CHAPTER 14 Pancreatic Resection
Case Study
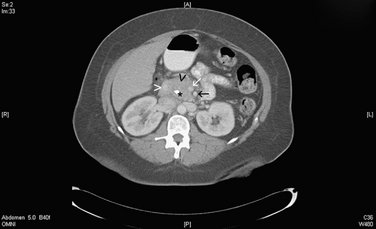
A 65-year-old male is referred to a surgeon for evaluation of a pancreatic mass. He reports a 2-month history of progressive jaundice, anorexia, and loss of 15 pounds. Additionally, he notes intermittent dull upper abdominal pain, light-colored stools, and tea-colored urine. He was recently seen by a gastroenterologist and underwent endoscopic retrograde cholangiopancreatography (ERCP), which showed narrowing of the distal common bile duct and pancreatic duct; a biliary stent was placed during the procedure. A subsequent computed tomography (CT) scan of the abdomen and pelvis showed a mass in the head of the pancreas without evidence of metastases or vascular encasement or invasion (Fig. 14-1).
INDICATIONS FOR PANCREATIC RESECTION
PREOPERATIVE EVALUATION
COMPONENTS OF PANCREATIC RESECTION AND APPLIED ANATOMY
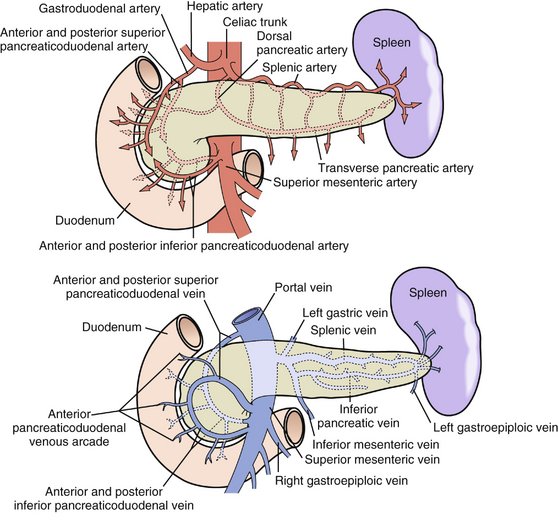
Figure 14-3 Arterial supply (top) and venous drainage (bottom) of the pancreas and duodenum.
(From Skandalakis JE, Gray SW, Rowe JS Jr, et al: Anatomical complications of pancreatic surgery. Contemp Surg 15:17–50, 1979. Reprinted with permission.)
Preoperative Considerations
Whipple Procedure
Distal Pancreatectomy
Additional Operative Considerations
COMPLICATIONS
Brugge WR, Lauwers GY, Sahani D, et al. Cystic neoplasms of the pancreas. N Engl J Med. 2004;351:1218-1226.
Steer ML. Exocrine pancreas. In: Townsend CM, Beauchamp RD, Evers BM, Mattox KL, editors. Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice. 17th ed. Philadelphia: Saunders; 2004:1667-1674.
Thayer SP, Warshaw AL. Periampullary cancer. In: Cameron JL, editor. Current Surgical Therapy. 8th ed. Philadelphia: Elsevier Mosby; 2004:494-504.