[level-membership-for-surgery-category]
CHAPTER 16 Colectomy
BACKGROUND
There are many indications for both partial and total colectomy. These include malignant, benign, ischemic, inflammatory, and infectious processes. The most common indications for colon and rectal resection are addressed individually later in the chapter. Common terms used to describe the types of colon and rectal operations are described in Table 16-1.
| Type of Resection | Description |
|---|---|
| Segmental colectomy | Removal of a portion of the colon (e.g., right, transverse, left, or sigmoid). |
| Total abdominal colectomy | Removal of the entire abdominal colon, leaving the rectum and creation of an end ileostomy or ileorectal anastomosis. |
| End stoma | Intestinal diversion involving division and exteriorization of the colon (colostomy) or terminal ileum (ileostomy) through the skin. The distal colon is then either brought out as a mucous fistula or left in the abdomen as a Hartmann’s pouch. |
| Loop stoma | A loop of either colon or ileum is exteriorized and opened, but not divided. |
| Hartmann’s pouch | An end stoma is created from proximal bowel; distal bowel is closed and remains in the pelvis. |
| Ileal pouch–anal anastomosis (Park’s pouch, J-pouch) | After total proctocolectomy, the terminal ileum is used to create a reservoir that is connected to the anus as a “neorectum.” |
| Total mesorectal excision | En bloc removal of the mesorectum along with the rectum for rectal cancers of the mid and distal rectum. This is carried out by dissection in the plane between the fascia propria of the rectum and the presacral fascia. |
| Low anterior resection | Resection of the upper rectum; an anastomosis is formed between the colon and distal rectum. |
| Abdominoperineal resection | Total mesorectal excision of the rectum, surrounding tissues, and lymph nodes via abdominal and perineal approaches; creation of an end stoma. |
| Total proctocolectomy | Removal of the entire colon and rectum. Ileoanal pouch reconstruction or end ileostomy is required. |
INDICATIONS FOR COLORECTAL RESECTION
PREOPERATIVE EVALUATION
COMPONENTS OF THE PROCEDURE AND APPLIED ANATOMY
Preoperative Considerations
Open Right Hemicolectomy
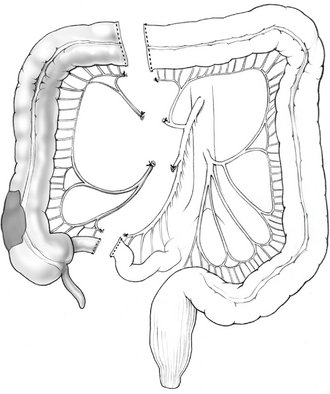
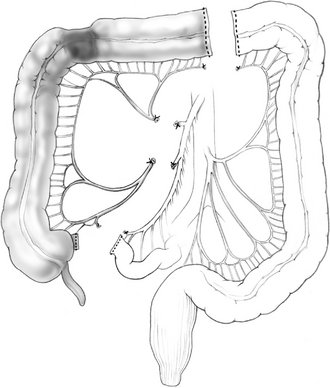
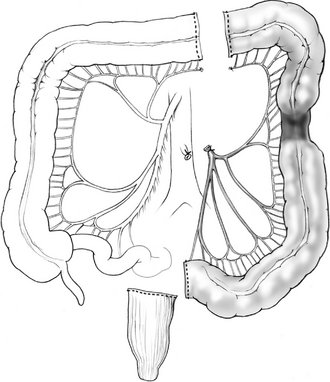
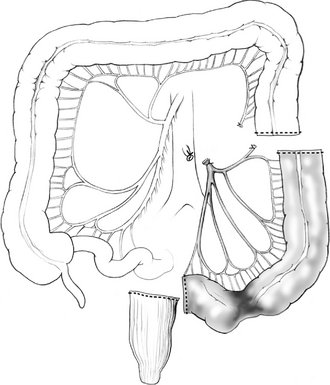
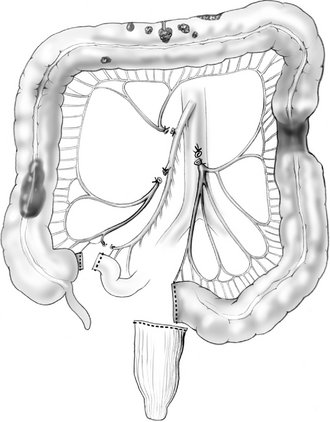
Figure 16-1 Right hemicolectomy.
(From Cameron JL [ed]: Current Surgical Therapy, 7th ed. Philadelphia, Mosby, 2001.)
Other Operative Procedures
POSTOPERATIVE COURSE
COMPLICATIONS
[/level-membership-for-surgery-category][not-level-membership-for-surgery-category]
CHAPTER 16 Colectomy
BACKGROUND
There are many indications for both partial and total colectomy. These include malignant, benign, ischemic, inflammatory, and infectious processes. The most common indications for colon and rectal resection are addressed individually later in the chapter. Common terms used to describe the types of colon and rectal operations are described in Table 16-1.
| Type of Resection | Description |
|---|---|
| Segmental colectomy | Removal of a portion of the colon (e.g., right, transverse, left, or sigmoid). |
| Total abdominal colectomy | Removal of the entire abdominal colon, leaving the rectum and creation of an end ileostomy or ileorectal anastomosis. |
| End stoma | Intestinal diversion involving division and exteriorization of the colon (colostomy) or terminal ileum (ileostomy) through the skin. The distal colon is then either brought out as a mucous fistula or left in the abdomen as a Hartmann’s pouch. |
| Loop stoma | A loop of either colon or ileum is exteriorized and opened, but not divided. |
| Hartmann’s pouch | An end stoma is created from proximal bowel; distal bowel is closed and remains in the pelvis. |
| Ileal pouch–anal anastomosis (Park’s pouch, J-pouch) | After total proctocolectomy, the terminal ileum is used to create a reservoir that is connected to the anus as a “neorectum.” |
| Total mesorectal excision | En bloc removal of the mesorectum along with the rectum for rectal cancers of the mid and distal rectum. This is carried out by dissection in the plane between the fascia propria of the rectum and the presacral fascia. |
| Low anterior resection | Resection of the upper rectum; an anastomosis is formed between the colon and distal rectum. |
| Abdominoperineal resection | Total mesorectal excision of the rectum, surrounding tissues, and lymph nodes via abdominal and perineal approaches; creation of an end stoma. |
| Total proctocolectomy | Removal of the entire colon and rectum. Ileoanal pouch reconstruction or end ileostomy is required. |
