Chapter 173 Vertebroplasty and Kyphoplasty
Indications and Techniques
Before the introduction of vertebroplasty and kyphoplasty, treatment of compression fractures consisted of bed rest, pain control (with nonsteroidal anti-inflammatory medications, calcitonin, and narcotics), and back bracing.1 This regimen is often effective, and most people eventually find relief from their pain as the fracture heals. However, a substantial number fail to heal within 3 to 6 weeks. These people often suffer persistent back pain and a risk of gradually worsening kyphotic deformity. Even in those whose compression fractures heal over time, the recovery period is time consuming, requiring at least several weeks. The experience is often profoundly unpleasant and can be marked by periods of insufficient pain control, delirium, and constipation. Such patients are sometimes bedridden, with the attendant risks of deep venous thrombosis, pulmonary embolism, and pneumonia. The prolonged immobility accelerates bone resorption and predisposes the patient to additional injury. Finally, the long-term effects of even a healed fracture may be substantial: kyphotic deformity, decreased lung capacity, and altered forces on intervertebral discs and facet joints.
The vertebroplasty procedure was introduced in France in 1984 by a group that used the technique to treat symptomatic vertebral hemangiomas.2 They found that the “internal casting” provided by polymethyl methacrylate (PMMA) injected into the pathologic vertebral body provided substantial pain relief. This success led to expansion of the procedure to the treatment of pain from myeloma and metastatic neoplasms of the vertebrae3; these indications remain the most common ones for the use of vertebroplasty in Europe. In 1993, the technique was introduced in the United States,4 where its chief use has been to treat the pain from osteoporotic compression fractures. Kyphoplasty was introduced in 1999 as the proprietary technology of Kyphon Inc. Kyphoplasty differs from vertebroplasty by adding the insertion and inflation of a balloon before cement delivery. It has the added goal of restoring vertebral body height and spine alignment.5 Both procedures are now practiced throughout the world, with the number of procedures and practitioners (including radiologists, orthopedic surgeons, neurosurgeons, and anesthesiologists) growing rapidly.
Contraindications
In addition, specific fracture features do not represent absolute contraindications but substantially increase the risk or technical difficulty of the procedure. Disruption of the posterior cortex increases the risk of posterior cement leakage and therefore the risk of spinal cord or nerve root compression; this feature is rare in osteoporotic compression fractures but frequent in burst fractures and metastatic neoplasm. Substantial canal narrowing (without clinical evidence of myelopathy or radiculopathy) increases the risk that even a small amount of cement leakage will produce neurologic compromise. Marked loss of vertebral body height makes the procedure more difficult since there may be little space for needle placement. Poor visualization of osseous structures on fluoroscopy increases the risk of improper needle placement and symptomatic cement leakage but can be overcome with the use of computed tomography (CT). Treatment of patients whose fractures have these features should only be performed by the most experienced practitioners.
Preprocedure Evaluation
History
The classic symptoms from an acute vertebral compression fracture include deep pain with sudden onset, midline location, and exacerbation by motion and standing. These fractures may occur with little or no trauma. The pain often diminishes little in the first week and then fades gradually over the next several weeks to 3 months.1 Lateral radiation may be present, but persistent radiation of the pain in a radiculopathic pattern is rare. When there is substantial kyphosis, patients may also suffer from difficulty breathing, anterior chest wall pain, and gastrointestinal discomfort.
Physical Examination
The practitioner should perform a directed physical examination. This examination includes inspection of the back, palpation for focal areas of tenderness, and correlation of the site of pain with anatomic landmarks. In difficult cases, examination of the sites of pain and tenderness can be performed with fluoroscopic assistance to localize the pain to specific anatomic structures. Although point tenderness at the spinous process of the fractured vertebra is the typical finding in unhealed compression fractures, the absence of typical focal tenderness does not preclude the presence of such a fracture. Imaging is a more reliable test than this portion of the physical examination.6 Assessment of lower extremity neurologic function is especially important in patients with symptoms suggestive of myelopathy, radiculopathy, or spinal stenosis. Evaluation of the heart and lungs is necessary for the safe use of sedation for the procedure.
Imaging
Imaging of the spine is undertaken in all cases to confirm the clinical diagnosis and to plan the procedure. Radiographs are the imaging study of choice for the initial imaging evaluation (Fig. 173-1). Anteroposterior (AP) and lateral views should be obtained. This study allows the practitioner to confirm the presence of fracture, determine the location of fractures, assess the degree of height loss and kyphosis, and identify anatomic variants. Whenever possible, comparison to prior studies is valuable. A single radiograph almost never allows the practitioner to distinguish a new or unhealed fracture from a chronic, healed fracture. With prior radiographs (“old gold”) for comparison, new compression fractures can be identified. If serial radiographs taken several weeks apart show a new compression fracture in a patient with classic history and symptoms, no further imaging may be necessary. However, since back pain is a difficult diagnostic problem, most patients benefit from advanced imaging.

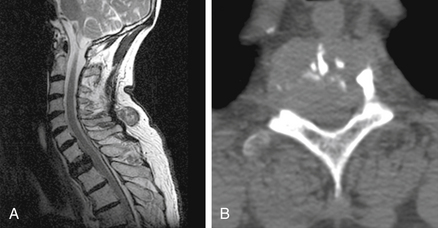
Magnetic resonance imaging (MRI) is the test of choice for this additional evaluation. The main goals of MRI are to (1) distinguish new or unhealed fractures from healed fractures, (2) identify other causes of pain, and (3) evaluate the risk of symptomatic cement leakage during the procedure. For these purposes, the most useful sequence is a T2-weighted sequence with fat suppression. We prefer using inversion recovery (i.e., a short tau inversion time recovery, or STIR, sequence) to achieve the fat suppression, since it is less prone to artifact than frequency-selective fat saturation techniques. On these MRI sequences, recent or unhealed fractures show a hyperintense signal within the bone marrow (Fig. 173-2). This signal may be present in poorly marginated areas filling much of the vertebral body or as discrete curvilinear fracture clefts. In contrast, healed fractures have a marrow signal similar to that of unfractured vertebra. These sequences also provide an adequate evaluation of the spinal canal and show most alternative causes of pain that might mimic fracture. Additional imaging with a sagittal T1-weighted sequence and axial T1- and T2-weighted images may be helpful. In most patients with a typical clinical history and physical examination for osteoporotic compression fracture, the STIR sequence alone is adequate, and the practitioner can reserve the full set of MRI sequences for patients whose pain is atypical or who have STIR abnormalities that require clarification. We have found value in obtaining an additional MRI shortly before the procedure when either (1) there has been worsening of the patient’s pain since the initial evaluation or (2) the imaging study used for the initial evaluation is more than 3 months old.7

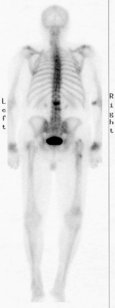
In patients who cannot tolerate MRI (e.g., those with a pacemaker), bone scan is the test of choice. Bone scan does not provide any evaluation of the soft tissues or spinal canal, but it does allow the differentiation of healed and recent fractures. The recent fractures take up the injected technetium 99m–medronate tracer in much higher concentrations (Fig. 173-3). The relative sensitivity and specificity of bone scan and MRI for this purpose have not been established.
CT is not necessary for most osteoporotic compression fractures but is useful for preprocedure evaluation of burst fractures and metastases. In these circumstances, there may be substantial loss of integrity of the posterior vertebral body cortex (Fig. 173-4). This loss increases the risk of the procedure, specifically the risk of posterior leakage of cement or posterior displacement of bone or tumor.8 CT provides the best means for assessing this cortex. CT is also the test of choice for postprocedure evaluation of unexpected symptoms (see the later section on risks).
Procedure: Vertebroplasty
Sedation
Analgesia is necessary to perform vertebroplasty and kyphoplasty safely and with minimal discomfort. This process begins with the informed consent. Fully informing the patient of what to expect in the operating room or procedure suite facilitates patient comfort, cooperation, and satisfaction. Satisfactory analgesia usually can then be achieved with local anesthetics and moderate sedation, but in some cases general endotracheal anesthesia is needed. Vertebroplasty has generally been performed with moderate sedation, while kyphoplasty has more commonly been performed with general anesthesia. At our institution, both are usually performed using moderate sedation with intravenous midazolam and fentanyl. Continuous patient monitoring is performed with electrocardiography, blood pressure measurement, and pulse oximetry. The drug delivery and monitoring are performed by certified nursing personnel. In patients with substantial preexisting respiratory or cardiac disease, an anesthesiologist is asked to evaluate the patient and determine whether monitored anesthesia care is warranted.
Patient Positioning
The ideal patient position for thoracic and lumbar procedures is prone. This position allows the practitioner to place the needle from either side and simplifies positioning of the biplane fluoroscopy unit or C-arm. Furthermore, this position and proper cushion support maximize extension of the fractured segments, promoting kyphosis reduction.9 Although the patient can be rotated slightly, substantial patient angulation can make this a more difficult procedure. A special table and cushions may be used to support the head and body, but good results can be achieved with a flat fluoroscopy table and careful placement of cushions. The patient’s arms should be placed sufficiently toward the head to keep them out of the path of the fluoroscope. Patients can usually be placed in the prone position despite their painful compression fracture. If necessary, moderate sedation can be initiated before the patient is moved. Care must be taken when transferring aged or osteoporotic patients, since transfer alone may cause new fractures.
Needle Placement
For either approach, there are two image guidance strategies. The “end-on” approach uses fluoroscope angulation to place the barrel of the pedicle cortex over the target site in the vertebra body. This view simplifies trajectory planning and is the simplest way of preventing the needle from violating the medial cortex of the pedicle. Alternatively, the AP approach may be used. This view may be easier to achieve with some fluoroscopy systems and in some cases provides superior delineation of the pedicle margins. Once an approach has been selected, the skin is anesthetized with a small amount of subcutaneous lidocaine or bupivacaine. Following the planned needle trajectory, the periosteum is anesthetized in a similar fashion. The planned trajectory can be assessed and adjusted from fluoroscopic views of this smaller needle at the bone surface. A small nick is made in the skin, and an 11- or 13-gauge needle is placed.
End-on Technique
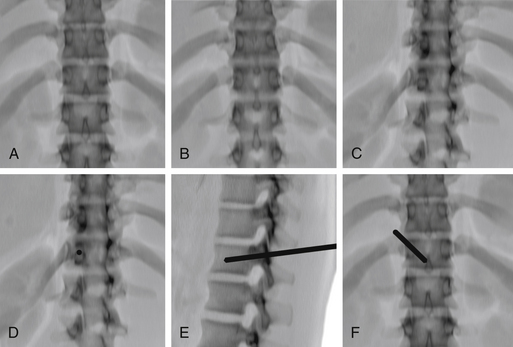
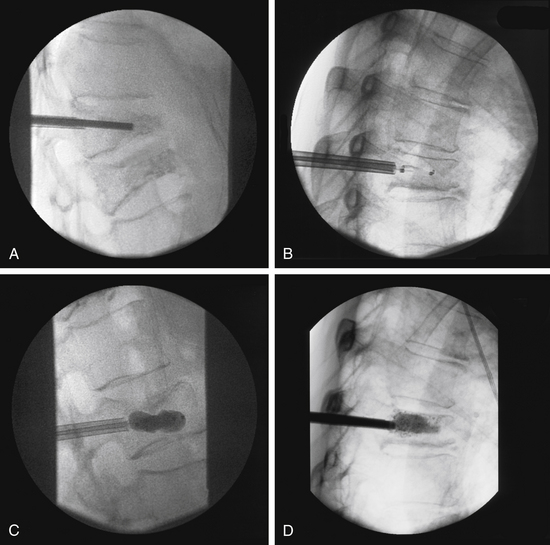
For the end-on technique, the operator rotates the fluoroscopy unit into an ipsilateral oblique view that places the fluoroscopy beam and needle tract perfectly parallel to each other (Fig. 173-5). The image intensifier is first rotated to a true AP position, aligning the spinous process midway between the pedicles. The craniocaudal angulation is changed to bring the pedicles to the midportion of the vertebral body. The image intensifier is then rotated to bring the ipsilateral pedicle so that its medial cortex is at the middle third of the vertebral body. This rotation can only be continued as long as the medial cortex of the pedicle remains clearly visible. The needle is placed so that it is “end on” to the image intensifier and appears as a small circle or ellipse. Once the needle has been advanced to the bone surface, small corrections in the craniocaudal angulation can be made using a true lateral view (care is needed to angle this view so that the pedicles project over each other). The needle is then advanced through the pedicle, maintaining the end-on appearance of the needle. Once the needle has traversed the pedicle, it is advanced using the lateral view to the junction of the anterior and middle thirds of the vertebral body.
AP Technique
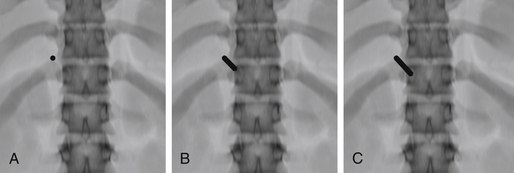
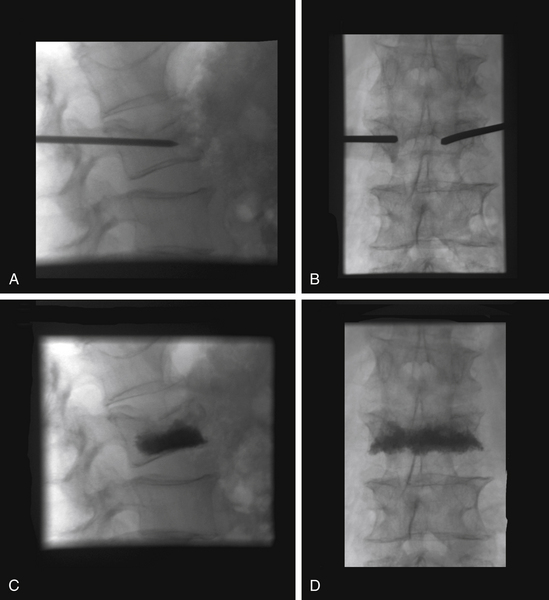
For the AP technique, the craniocaudal angulation is adjusted to bring the vertebral body end plates perpendicular to the image (Fig. 173-6). The skin entry site is placed about 1 cm superior and lateral to the center of the pedicle but must be adjusted for the thickness of the posterior paraspinal soft tissues. The needle is advanced anteriorly, medially, and caudally. By the time it reaches the bone surface, the tip should project over the upper outer cortex of the pedicle. Again, small corrections in the craniocaudal angulation can be made using a true lateral view. The needle is advanced so that its tip projects over the center of the pedicle on both AP and lateral views. The tip should project over the medial pedicle cortex as the needle traverses the posterior third of the vertebral body. The final position is again adjusted on the lateral view.
The image guidance for a parapedicular approach is quite similar. The needle is placed lateral and superior to the lateral cortex of the pedicle and enters the vertebral body at its junction with the pedicle. The position at which bone is encountered (i.e., at the junction of the pedicle and vertebral body) is more anterior on the lateral view.
The planning for the lateral position of the tip should be adjusted for the procedure to be performed and the shape of the vertebral body. Vertebroplasty for osteoporotic vertebral compression fractures was initially performed using two needles and a bipedicular approach. This technique allows reliable filling of both halves of the vertebral body, independent of the precise lateral position of the needle tip within its half of the vertebral body. However, some practitioners have adopted a unipedicular approach. This technique requires a single needle and decreases the risk and time associated with needle placement. For the unipedicular approach, a near-midline position of the needle tip provides more reliable filling of the vertebral body. In my experience, both techniques work well, and my colleagues and I base our approach on the number of levels to be treated and the configuration of the fractured vertebra. For example, in a severely collapsed vertebra, there is often substantially more marrow space at the lateral aspects of the vertebral body. In this circumstance, a bipedicular approach with lateral positioning of the needle tip provides reliable bilateral filling with little risk of symptomatic cement leakage.10 With more lateral tip positions, it is important to remember that the vertebral body is round and that the anterior cortex of the vertebra along the needle trajectory is posterior to the radiopaque line of anterior cortex on the fluoroscopic image.
Cement Placement
As the cement flows from the needle cannula, careful fluoroscopic monitoring helps ensure that the cement remains within the target zone or vertebra. While both AP and lateral views are important, the lateral is most valuable, since it allows the operator to evaluate the posterior position of the cement relative to the neural foramina and spinal canal. This view also shows venous or intradiscal leakage to good advantage. Some practitioners have advocated fluoroscopic monitoring of an injection of iodinated contrast before the cement instillation,4 but this practice is not necessary for the safe placement of cement.11
The endpoints for cement injection are (1) leakage of cement beyond the marrow space, (2) cement reaching the posterior quarter of the vertebral body, and (3) cement filling the vertical expanse of the vertebra and extending across the midline. Injection stops when any of these criteria is met (Fig. 173-7). Since the cement tends to follow any pathway of least resistance, it is rare to achieve a complete vertebral body cast. It is tempting to inject until a “pretty” fluoroscopic picture is achieved. However, filling until the practitioner has achieved a complete cast of the vertebra is not necessary to provide pain relief or stability,12,13 and when taken to extremes, this approach leads to higher rates of cement leakage and clinical complications.14 Even with these guidelines, however, there is substantial variation in philosophy and practice among practitioners regarding the optimum amount and pattern of cement deposition.15
Procedure: Kyphoplasty
Much of the kyphoplasty procedure follows steps and guidelines similar to those described for vertebroplasty. Patient preparation, sedation, positioning, and image guidance are largely the same. Kyphoplasty has traditionally been performed with general anesthesia. There is justification for this difference: The procedure time is longer, larger cannulas are used, and there is greater manipulation of osseous structures. However, many institutions have been able to overcome these obstacles for most patients, and the procedure is performed with moderate to deep sedation with success.5,16
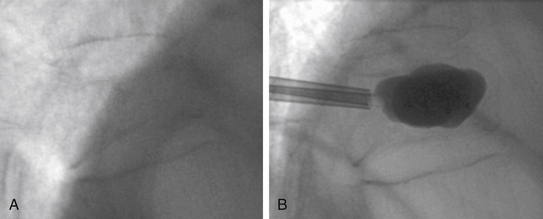
The initial needle placement is similar to that of vertebroplasty, but the cannula is only advanced to the posterior aspect of the vertebral body. The stylet or introducer is then exchanged for a hand-operated drill bit. This drill is carefully advanced to the anterior aspect of the vertebral body, 3 to 4 mm posterior to the anterior cortical margin (Fig. 173-8). In general, a near-midline position of the needle tip on the AP view is desired. The drill or introducer is removed, and the space thus created is smoothed with a blunt stylet. A deflated balloon tamp is advanced into this small cavity so that the posterior balloon marker is sufficiently anterior to the cannula tip. A second system is then placed from the other side in a similar manner. Once both balloons are in place, each balloon tamp, attached to a locking syringe with a digital manometer, is slowly inflated with iodinated contrast. The inflation is performed synchronously and is monitored with the pressure transducer and intermittent fluoroscopy. Inflation continues slowly until (1) the kyphotic deformity is corrected, (2) the balloon tamp reaches one of the cortical margins, or (3) the system reaches maximum pressure or maximum balloon volume. The balloon is then deflated. Cement is prepared and placed into tubular bone fillers. Sufficient time is allowed for the cement to reach the desired consistency, often with a greater viscosity than that many practitioners use for vertebroplasty. The loaded bone filler is placed through the cannula into the cavity, and the cement is slowly hand injected under fluoroscopic guidance. The cement fills the cavity, matching or slightly exceeding the volume of the inflated balloon tamp.
Kyphoplasty has traditionally been performed with bilateral needle and balloon placements, but unilateral balloon placement has also been used with success.5,17 Several balloon sizes and configurations improve the ability of the system to achieve vertical expansion of the vertebral body before inflation must end. An available curette allows the operator to focally disrupt the integrity of the osseous matrix before full balloon inflation, improving chances for height gain and kyphosis reduction.
Risks
Vertebroplasty and kyphoplasty are minimally invasive procedures with only small risks of morbidity and mortality. However, careful attention to technique and first-rate imaging equipment are necessary, since the practitioner is working near the spinal cord and aorta with large needles and a liquid polymer. With such care, the overwhelming majority of complications should be minor. The overall incidence of clinically evident complications for the procedures ranges from 1% to 5%.18,19
The most common complication reported for vertebroplasty and kyphoplasty is rib fracture. In the largest case series, the reported incidence is 3%.20,21 These fractures presumably result from even minor trauma to the osteoporotic skeleton during transfer of the patient or needle placement. Since such fractures can occur in these patients with even normal movement, they may be difficult to prevent entirely.
Passage of cement beyond the confines of the vertebra is a complication unique to these procedures. The cement is injected, and filling of the vertebra depends on a small pressure gradient between the needle tip and the cement’s destination. The cement flows along pathways of least resistance. These pathways include fracture clefts and venous channels. The incidence of such leakage varies substantially in reported series and is a function of the procedure chosen (vertebroplasty vs. kyphoplasty), operator experience, and approach to cement filling (see the earlier section on cement placement). In most circumstances, a small amount of extraosseous cement produces no symptoms or long-term morbidity. These leaks include those that occur along the anterior and lateral surfaces of the vertebral body and those into the intervertebral disc. However, even small amounts of cement adjacent to a nerve root can produce radicular pain. The large vertebroplasty case series published by experienced operators reported a risk of symptomatic cement leakage about the vertebral body that varies from 0% to 1% for the treatment of osteoporotic fractures11,20,21 and is up to 4% to 8% for the treatment of metastases.8,22 For kyphoplasty, the overall risk of leakage is less.18 Kyphoplasty permits greater control of cement instillation through the creation of a cavity into which a predetermined volume of cement is placed and the use of more viscous cement. The incidence of any leakage with kyphoplasty is about 14%, and symptomatic leakage is rare.18
When radiculopathy is produced by cement leakage, the pain usually can be treated with a short course of intravenous or oral steroids or nerve root block. In some cases, there is sufficient foraminal cement to cause frank root compression; in these cases, surgical decompression may be the treatment of choice.22 In rare cases, sufficient cement has been placed in the spinal canal to cause cord compression or cauda equina syndrome; surgical decompression is then warranted.23
If cement passes into perivertebral veins, it can be carried to the lungs and produce symptomatic pulmonary embolism. The incidence of small pulmonary cement emboli is probably higher than once thought, with a recent CT study uncovering the phenomenon in 23% of treatment sessions.24 However, most such emboli produce no symptoms or changes in oxygenation.24,25 Although the morbidity is usually mild,20,26 substantial cement embolization has occurred, necessitating endovascular or surgical intervention. Paradoxical embolization, including cerebral embolization and stroke, has been reported.27 Most cases of embolism have been unrecognized during cement placement; good cement opacification, high-quality equipment, vigilant fluoroscopic monitoring, and meticulous patient monitoring keep these risks to a minimum.
Other rare complications reported in the larger case series for these procedures include transient fever, transient hypotension, unexplained pain exacerbation, hematoma, pedicle fracture, noninfectious discitis, and spinal infection. Death has occurred in a few patients in the periprocedure period, generally from cardiovascular complications of uncertain etiology.28
It has been proposed that the presence of the intravertebral PMMA creates stresses that can lead to fractures in adjacent vertebrae. Additional fractures occur in 8% to 27% of patients treated with PMMA augmentation.29 Suspicion that fracture risk is increased by the procedures arises from retrospective analyses showing a substantially greater risk of fracture at levels adjacent to treated vertebrae.30,31 However, there are other explanations for this phenomenon. Regional variation in stresses and in bone integrity at baseline could explain increased fracture risk in adjacent vertebrae.29 In the one prospective, randomized trial sufficiently powered to detect differences in fracture rates, no difference was observed.32
Benefits
Pain Relief and Activity
The primary goal of both vertebroplasty and kyphoplasty is pain relief. This pain relief is often immediate (as soon as the patient has reached the recovery room) and sometimes complete. Most practitioners have had bedridden patients in severe pain leave the same day, smiling and pain free. Most patients are able to stop or reduce their use of analgesic medications and resume activities of daily living. This experience has been borne out in case series that testified to the marked pain relief and improved function in about 90% of patients.33
Until recently, data on the efficacy of these procedures chiefly consisted of large case series. For vertebroplasty, case series have reported the results in hundreds of patients with osteoporosis. Most of these studies consistent of patients treated after a 4- to 6-week trial of conservative management. These studies have uniformly shown long-standing benefits of reduced pain and improved function in patients treated.20,21,30,34,35 One small prospective, randomized trial compared vertebroplasty with medical management in patients within 8 weeks of fracture and found that patients who received vertebroplasty had substantially better pain control at 24 hours than those hospitalized for narcotic analgesia and bed rest.36 Consistent with the known natural history of patients with compression fractures (i.e., those not subjected to a trial of conservative management), follow-up at 3 months showed no significant benefit.
In 2009, the results of two double-blinded, randomized, controlled studies were reported. Each included a control group that underwent a sham procedure simulating vertebroplasty. Neither of the studies showed a major benefit for vertebroplasty. Buchbinder et al.37 randomized 78 patients and used as the primary endpoint a score for overall pain at 3 months postprocedure. The study was powered to have an 80% chance of finding a 2.5 in 10 difference in this score. Kallmes et al.,38 randomized 131 patients and used as primary endpoints the modified Roland-Morris Disability Questionnaire and an average 24-hour back pain scale at 1 month postprocedure. The study did not meet initial enrollment targets but ultimately had an estimated 80% chance of detecting a 3-point difference on the disability measure and a 1.5-point difference on the pain scale.
Kyphoplasty has shown a similar ability to reduce pain in smaller series.39–43 One larger, multicenter, prospective series of 155 patients showed a mean decrease in a visual analogue pain scale of 4.5 in 10, significant improvement in patient activity, and substantial improvements in most SF-36 physical and mental subdomains.44 Recently, the results of a multicenter, prospective, randomized trial were published for kyphoplasty. In this study, 300 patients with compression fractures were randomized to either kyphoplasty or medical management. The SF-36 physical component summary scale and other measures showed significantly greater improvement in the kyphoplasty group at 1 month.32 The positive effects persisted over 1 year, though differences between treatment and control groups slowly diminished as scores in the control group improved.
The pain resulting from neoplasm and hemangioma frequently responds to vertebroplasty or kyphoplasty. For hemangiomas, pain relief is nearly uniform and long lasting.45 For neoplasms, pain relief is achieved in many patients but results are slightly less impressive than those for patients with osteoporotic fractures.3,46 One recent prospective, uncontrolled study of kyphoplasty showed marked, immediate, and durable pain relief in such patients,47 and no clinical adverse events occurred.
Fracture Stabilization
Stabilization of the vertebral body is usually a secondary goal of vertebroplasty and kyphoplasty. Many vertebrae that have compression fractures continue to lose height over time as they undergo additional fractures. Vertebroplasty and kyphoplasty prevent this additional pain and additional deformity in almost all cases. Case series with long-term follow-up have generally not reported any recurrent fractures at treated levels.22,34 However, a small incidence of repeat fracture in treated vertebrae has been reported in the setting of osteoporosis.48 In patients with metastatic neoplasm, vertebroplasty has been performed for stabilization of pathologic but unfractured vertebrae. In this setting, no fracture has been reported in short-term follow-up.3
Height Restoration and Kyphosis Correction
Kyphoplasty has the added goal of restoring or improving vertebral body height and mechanical alignment at the fracture. The height loss and kyphosis associated with compression fractures can lead to decreased pulmonary capacity and quality of life. Furthermore, it has been proposed that the kyphotic deformity alone may predispose patients to chronic pain and the risk of additional injury. There are clearly cases in which marked height restoration and kyphosis reduction can be achieved with kyphoplasty (Fig. 173-9). There is anecdotal evidence of patients for whom kyphoplasty provides substantial relief of not only pain but also breathing difficulty and deformity. However, this feature has been de-emphasized in recent years and was not assessed in the industry-sponsored Fracture Reduction Evaluation (FREE) trial.
The restoration of vertebral body height following kyphoplasty has been quantified in several case series. Height improvement is achieved to some degree in 80% of patients,44 and complete or near-complete height restoration is achieved in 10% to 20%.40,42 Greater degrees of height restoration appear to be achieved when kyphoplasty is performed earlier.41 One study found small immediate improvement in height but observed that this diminished to baseline over 1 year.47
The restoration of alignment following kyphoplasty has been studied in only a few reports. Phillips et al.43 found 58% of fractures treated with kyphoplasty to be partially reducible; in the reducible fractures, the mean Cobb angle correction was 14 degrees. The mean for all levels was 9 degrees. Theodorou et al.16 reported substantially improved kyphosis with a mean angle correction for all fractures of about 10 degrees, representing a 62% reduction of the deformity. This improvement may also be transient.47
Vertebroplasty also appears to result in partial restoration of vertebral body height and alignment in some cases. Teng et al.9 showed small but significant improvement in vertebral height and kyphosis, with these improvements present in all but a few patients. Pitton et al.49 found durable height restoration (average 1.5 mm) and decreased wedge deformity (average 3.4 degrees) at 1 year, but these benefits were limited to patients with marked preprocedure wedge deformity. Hiwatashi et al.50 found an average 2 mm increase in vertebral body height and 3 degree decrease in wedge deformity. Furthermore, they found no significant difference for these parameters between kyphoplasty and vertebroplasty.
Future Directions
Technical Innovation
There are several PMMA formulations available, and they have different setting and mechanical properties.51 There has been considerable interest in development of higher-viscosity cements, again with the hope of providing superior vertebral filling and decreased leakage.52 One approach includes extracorporeal radiofrequency heating of the PMMA and controlled high-pressure cement injection. PMMA has been mixed with radioactive materials in a form of brachytherapy for spine metastases.53
Bioactive cement materials may one day replace PMMA. The advantage of these materials is that they more closely match the physical properties of native bone and remodel over time. Early results with these materials have been mixed. While they appear to be capable of providing similar pain relief,54,55 there have been problems with cement stability and fracture.56
Vertebroplasty and kyphoplasty are also being combined with other procedures for the treatment of neoplasm or trauma. For metastases, the procedures have been safely performed after the use of radiofrequency ablation or cyroablation.57 For burst fractures, the procedures have been combined with posterior instrumented decompression.58
Vertebroplasty versus Kyphoplasty
One of the chief controversies in the treatment of compression fractures revolves around the relative merits of vertebroplasty and kyphoplasty and their variants. Each of the procedures has some advantages. Vertebroplasty has the advantages of simplicity and lower cost. The procedure requires about half the time of kyphoplasty.5 The materials are less expensive by a factor of 5 to 10. Both procedures can be performed with moderate sedation, but the procedure time, larger cannulas, and balloon inflation of kyphoplasty make greater demands on the analgesia. Kyphoplasty has the advantage of providing better control of the infused cement, and this results in a lower incidence of extraosseous passage of PMMA and related adverse events.59
The two procedures seem to provide similar levels and duration of pain relief. Meta-analyses have shown little difference in the clinical effectiveness between the two procedures.59,60 There are two ongoing randomized, controlled trials with primary objectives of comparing the effectiveness or safety of the two procedures. The industry-sponsored Kyphoplasty and Vertebroplasty in the Augmentation and Restoration of Vertebral Body Compression Fractures trials randomized patients with osteoporotic compression fractures to one of the two procedures. Their results may be available in 2012.
The proposal that one procedure is superior to the other may be overly simplistic. These may be complementary procedures whose use can be based rationally on patient and fracture characteristics. For example, patients with recent fractures may see substantial additional benefit from kyphoplasty, whereas those with older fractures may not. One prospective study used fracture age and morphology to select the procedure performed,61 with good result.
Buchbinder R., Osborne R.H., Ebeling P.R., et al. A randomized trial of vertebroplasty for painful osteoporotic vertebral fractures. N Engl J Med. 2009;361:557-568.
Cotten A., Dewatre F., Cortet B., et al. Percutaneous vertebroplasty for osteolytic metastases and myeloma: effects of the percentage of lesion filling and the leakage of methylmethacrylate at clinical follow-up. Radiology. 1996;200:525-530.
Coumans J.V., Reinhardt M.K., Lieberman I.H. Kyphoplasty for vertebral compression fractures: 1-year clinical outcomes from a prospective study. J Neurosurg. 2003;99:44-50.
Deramond H., Depriester C., Galibert P., et al. Percutaneous vertebroplasty with polymethylmethacrylate: technique, indications, and results. Radiol Clin North Am. 1998;36:533-546.
Eck J.C., Nachtigall D., Humphreys S.C., et al. Comparison of vertebroplasty and balloon kyphoplasty for treatment of vertebral compression fractures: a meta-analysis of the literature. Spine J. 2008;8:488-497.
Evans A.J., Jensen M.E., Kip K.E., et al. Vertebral compression fractures: pain reduction and improvement in functional mobility after percutaneous polymethylmethacrylate vertebroplasty—retrospective report of 245 cases. Radiology. 2003;226:366-372.
Garfin S.R., Buckley R.A., Ledlie J. Balloon kyphoplasty for symptomatic vertebral body compression fractures results in rapid, significant, and sustained improvements in back pain, function, and quality of life for elderly patients. Spine. 2006;31:2213-2220.
Hodler J., Peck D., Gilula L.A. Midterm outcome after vertebroplasty: predictive value of technical and patient related fractures. Radiology. 2003;227:662-668.
Jensen M.E., Evans A.J., Mathis J.M., et al. Percutaneous polymethyl methacrylate vertebroplasty in the treatment of osteoporotic vertebral body compression fractures: technical aspects. AJNR Am J Neuroradiol. 1997;18:1897-1904.
Jha R.M., Yoo A.J., Hirsch A.E., et al. Predictors of successful palliation of compression fractures with vertebral augmentation: single-center experience of 525 cases. J Vasc Intervent Radiol. 2009;20:760-768.
Kallmes D.F., Comstock B.A., Heagerty P.J., et al. A randomized trial of vertebroplasty for osteoporotic spinal fractures. N Engl J Med. 2009;361:569-579.
Kim Y.J., Lee J.W., Park K.W., et al. Pulmonary cement embolism after percutaneous vertebroplasty in osteoporotic vertebral compression fractures: incidence, characteristics, and risk factors. Radiology. 2009;251:250-259.
Ledlie J.T., Renfro M. Balloon kyphoplasty: one-year outcomes in vertebral body height restoration, chronic pain, and activity levels. J Neurosurg. 2003;98:36-42.
Lee M.J., Dumonski M., Cahill P., et al. Percutaneous treatment of vertebral compression fractures: a meta-analysis of complications. Spine. 2009;34:1228-1232.
Lovi A., Teli M., Ortolina A., et al. Vertebroplasty and kyphoplasty: complementary techniques for the treatment of painful osteoporotic vertebral compression fractures. A prospective non-randomised study on 154 patients. Eur Spine J. 2009;18(Suppl 1):95-101.
Masala S., Mammucari M., Angelopoulos G., et al. Percutaneous vertebroplasty in the management of vertebral osteoporotic fractures. Short-term, mid-term and long-term follow-up of 285 patients. Skeletal Radiol. 2009;38:863-869.
McGirt M.J., Parker S.L., Wolinsky J.P., et al. Vertebroplasty and kyphoplasty for the treatment of vertebral compression fractures: an evidenced-based review of the literature. Spine J. 2009;9:501-508.
Ortiz A.O., Zoarski G.H., Beckerman M. Kyphoplasty. Tech Vasc Interv Radiol. 2002;5:239-249.
Peh W.C.G., Gilula L.A., Peck D.D. Percutaneous vertebroplasty for severe osteoporotic vertebral body compression fractures. Radiology. 2002;223:121-126.
Pflugmacher R., Taylor R., Agarwal A., et al. Balloon kyphoplasty in the treatment of metastatic disease of the spine: a 2-year prospective evaluation. Eur Spine J. 2008;17:1042-1048.
Phillips F.M., Ho E., Campbell-Hupp M., et al. Early radiographic and clinical results of balloon kyphoplasty for the treatment of osteoporotic vertebral compression fractures. Spine. 2003;28:2260-2267.
Taylor R.S., Taylor R.J., Fritzell P. Balloon kyphoplasty and vertebroplasty for vertebral compression fractures: a comparative systematic review of efficacy and safety. Spine. 2006;31:2747-2755.
Theodorou D.J., Theodorou S.J., Duncan T.D., et al. Percutaneous balloon kyphoplasty for the correction of spinal deformity in painful vertebral body compression fractures. J Clin Imaging. 2002;26:1-5.
Wardlaw D., Cummings S.R., Van Meirhaeghe J., et al. Efficacy and safety of balloon kyphoplasty compared with non-surgical care for vertebral compression fracture (FREE): a randomised controlled trial. Lancet. 2009;373:1016-1024.
Zoarski G.H., Snow P., Olan W.J., et al. Percutaneous vertebroplasty of osteoporotic compression fractures: quantitative prospective evaluation of long-term outcomes. J Vasc Interv Radiol. 2002;13:139-148.
1. Silverman S.L. The clinical consequences of vertebral compression fracture. Bone. 1992;13:S27-S31.
2. Galibert P., Deramond H., Rosat P., et al. Preliminary note on the treatment of vertebral angioma by percutaneous acrylic vertebroplasty. Neurochirurgie. 1987;33:166-168.
3. Jensen M.E., Kallmes D.E. Percutaneous vertebroplasty in the treatment of malignant spine disease. Cancer J. 2002;8:194-206.
4. Jensen M.E., Evans A.J., Mathis J.M., et al. Percutaneous polymethyl methacrylate vertebroplasty in the treatment of osteoporotic vertebral body compression fractures: technical aspects. AJNR Am J Neuroradiol. 1997;18:1897-1904.
5. Ortiz A.O., Zoarski G.H., Beckerman M. Kyphoplasty. Tech Vasc Interv Radiol. 2002;5:239-249.
6. Gaughen J.R., Jensen M.E., Schweickert P.A., et al. Lack of preoperative spinous process tenderness does not affect clinical success of percutaneous vertebroplasty. J Vasc Interv Radiol. 2002;13:1135-1138.
7. Benz B.K., Gemery J.M., McIntyre J.J., et al. Value of immediate pre-procedure MR imaging in patients scheduled to undergo vertebroplasty or Kyphoplasty. Spine. 2009;34:609-612.
8. Weill A., Chiras J., Simon J.M., et al. Spinal metastases: indications for and results of percutaneous injection of acrylic surgical cement. Radiology. 1996;199:241-247.
9. Teng M.M., Wei C.J., Wei L.C., et al. Kyphosis correction and height restoration effects of percutaneous vertebroplasty. AJNR Am J Neuroradiol. 2003;24:1893-1900.
10. Peh W.C.G., Gilula L.A., Peck D.D. Percutaneous vertebroplasty for severe osteoporotic vertebral body compression fractures. Radiology. 2002;223:121-126.
11. Vasconcelos C., Gailloud P., Beauchamp N.J., et al. Is percutaneous vertebroplasty without pretreatment venography safe? Evaluation of 205 consecutive procedures. AJNR Am J Neuroradiol. 2002;23:913-917.
12. Cotten A., Dewatre F., Cortet B., et al. Percutaneous vertebroplasty for osteolytic metastases and myeloma: effects of the percentage of lesion filling and the leakage of methylmethacrylate at clinical follow-up. Radiology. 1996;200:525-530.
13. Knavel E.M., Rad A.E., Thielen K.R., et al. Clinical outcomes with hemivertebral filling during percutaneous vertebroplasty. AJNR Am J Neuroradiol. 2009;30:496-499.
14. Ryu K.S., Park C.K., Kim M.C., et al. Dose-dependent epidural leakage of polymethylmethacrylate after percutaneous vertebroplasty in patients with osteoporotic vertebral compression fractures. J Neurosurg. 2002;96:56-61.
15. Gilula L. Is insufficient use of polymethylmethacrylate a cause for vertebroplasty failure necessitating repeat vertebroplasty? AJNR Am J Neuroradiol. 2003;24:2120-2121.
16. Theodorou D.J., Theodorou S.J., Duncan T.D., et al. Percutaneous balloon kyphoplasty for the correction of spinal deformity in painful vertebral body compression fractures. J Clin Imaging. 2002;26:1-5.
17. Lee S.B., Cho K.S., Huh P.W., et al. Clinical and radiographic results of unilateral transpedicular balloon kyphoplasty for the treatment of osteoporotic vertebral compression fractures. Acta Neurochir Suppl. 2008;101:157-160.
18. Lee M.J., Dumonski M., Cahill P., et al. Percutaneous treatment of vertebral compression fractures: a meta-analysis of complications. Spine. 2009;34:1228-1232.
19. McGirt M.J., Parker S.L., Wolinsky J.P., et al. Vertebroplasty and kyphoplasty for the treatment of vertebral compression fractures: an evidenced-based review of the literature. Spine J. 2009;9:501-508.
20. Hodler J., Peck D., Gilula L.A. Midterm outcome after vertebroplasty: predictive value of technical and patient related fractures. Radiology. 2003;227:662-668.
21. Evans A.J., Jensen M.E., Kip K.E., et al. Vertebral compression fractures: pain reduction and improvement in functional mobility after percutaneous polymethylmethacrylate vertebroplasty—retrospective report of 245 cases. Radiology. 2003;226:366-372.
22. Deramond H., Depriester C., Galibert P., et al. Percutaneous vertebroplasty with polymethylmethacrylate: technique, indications, and results. Radiol Clin North Am. 1998;36:533-546.
23. Shapiro S., Abel T., Purvines S. Surgical removal of epidural and intradural polymethylmethacrylate extravasation complicating percutaneous vertebroplasty for an osteoporotic lumbar compression fracture: Case report. J Neurosurg. 2003;98:90-92.
24. Kim Y.J., Lee J.W., Park K.W., et al. Pulmonary cement embolism after percutaneous vertebroplasty in osteoporotic vertebral compression fractures: incidence, characteristics, and risk factors. Radiology. 2009;251:250-259.
25. Venmans A., Lohle P.N., van Rooij W.J., et al. Frequency and outcome of pulmonary polymethylmethacrylate embolism during percutaneous vertebroplasty. AJNR Am J Neuroradiol. 2008;29:1983-1985.
26. Padovani B., Kasriel O., Brunner P., et al. Pulmonary embolism caused by acrylic cement: a rare complication of percutaneous vertebroplasty. AJNR Am J Neuroradiol. 1999;20:375-377.
27. Marden F.A., Putman C.M. Cement–embolic stroke associated with vertebroplasty. AJNR Am J Neuroradiol. 2008;29:1986-1988.
28. Jensen M.E., Evans A.J. Cardiovascular collapse and death during vertebroplasty. Radiology. 2003;228:902-903.
29. Hierholzer J., Fuchs H., Westphalen K., et al. Incidence of symptomatic vertebral fractures in patients after percutaneous vertebroplasty. Cardiovasc Intervent Radiol. 2008;31:1178-1183.
30. Grados F., Depriester C., Cayrolle G., et al. Long-term observations of vertebral osteoporotic fractures treated by percutaneous vertebroplasty. Rheumatology. 2000;39:1410-1414.
31. Uppin A.A., Hirsch J.A., Centenera L.V., et al. Occurrence of new vertebral body fracture after percutaneous vertebroplasty in patients with osteoporosis. Radiology. 2003;226:119-124.
32. Wardlaw D., Cummings S.R., Van Meirhaeghe J., et al. Efficacy and safety of balloon kyphoplasty compared with non-surgical care for vertebral compression fracture (FREE): a randomised controlled trial. Lancet. 2009;373:1016-1024.
33. Zoarski G.H., Snow P., Olan W.J., et al. Percutaneous vertebroplasty of osteoporotic compression fractures: Quantitative prospective evaluation of long-term outcomes. J Vasc Interv Radiol. 2002;13:139-148.
34. Perez-Higueras A., Alvarez L., Rossi R.E., et al. Percutaneous vertebroplasty: long-term clinical and radiological outcome. Neuroradiology. 2002;44:950-954.
35. Masala S., Mammucari M., Angelopoulos G., et al. Percutaneous vertebroplasty in the management of vertebral osteoporotic fractures. Short-term, mid-term and long-term follow-up of 285 patients. Skeletal Radiol. 2009;38:863-869.
36. Rousing R., Andersen M.O., Jespersen S.M., et al. Percutaneous vertebroplasty compared to conservative treatment in patients with painful acute or subacute osteoporotic vertebral fractures: three-months follow-up in a clinical randomized study. Spine. 2009;34:1349-1354.
37. Buchbinder R., Osborne R.H., Ebeling P.R., et al. A randomized trial of vertebroplasty for painful osteoporotic vertebral fractures. N Engl J Med. 2009;361:557-568.
38. Kallmes D.F., Comstock B.A., Heagerty P.J., et al. A randomized trial of vertebroplasty for osteoporotic spinal fractures. N Engl J Med. 2009;361:569-579.
39. Coumans J.V., Reinhardt M.K., Lieberman I.H. Kyphoplasty for vertebral compression fractures: 1-year clinical outcomes from a prospective study. J Neurosurg. 2003;99:44-50.
40. Dudeney S., Lieberman I.H., Reinhardt M.K., et al. Kyphoplasty in the treatment of osteolytic vertebral compression fractures as a result of multiple myeloma. J Clin Oncol. 2002;20:2382-2387.
41. Ledlie J.T., Renfro M. Balloon kyphoplasty: one-year outcomes in vertebral body height restoration, chronic pain, and activity levels. J Neurosurg. 2003;98:36-42.
42. Lieberman I.H., Dudeney S., Reinhardt M.K., et al. Initial outcome and efficacy of “kyphoplasty” in the treatment of painful osteoporotic vertebral compression fractures. Spine. 2001;26:1631-1638.
43. Phillips F.M., Ho E., Campbell-Hupp M., et al. Early radiographic and clinical results of balloon kyphoplasty for the treatment of osteoporotic vertebral compression fractures. Spine. 2003;28:2260-2267.
44. Garfin S.R., Buckley R.A., Ledlie J. Balloon kyphoplasty for symptomatic vertebral body compression fractures results in rapid, significant, and sustained improvements in back pain, function, and quality of life for elderly patients. Spine. 2006;31:2213-2220.
45. Guarnieri G., Ambrosanio G., Vassallo P., et al. Vertebroplasty as treatment of aggressive and symptomatic vertebral hemangiomas: up to 4 years of follow-up. Neuroradiology. 2009;51:471-476.
46. Jha R.M., Yoo A.J., Hirsch A.E., et al. Predictors of successful palliation of compression fractures with vertebral augmentation: single-center experience of 525 cases. J Vasc Intervent Radiol. 2009;20:760-768.
47. Pflugmacher R., Taylor R., Agarwal A., et al. Balloon kyphoplasty in the treatment of metastatic disease of the spine: a 2-year prospective evaluation. Eur Spine J. 2008;17:1042-1048.
48. Gaughen J.R.Jr., Jensen M.E., Schweickert P.A., et al. The therapeutic benefit of repeat percutaneous vertebroplasty at previously treated vertebral levels. AJNR Am J Neuroradiol. 2002;23:1657-1661.
49. Pitton M.B., Morgen N., Herber S., et al. Height gain of vertebral bodies and stabilization of vertebral geometry over one year after vertebroplasty of osteoporotic vertebral fractures. Eur Radiol. 2008;18:608-615.
50. Hiwatashi A., Westesson P.L., Yoshiura T., et al. Kyphoplasty and vertebroplasty produce the same degree of height restoration. AJNR Am J Neuroradiol. 2009;30:669-673.
51. Jasper L.E., Deramond H., Mathis J.M., et al. Material properties of various cements for use with vertebroplasty. J Mat Sci Mat Med. 2002;13:1-5.
52. Anselmetti G.C., Zoarski G., Manca A., et al. Percutaneous vertebroplasty and bone cement leakage: clinical experience with a new high-viscosity bone cement and delivery system for vertebral augmentation in benign and malignant compression fractures. Cardiovasc Intervent Radiol. 2008;31:937-947.
53. Ashamalla H., Cardoso E., Macedon M., et al. Phase I trial of vertebral intracavitary cement and samarium (VICS): novel technique for treatment of painful vertebral metastasis. Int J Radiat Oncol Biol Phys. 2009;75:836-842.
54. Nakano M., Hirano N., Matsuura K., et al. Percutaneous transpedicular vertebroplasty with calcium phosphate cement in the treatment of osteoporotic vertebral compression and burst fractures. J Neurosurg Spine. 2002;97:287-293.
55. Grafe I.A., Baier M., Noldge G., et al. Calcium-phosphate and polymethylmethacrylate cement in long-term outcome after kyphoplasty of painful osteoporotic vertebral fractures. Spine. 2008;33:1284-1290.
56. Blattert T.R., Jestaedt L., Weckbach A. Suitability of a calcium phosphate cement in osteoporotic vertebral body fracture augmentation: a controlled, randomized, clinical trial of balloon kyphoplasty comparing calcium phosphate versus polymethylmethacrylate. Spine. 2009;34:108-114.
57. Munk P.L., Rashid F., Heran M.K., et al. Combined cementoplasty and radiofrequency ablation in the treatment of painful neoplastic lesions of bone. J Vasc Intervent Radiol. 2009;209:903-911.
58. Pflugmacher R., Agarwal A., Kandziora F., et al. Balloon kyphoplasty combined with posterior instrumentation for the treatment of burst fractures of the spine—1-year results. J Orthop Trauma. 2009;23:126-131.
59. Taylor R.S., Taylor R.J., Fritzell P. Balloon kyphoplasty and vertebroplasty for vertebral compression fractures: a comparative systematic review of efficacy and safety. Spine. 2006;31:2747-2755.
60. Eck J.C., Nachtigall D., Humphreys S.C., et al. Comparison of vertebroplasty and balloon kyphoplasty for treatment of vertebral compression fractures: a meta-analysis of the literature. Spine J. 2008;8:488-497.
61. Lovi A., Teli M., Ortolina A., et al. Vertebroplasty and kyphoplasty: complementary techniques for the treatment of painful osteoporotic vertebral compression fractures. A prospective non-randomised study on 154 patients. Eur Spine J. 2009;18(Suppl 1):95-101.






