[level-membership-for-surgery-category]
CHAPTER 5 Ventral Herniorrhaphy
BACKGROUND
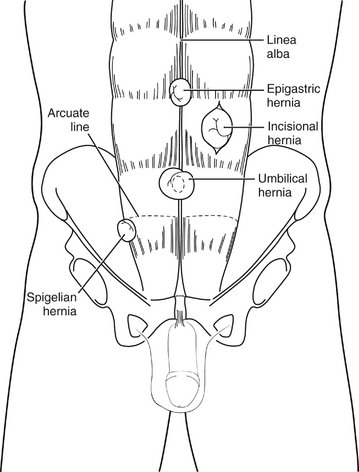
A variety of abdominal wall hernias (ventral hernias) are commonly treated by the general surgeon (Fig. 5-1). Umbilical hernias are common in young children; most close by 2 years of age, and repair is rarely considered before 5 years of age. Umbilical hernias in adults are most commonly acquired and typically develop in patients with elevated intra-abdominal pressure (e.g., from obesity, pregnancy, or ascites). Epigastric hernias are found in the midline, superior to the umbilicus, and are often small and multiple. Pain may result from incarceration of properitoneal fat. Spigelian hernias result from herniation at the lateral border of the rectus sheath (linea semilunaris). A bulge is rarely apparent because these hernias usually dissect behind the external oblique aponeurosis. Incisional hernias are a common complication of abdominal surgery, occurring after up to 10% of abdominal wall closures. Technical error (e.g., excessive tension on the abdominal closure and inadequate approximation of the fascial edges) is the major etiology. Factors that result in increased intra-abdominal pressure (e.g., obesity, pregnancy, and ascites) and compromise wound healing (e.g., malnutrition and immunosuppression) may be contributory.
INDICATIONS FOR VENTRAL HERNIA REPAIR
PREOPERATIVE EVALUATION
COMPONENTS OF THE PROCEDURE AND APPLIED ANATOMY
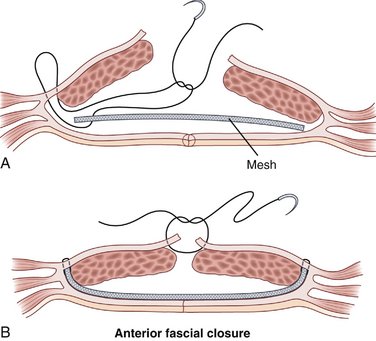
Ventral hernias may be repaired using a variety of approaches. Factors that influence the choice of approach include the size of the defect, the integrity of the abdominal wall fascia surrounding the hernia, and surgeon preference (Fig. 5-2).

Preoperative Considerations
Operative Repair
COMPLICATIONS
Berry MF, Paisley S, Low DW, Rosato EF. Repair of large complex recurrent incisional hernias with retromuscular mesh and panniculectomy. Am J Surg. 2007;194:199-204.
Malangoni MA, Gagliardi RJ. Hernias. In: Townsend CM, Beauchamp RD, Evers BM, Mattox KL, editors. Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice. 17th ed. Philadelphia: Saunders; 2004:1199-1218.
[/level-membership-for-surgery-category][not-level-membership-for-surgery-category]
CHAPTER 5 Ventral Herniorrhaphy
BACKGROUND
A variety of abdominal wall hernias (ventral hernias) are commonly treated by the general surgeon (Fig. 5-1). Umbilical hernias are common in young children; most close by 2 years of age, and repair is rarely considered before 5 years of age. Umbilical hernias in adults are most commonly acquired and typically develop in patients with elevated intra-abdominal pressure (e.g., from obesity, pregnancy, or ascites). Epigastric hernias are found in the midline, superior to the umbilicus, and are often small and multiple. Pain may result from incarceration of properitoneal fat. Spigelian hernias result from herniation at the lateral border of the rectus sheath (linea semilunaris). A bulge is rarely apparent because these hernias usually dissect behind the external oblique aponeurosis. Incisional hernias are a common complication of abdominal surgery, occurring after up to 10% of abdominal wall closures. Technical error (e.g., excessive tension on the abdominal closure and inadequate approximation of the fascial edges) is the major etiology. Factors that result in increased intra-abdominal pressure (e.g., obesity, pregnancy, and ascites) and compromise wound healing (e.g., malnutrition and immunosuppression) may be contributory.
INDICATIONS FOR VENTRAL HERNIA REPAIR
PREOPERATIVE EVALUATION
COMPONENTS OF THE PROCEDURE AND APPLIED ANATOMY
Ventral hernias may be repaired using a variety of approaches. Factors that influence the choice of approach include the size of the defect, the integrity of the abdominal wall fascia surrounding the hernia, and surgeon preference (Fig. 5-2).
