tumors in the suprasellar area and the anterior skull base. A modification of this approach is the orbitozygomatic or modified orbitozygomatic approach, which removes the orbital rim to facilitate access to the skull base and minimize brain retraction. The patient is positioned according to the principles stated earlier: a relaxed neck to promote venous drainage, elevation of the head above the level of the heart to promote venous drainage, and turning of the head so that the approach to an intrinsic tumor is perpendicular to the floor. For tumors in the suprasellar area, the head is positioned so that the neck is extended about 30 degrees from the axis of the cervical spine, which results in the malar eminence being the highest point in the field. This position allows gravity to pull the frontal lobes away from the skull base and thus reduces the amount of retraction necessary to expose the suprasellar area.
A frontotemporal craniotomy is a standard approach to intrinsic tumors located in the frontal or temporal lobes. It is also used for tumors in the suprasellar area and the anterior skull base. A modification of this approach is the orbitozygomatic or modified orbitozygomatic approach, which removes the orbital rim to facilitate access to the skull base and minimize brain retraction. The patient is positioned according to the principles stated earlier: a relaxed neck to promote venous drainage, elevation of the head above the level of the heart to promote venous drainage, and turning of the head so that the approach to an intrinsic tumor is perpendicular to the floor. For tumors in the suprasellar area, the head is positioned so that the neck is extended about 30 degrees from the axis of the cervical spine, which results in the malar eminence being the highest point in the field. This position allows gravity to pull the frontal lobes away from the skull base and thus reduces the amount of retraction necessary to expose the suprasellar area. Parietal-occipital craniotomy allows exposure of the entire parietal lobe, the posterior temporal lobe, and the occipital lobe. Tumors located in the parietal-occipital area are best approached with this craniotomy. In addition, intraventricular tumors located in the posterior horn of the ventricle, as well as thalamic tumors, are approached with this craniotomy. The patient is positioned in the lateral position on a beanbag with an axillary roll. The head is positioned so that the approach to the tumor is perpendicular to the floor. For lateral parietal tumors, the head should be neutral with the long axis of the body. For occipital tumors, the head should be turned toward the floor. For approaches to ventricular and periventricular tumors, the head is bent toward the ipsilateral shoulder to bring the superior parietal lobule to the highest point in the field.
Parietal-occipital craniotomy allows exposure of the entire parietal lobe, the posterior temporal lobe, and the occipital lobe. Tumors located in the parietal-occipital area are best approached with this craniotomy. In addition, intraventricular tumors located in the posterior horn of the ventricle, as well as thalamic tumors, are approached with this craniotomy. The patient is positioned in the lateral position on a beanbag with an axillary roll. The head is positioned so that the approach to the tumor is perpendicular to the floor. For lateral parietal tumors, the head should be neutral with the long axis of the body. For occipital tumors, the head should be turned toward the floor. For approaches to ventricular and periventricular tumors, the head is bent toward the ipsilateral shoulder to bring the superior parietal lobule to the highest point in the field. Intra-axial and extra-axial tumors located in the parasagittal region are approached with this craniotomy. This is also the craniotomy for intraventricular tumors in the anterior horn and body of the lateral ventricle, as well as for tumors located in the region of the foramen of Monro and third ventricle.
Intra-axial and extra-axial tumors located in the parasagittal region are approached with this craniotomy. This is also the craniotomy for intraventricular tumors in the anterior horn and body of the lateral ventricle, as well as for tumors located in the region of the foramen of Monro and third ventricle. This approach is used for tumors located in the fourth ventricle, in the vermis, or in the pineal region. The exposed cerebellum includes a portion of both cerebellar hemispheres, so a tumor located medially in the cerebellar hemisphere could also be approached with this craniotomy.
This approach is used for tumors located in the fourth ventricle, in the vermis, or in the pineal region. The exposed cerebellum includes a portion of both cerebellar hemispheres, so a tumor located medially in the cerebellar hemisphere could also be approached with this craniotomy.
Tumor Removal
Intraoperative adjuvants that facilitate maximal safe surgical resection include intraoperative navigation with frameless stereotactic systems, intraoperative ultrasonography, and intraoperative MRI. These tools provide imaging feedback that the surgeon can use to evaluate the extent of resection. These tools should be used as adjuvants to complement the visual feedback that the surgeon is receiving from the gross appearance of the tumor. 5-Aminolevulinic acid (5-ALA) is a fluorescent marker that accumulates in malignant glioma tissue and can be used to evaluate the extent of resection. Intraoperative use of this marker guides the tumor resection such that studies have demonstrated more complete glioma resection, based on postoperative MRI, when 5-ALA was used than when it was not used.5
Cushing H. Studies in Intracranial Physiology and Surgery. London: Oxford University Press; 1926. 19-23
Leenders KL, Beaney RP, Brooks DJ, et al. Dexamethasone treatment of brain tumor patients: effects on regional cerebral blood flow, blood volume, and oxygen utilization. Neurology. 1985;35:1610-1616.
Tonn JC, Stummer W. Fluorescence-guided resection of malignant gliomas using 5-aminolevulinic acid: practical use, risks, and pitfalls. Clin Neurosurg. 2008;55:20-26.
Yamada K, Bremer AM, West CR. Effects of dexamethasone on tumor-induced brain edema and its distribution in the brain of monkeys. J Neurosurg. 1979;50:361-367.
Yamada K, Ushio Y, Hayakawa T, et al. Effects of methylprednisolone on peritumoral brain edema. J Neurosurg. 1983;59:612-619.
1 Cushing H. Studies in Intracranial Physiology and Surgery. London: Oxford University Press; 1926. 19-23
2 Yamada K, Ushio Y, Hayakawa T, et al. Effects of methylprednisolone on peritumoral brain edema. J Neurosurg. 1983;59:612-619.
3 Leenders KL, Beaney RP, Brooks DJ, et al. Dexamethasone treatment of brain tumor patients: effects on regional cerebral blood flow, blood volume, and oxygen utilization. Neurology. 1985;35:1610-1616.
4 Yamada K, Bremer AM, West CR. Effects of dexamethasone on tumor-induced brain edema and its distribution in the brain of monkeys. J Neurosurg. 1979;50:361-367.
5 Tonn JC, Stummer W. Fluorescence-guided resection of malignant gliomas using 5-aminolevulinic acid: practical use, risks, and pitfalls. Clin Neurosurg. 2008;55:20-26.