[level-membership-for-surgery-category]
CHAPTER 15 Appendectomy
Case Study
A 19-year-old male presents to the emergency room complaining of severe right-sided lower abdominal pain, nausea, and anorexia, which began 24 hours earlier. On physical examination, he has a fever of 100.5°F. His abdomen is focally tender on palpation of the right lower quadrant. His white blood cell count is within the normal range. A computed tomography (CT) scan of the abdomen and pelvis shows a thickened appendix and periappendiceal inflammation (Fig. 15-1).
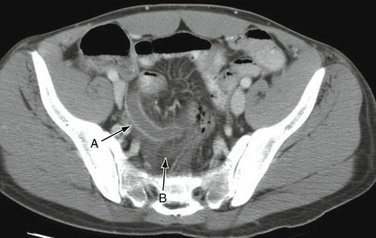
Figure 15-1 Computed tomography scan showing a thickened appendix (A) and adjacent inflammation (B).
(From Rakel RE [ed]: Textbook of Family Medicine, 7th ed. Philadelphia, Saunders, 2007, courtesy of Dr. Perry Pernicano, Department of Radiology, University of Michigan Medical School, Ann Arbor, MI.)
BACKGROUND
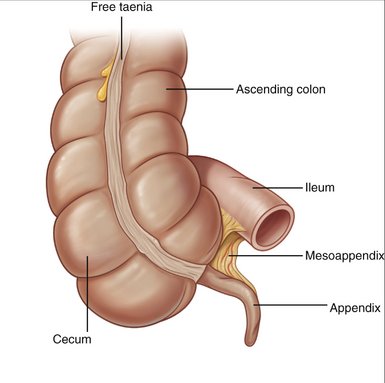
The appendix is a blind-ended tubular structure arising from the cecum approximately 2 cm below the ileocecal valve (Fig. 15-2). Obstruction of the lumen of the appendix by fecal material (i.e., fecalith), a tumor, or lymphoid hyperplasia may result in elevated intraluminal pressures, vascular congestion, stasis, bacterial overgrowth, and inflammation. Without intervention, the resulting appendicitis may progress to wall necrosis and appendiceal perforation. Prompt diagnosis and management are critical to the successful treatment of appendicitis. Despite the high incidence of appendicitis, however, its diagnosis is not always straightforward. The differential diagnosis of appendicitis is broad and may include gastroenteritis, Meckel’s diverticulitis, colonic diverticulitis, inflammatory bowel disease, urinary tract infection, epididymitis, and gastrointestinal and reproductive tract malignancies. Women of childbearing age who present with abdominal pain pose a particular diagnostic challenge because pelvic inflammatory disease, ovarian cysts, and ovarian torsion can also mimic appendicitis.
INDICATIONS FOR SURGERY
PREOPERATIVE EVALUATION
COMPONENTS OF THE PROCEDURE AND APPLIED ANATOMY
Preoperative Considerations
Open Appendectomy
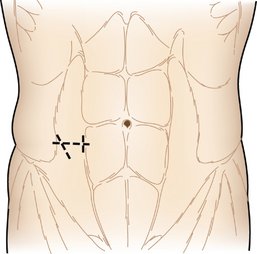
Figure 15-5 Common incisions for open appendectomy (dashed lines).
(From Ortega JM, Ricardo AE: Surgery of the appendix and colon. In Moody FG [ed]: Atlas of Ambulatory Surgery. Philadelphia, WB Saunders, 1999.)
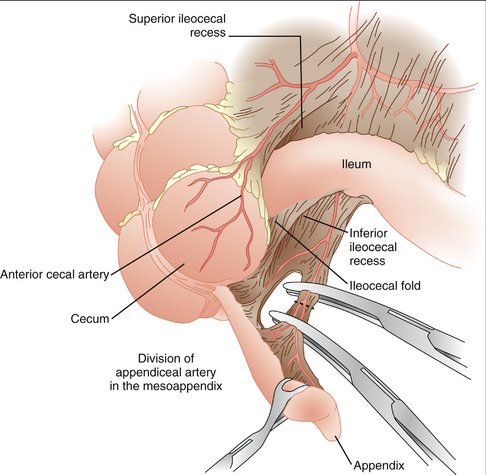
Figure 15-6 Division of the mesoappendix.
(From Ortega JM, Ricardo AE: Surgery of the appendix and colon. In Moody FG [ed]: Atlas of Ambulatory Surgery. Philadelphia, WB Saunders, 1999.)
Laparoscopic Appendectomy
Additional Considerations
COMPLICATIONS
Lally KP, Cox CS, Andrassy RJ. Appendix. In Townsend CM, Beauchamp RD, Evers BM, Mattox KL, editors: Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice, 17th ed, Philadelphia: Saunders, 2004.
Paulson EK, Kalady MF, Pappas TN. Clinical practice: suspected appendicitis. N Engl J Med. 2003;348:236-242.
[/level-membership-for-surgery-category][not-level-membership-for-surgery-category]
CHAPTER 15 Appendectomy
Case Study
A 19-year-old male presents to the emergency room complaining of severe right-sided lower abdominal pain, nausea, and anorexia, which began 24 hours earlier. On physical examination, he has a fever of 100.5°F. His abdomen is focally tender on palpation of the right lower quadrant. His white blood cell count is within the normal range. A computed tomography (CT) scan of the abdomen and pelvis shows a thickened appendix and periappendiceal inflammation (Fig. 15-1).
Figure 15-1 Computed tomography scan showing a thickened appendix (A) and adjacent inflammation (B).
(From Rakel RE [ed]: Textbook of Family Medicine, 7th ed. Philadelphia, Saunders, 2007, courtesy of Dr. Perry Pernicano, Department of Radiology, University of Michigan Medical School, Ann Arbor, MI.)
BACKGROUND
The appendix is a blind-ended tubular structure arising from the cecum approximately 2 cm below the ileocecal valve (Fig. 15-2). Obstruction of the lumen of the appendix by fecal material (i.e., fecalith), a tumor, or lymphoid hyperplasia may result in elevated intraluminal pressures, vascular congestion, stasis, bacterial overgrowth, and inflammation. Without intervention, the resulting appendicitis may progress to wall necrosis and appendiceal perforation. Prompt diagnosis and management are critical to the successful treatment of appendicitis. Despite the high incidence of appendicitis, however, its diagnosis is not always straightforward. The differential diagnosis of appendicitis is broad and may include gastroenteritis, Meckel’s diverticulitis, colonic diverticulitis, inflammatory bowel disease, urinary tract infection, epididymitis, and gastrointestinal and reproductive tract malignancies. Women of childbearing age who present with abdominal pain pose a particular diagnostic challenge because pelvic inflammatory disease, ovarian cysts, and ovarian torsion can also mimic appendicitis.
