[level-membership-for-opthalmology-category]
Chapter 52 Acquired Retinal Macroaneurysms
Clinical description
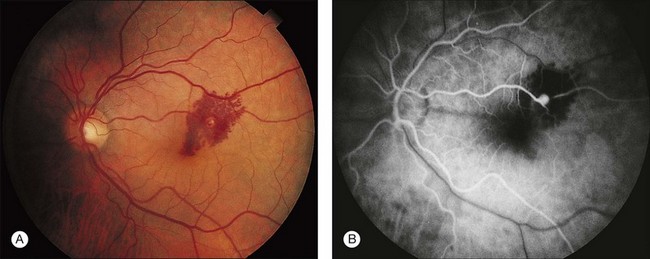
Acquired retinal macroaneurysms are fusiform or round dilations of the retinal arterioles that occur in the posterior fundus within the first three orders of arteriolar bifurcation. Often they are located at the site of an arteriolar bifurcation or an arteriovenous crossing (Fig. 52.1). The supratemporal artery is the most commonly reported site of involvement because patients with such involvement are more likely to have visual impairment. Women make up the majority of reported cases. Most cases are unilateral, while 10% may be bilateral. Retinal macroaneurysm was estimated to occur in 1 in 9000 in the Beijing Eye Study.1
Most commonly, retinal macroaneurysm affects patients in the sixth and seventh decades of life. Often associated are vascular problems such as hypertension and general arteriosclerotic cardiovascular disease, as noted by Robertson,2 who first coined the term retinal macroaneurysm. Uncontrolled hypertension can present with a retinal artery macroaneurysm and its accompanying vitreous hemorrhage.3 Other investigators have confirmed this association with hypertension.4 Serum lipid and lipoprotein abnormalities have also been reported in patients with this condition.5 Systemic investigations for hypertension and cardiovascular disease should be conducted in patients who have a retinal arteriolar macroaneurysm.
Although a patient with a retinal arteriolar macroaneurysm may be asymptomatic if the macula is not involved (Fig. 52.2), the most common clinical symptom is decline in central visual acuity as a result of retinal edema, exudation, or hemorrhage.6 Bleeding from macroaneurysms can occur in the subretinal space, into the retina, beneath the internal limiting membrane, or into the vitreous. So-called hourglass hemorrhages are typical. Hemorrhage in the space beneath the retinal pigment epithelium may produce a dark lesion simulating an ocular tumor such as malignant melanoma,7 or a lesion associated with age-related macular degeneration. A complication of the vitreous hemorrhage also includes the development of angle closure glaucoma.8

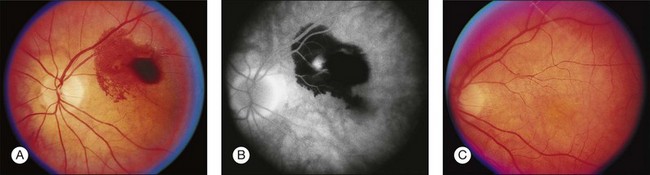
The hemorrhage may also partially or completely obscure the aneurysm (Fig. 52.3). Occasionally, multiple macroaneurysms occur. Other retinal microvascular changes associated with macroaneurysms include widening of the periarterial capillary-free zone around the area of the aneurysm, capillary dilation and nonperfusion, microaneurysms, and artery-to-artery collaterals.
Diagnosis of retinal macroaneurysm
Fluorescein angiography initially may fail to demonstrate the macroaneurysm because of blockage by the surrounding hemorrhage. Dense hemorrhage in the retina can cause marked hypofluorescence. In such cases of dense hemorrhage, indocyanine green angiography may be useful because its absorption and emission peak in the near-infrared range allow the light to penetrate the hemorrhage to a greater extent than fluorescein angiography.9 A small case series using indocyanine green angiography has demonstrated these lesions to be pulsatile and contiguous with the arterial wall, pathognomonic of an insolated retinal artery macroaneurysm.10 The macroaneurysm typically fills in the early arterial phase of the angiogram. The appearance of the late phase of the fluorescein angiogram varies, ranging from little staining of the vessel wall to marked leakage. Leakage of surrounding dilated capillaries also may be seen. The lipid often present in the macular area fails to block fluorescein unless the amount of lipid is massive. Macular hole formation following rupture of a retinal arterial macroaneurysm has been reported.11,12
Evaluation of the retinal structure with optical coherence tomography was conducted in a series of patients with retinal macroaneurysm.13 Although most of the retinal structure was intact at the initial exam, subretinal hemorrhage or extensive exudative changes from retinal macroaneurysm can cause the deterioration of the foveal outer photoreceptor layer with a poor visual outcome.
Natural course and treatment of retinal macroaneurysms
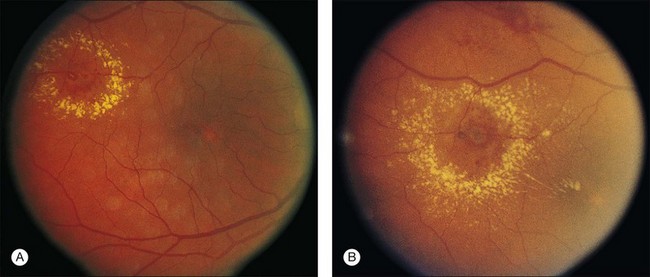
Several series have reported on the natural history and treatment response of macroaneurysms.5,14,15 The yellow dye laser has been considered for treatment because of its theoretical advantages.16 Some investigators believe the visual prognosis is excellent in most patients who have macroaneurysms and do not have treatment because the lesions can thrombose and undergo spontaneous involution with clearing of the macular exudate.2 However, the exudative process may progress in some patients and cause structural damage to the macula with loss of vision (Fig. 52.4).17 Moderate visual loss also may occur if bleeding causes secondary morphologic changes in the macula. No clear indication for treatment with laser photocoagulation has been established, and the beneficial effects of such treatments have not been proven.
Vitrectomy was performed for clearing the macular hemorrhage associated with the rupture of a macroaneurysm.18 The results of vitrectomy are variable depending on the location of the hemorrhage from the retinal macroaneurysms. The vision is particularly poor in those patients who have dense submacular hemorrhage.19
Pneumatic displacement with or without tissue plasminogen activator has also been used for the therapy of submacular hemorrhage associated with a macroaneurysms.20 Yag laser has also been used to treat such premacular hemorrhage.21 The surgical excision of the retinal macroaneruysm with scissors and diathermy followed by the drainage of the submacular hemorrhage was also explored in 2 cases, with some improvement in vision.22
The differential diagnoses of retinal macroaneurysms include other retinal vascular abnormalities, including diabetic retinopathy, retinal telangiectasia, retinal capillary angioma, cavernous hemangioma, malignant melanoma,7 and the hemorrhagic pigment epithelial detachment of age-related macular degeneration.23
1 Xu L, Wang Y, Jonas JB. Frequency of retinal macroaneurysm in adult Chinese, Beijing Eye Study. Br J Ophthalmol. 2007;91:840–841.
2 Robertson DM. Macroaneurysms of the retinal arteries. Trans Am Acad Ophthalmol Otolaryngol. 1973;77:55–67.
3 Sekuri C, Kayikcioglu M, Kaykcioglu O. Retinal artery macroaneurysm as initial presentation of hypertension. Int J Cardiol. 2004;93:87–88.
4 Moosavi RA, Fong KCS, Chopdar A. Retinal artery macroaneurysms: clinical and fluorescein angiographic features in 34 patients. Eye. 2006;20:1011–1020.
5 Cleary PE, Kohner EM, Hamilton AM, et al. Retinal macro-aneurysms. Br J Ophthalmol. 1975;59:355–361.
6 Rabb MF, Gagliano DA, Teske MP. Retinal arterial macro-aneurysms. Surv Ophthalmol. 1988;33:73–96.
7 Fritsche PL, Flipsen E, Polak BC. Subretinal hemorrhage from retinal arterial macroaneurysm simulating malignancy. Arch Ophthalmol. 2000;118:1704–1705.
8 Arthur SN, Mason J, Roberts B, et al. CA. Secondary acute angle-closure glaucoma associated with vitreous hemorrhage after ruptured retinal arterial macroaneurysm. Am J Ophthalmol. 2004;138:682–683.
9 Townsend-Pico WA, Meyers SM, Lewis H. Indocyanine green angiography in the diagnosis of retinal arterial macroaneurysms associated with submacular and preretinal hemorrhages: a case series. Am J Ophthalmol. 2000;129:33–37.
10 Schneider U, Wagner AL, Kreissig I. Indocyanine green videoangiography of hemorrhagic retinal arterial macroaneurysms. Ophthalmologica. 1997;211:115–118.
11 Mitamura Y, Terashima H, Takeuchi S. Macular hole formation following rupture of retinal arterial macroaneurysm. Retina. 2002;22:113–115.
12 Sato R, Yasukawa T, Hirano Y, et al. Early-onset macular holes following ruptured retinal arterial macroaneurysms. Graefes Arch Clin Exp Ophthalmol. 2008;246:1779–1782.
13 Tsujikawa A, Sakamoto A, Ota M, et al. Retinal structural changes associated with retinal arterial macroaneurysm examined with optical coherence tomography. Retina. 2009;29:782–792.
14 Abdel-Khalek MN, Richardson J. Retinal macroaneurysm: natural history and guidelines for treatment. Br J Ophthalmol. 1986;70:2–11.
15 Lewis RA, Norton EWD, Gass JDM. Acquired arterial macro-aneurysms of the retina. Br J Ophthalmol. 1976;60:21–30.
16 Mainster MA, Whitacre MM. Dye yellow photocoagulation of retinal arterial macroaneurysms. Am J Ophthalmol. 1988;105:97–98.
17 Yang CS, Tsai DC, Lee FL, et al. Retinal arterial macroaneurysms: risk factors of poor visual outcome. Ophthalmologica. 2005;219:366–372.
18 Zhao P, Hayashi H, Oshima K, et al. Vitrectomy for macular hemorhage associated with retinal arterial macroanerusym. Ophthalmol. 2000;107:613–617.
19 Nakamura H, Hayakawa K, Sawguchi S, et al. Visual outcome after vitreous, sub-internal limiting membrane, and/or submacular hemorrhage removal associated with ruptured retinal arterial macroaneurysms. Graefes Arch Lin Exp Ophthalmol. 2008;246:661–669.
20 Mizutani T, Yasukawa T, Ito Y, et al. Pneumatic displacement of submacular hemorrhage with or without tissue plasminogen activator. Graefes Arch Clin Exp Ophthalmol. 2011;249:1153–1157.
21 Dahreddine M, Eldirani H, Mutsinzi E. Retinal macroaneurysm complicated by premacular hemorrhage: treatment by YAG laser disruption. J Fr Ophthalmol. 2011;34:131.
22 Oie Y, Emi K. Surgical excision of retinal macroaneurysms with submacular hemorrhage. Jpn J Ophthalmol. 2006;50:550–553.
23 Hochman MA, Seery CM, Zarbin MA. Pathophysiology and management of subretinal hemorrhage. Surv Ophthalmol. 1997;42:195–213.
[/level-membership-for-opthalmology-category][not-level-membership-for-opthalmology-category]
Chapter 52 Acquired Retinal Macroaneurysms
Clinical description
Acquired retinal macroaneurysms are fusiform or round dilations of the retinal arterioles that occur in the posterior fundus within the first three orders of arteriolar bifurcation. Often they are located at the site of an arteriolar bifurcation or an arteriovenous crossing (Fig. 52.1). The supratemporal artery is the most commonly reported site of involvement because patients with such involvement are more likely to have visual impairment. Women make up the majority of reported cases. Most cases are unilateral, while 10% may be bilateral. Retinal macroaneurysm was estimated to occur in 1 in 9000 in the Beijing Eye Study.1
Most commonly, retinal macroaneurysm affects patients in the sixth and seventh decades of life. Often associated are vascular problems such as hypertension and general arteriosclerotic cardiovascular disease, as noted by Robertson,2 who first coined the term retinal macroaneurysm. Uncontrolled hypertension can present with a retinal artery macroaneurysm and its accompanying vitreous hemorrhage.3 Other investigators have confirmed this association with hypertension.4 Serum lipid and lipoprotein abnormalities have also been reported in patients with this condition.5 Systemic investigations for hypertension and cardiovascular disease should be conducted in patients who have a retinal arteriolar macroaneurysm.
Although a patient with a retinal arteriolar macroaneurysm may be asymptomatic if the macula is not involved (Fig. 52.2), the most common clinical symptom is decline in central visual acuity as a result of retinal edema, exudation, or hemorrhage.6 Bleeding from macroaneurysms can occur in the subretinal space, into the retina, beneath the internal limiting membrane, or into the vitreous. So-called hourglass hemorrhages are typical. Hemorrhage in the space beneath the retinal pigment epithelium may produce a dark lesion simulating an ocular tumor such as malignant melanoma,7 or a lesion associated with age-related macular degeneration. A complication of the vitreous hemorrhage also includes the development of angle closure glaucoma.8
The hemorrhage may also partially or completely obscure the aneurysm (Fig. 52.3). Occasionally, multiple macroaneurysms occur. Other retinal microvascular changes associated with macroaneurysms include widening of the periarterial capillary-free zone around the area of the aneurysm, capillary dilation and nonperfusion, microaneurysms, and artery-to-artery collaterals.
