17
Urinary incontinence
Introduction
Urinary incontinence is defined as the condition in which there is involuntary loss of urine, which can be objectively demonstrated and which is a social or hygienic problem. It should be noted that the volume of urine lost is not a feature of the definition, but the ability of an independent person to confirm that there is urine loss is essential.
Urinary incontinence is an important condition because it causes significant distress. It is generally accepted that around 15% of the adult female population have a significant problem with urinary incontinence, for which they are getting treatment or would like treatment if it is available. Urinary incontinence is a major quality-of-life (QOL) issue. Patients can become reclusive, unwilling to go out and feel a burden to their loved ones. Incontinence increases in age with the incidence of an overactive bladder as high as 50% or more in institutionalized elderly females.
Types of urinary incontinence
The commonest types of urinary incontinence in women are:
 stress urinary incontinence (SUI)
stress urinary incontinence (SUI)
 overactive bladder (OAB)
overactive bladder (OAB)
 mixed incontinence (SUI and OAB)
mixed incontinence (SUI and OAB)
 retention with overflow
retention with overflow
 fistula.
fistula.
Stress urinary incontinence (SUI) is the commonest cause of urinary incontinence in adult women, accounting for 40% of cases. SUI is a sign or a symptom, but if this is proven at urodynamic testing, then it is called ‘urodynamic stress incontinence’ (USI). This has replaced the old term ‘genuine stress incontinence’. SUI is leakage that occurs when there is a rise in intra-abdominal pressure without a detrusor contraction; women therefore notice leakage on coughing, laughing, sneezing, etc. and, in severe cases, even on walking or on rising from a sitting position.
An overactive bladder (OAB; previously called detrusor instability, detrusor overactivity or detrusor hyperreflexia), occurs when a woman is incontinent in response to an involuntary detrusor contraction. This accounts for about 25% of cases of incontinence in adult women as a sole diagnosis. The woman will experience urgency, and if she cannot reach the toilet and the bladder contraction persists, she will be incontinent. As the problem tends to happen both day and night, she will usually also complain of urinary frequency and nocturia, and, in severe cases, enuresis (bed wetting).
Increasingly, women have a pattern of mixed incontinence (having both SUI and OAB) and this now accounts for around 30% of cases.
Retention with overflow is only common in elderly female patients or in those with a neurological problem. The denervated bladder continues to fill until it simply spills over, resulting in leakage.
A fistula is an abnormal communication between two epithelial surfaces and, in the UK, usually results as a complication of surgery. In less affluent countries, obstructed labour is a common cause. Any communication between the lower urinary tract (ureter, bladder or urethra) and the genital tract (uterus and vagina) will result in continuous dribbling incontinence. Fistulae account for only 1 in 1000 cases of incontinence in women in the UK.
It is important to be aware that any incontinent woman may have more than one type of coexisting incontinence. As stated, SUI and OAB commonly coexist, and voiding difficulty or retention can accompany either or both of these.
The mechanism of continence
The mechanism of continence must be understood if the pathophysiology of incontinence is to be understood. In the normal woman, continence is maintained at the level of the bladder neck. If, for instance, a radio-opaque medium was to be placed in the bladder of a normal, continent woman and that woman was asked to stand, an X-ray would demonstrate that urine does not flow into the urethra. The concept therefore arose of a so-called proximal urethral sphincter, a mechanism present in the region of the bladder neck and proximal urethra, which maintains continence. It was originally considered that this was an arrangement of smooth muscle in the proximal urethra. However, no such sphincter mechanism based upon muscle, exists. There is smooth muscle in the proximal urethra but it generally runs in a longitudinal rather than a circular direction and as such, could not maintain continence.
It is now considered that the so-called proximal urethral sphincter mechanism is a water-tight seal, which maintains the pressure in the urethra greater than the pressure in the bladder. The anatomical basis of that seal is considered to be a series of arteriovenous anastomoses within the wall of the proximal urethra. These can be demonstrated on histological examination. They allow some degree of turgor pressure to be exerted circumferentially around the urethra, which results in the formation of a hermetic seal by keeping the urethra occluded. The effect of any pressure exerted around the periphery of a hollow tube is to occlude that tube. If the pressure is exerted in numerous places around the circumference of the tube, then the tube will simply close. Such is the proximal urethral sphincter.
The situation becomes more complex, in that if a pressure study is performed to compare the pressure in the urethra with the pressure within the bladder, then while the pressure in the proximal urethra exceeds that in the bladder, the greatest pressure difference exists at the mid-urethra. This is the so-called distal urethral sphincter mechanism. This does have an anatomical basis in muscle in that striated muscle, innervated by spinal roots S2–4, is found within the wall of the mid-urethra.
There are further features which aid the maintenance of continence, particularly the supporting tissues around the urethra, which maintain the proximal urethra in an intra-abdominal position. The importance of this position is that if the proximal urethra is intra-abdominal, then any pressure rise within the abdomen will be transmitted equally to the bladder and the proximal urethra; the pressure difference will not change and continence will therefore be maintained. Weakness or damage to the supporting tissues may predispose to SUI. The supporting tissues are characterized anatomically as the pubourethral ligaments, derived from the fascia of the pelvic floor, and, to a lesser degree, the pelvic floor musculature, namely levator ani. It has been demonstrated that vaginal delivery may denervate both the pubourethral ligaments and levator ani, the nerve damage being manifest within the pudendal nerve. Thus, vaginal delivery may predispose towards SUI.
There is also the concept of bladder stability. The bladder muscle, the detrusor, should only contract during micturition, whereas it should relax during bladder filling. Such a situation is described as a ‘stable’ bladder. In women who have an overactive bladder, the detrusor initially relaxes during filling but then contracts involuntarily. Such a situation is termed an overactive bladder (OAB). If the contraction is modest, then the woman will appreciate the contraction as urinary urgency, but if the contraction is strong enough to elevate the pressure in the bladder above that in the urethra, then there will be the symptom of urge incontinence.
Aetiology
Stress urinary incontinence
SUI clearly requires some degree of weakness of both the proximal and distal urethral sphincter mechanisms. While no single aetiological factor exists in all women with SUI, there are a series of predisposing factors which often explain the condition. These include:
 pregnancy
pregnancy
 prolapse
prolapse
 menopause
menopause
 collagen disorder
collagen disorder
 obesity.
obesity.
Pregnancy
Vaginal delivery may cause denervation of the pudendal nerve and hence damage to the supporting tissues of the urethra. Moreover, the pudendal nerve in part supplies innervation to the distal urethral sphincter. The first vaginal delivery is more likely than a subsequent vaginal delivery to cause SUI, and this incontinence may be preventable by elective caesarean section. There is also a transient form of SUI, which occurs during pregnancy but is not present outside of pregnancy. The mechanism of this incontinence is a combination of the raised intra-abdominal pressure related to uterine contents together with the smooth-muscle-relaxant effect of progesterone. Thus, some women will describe SUI during pregnancy but not at other times.
Prolapse
Prolapse and SUI coexist in over 50% of cases. Only if the bladder neck/continence mechanism is prolapsing is the prolapse per se, the cause of this. The relationship otherwise relates to poor pelvic floor function secondary to pudendal nerve damage, which is the main aetiology of both conditions.
Menopause
Many women date the onset of their symptoms from the menopause. There is evidence that the withdrawal of oestrogen reduces the so-called maximal urethral closure pressure; hence the pressure in the urethra is not as great as it used to be. The effect of this pressure reduction is that a smaller rise in intra-abdominal pressure will result in SUI.
Collagen disorder
Collagen is a major component of the pubourethral ligaments. There are several different types of collagen within the body and there is evidence that there are different types of collagen in varying proportions in the pubourethral ligaments of women who become incontinent compared with the pubourethral ligaments of those who do not.
Overactive bladder
In the majority of women, the aetiology of an overactive bladder is unknown. Neurological conditions, typically multiple sclerosis, stroke or cervical spine lesions, are known to be a cause of overactivity but it is very uncommon for such patients to present de novo at a urogynaecology clinic. There is also a link between psychological upset and OAB, with such patients having a higher than background incidence of anxiety and neuroses.
Voiding difficulty
The aetiology of voiding difficulty in the female is the opposite of that in the male. In women, it is due to an underactive detrusor (hypotonia) in 90% of cases, and in only 10% of cases does it reflect anatomical obstruction. The aetiology of the detrusor hypotonia is usually simply ageing, with the natural reduction in muscle fibres and muscle strength being enough to bring about a clinical problem. There is some evidence that young women who put off voiding during their adult life (‘infrequent voiders’) are more prone to this problem. Women with neurological disease can have voiding difficulty due to either detrusor hypotonia or obstruction, in the latter case secondary to inappropriate contraction of the urethral sphincter.
Clinical presentation
Stand-alone symptoms are uncommon and so urinary incontinence usually presents as part of a symptom complex comprising stress incontinence, frequency, urgency and nocturia. Urge incontinence will usually be present if the patient is suffering from an overactive bladder. One must also enquire about voiding problems, and the symptoms in women are the same as in men with prostatic enlargement: hesitancy, poor stream, intermittent stream, straining to void, feeling of incomplete emptying and post-micturition dribbling. Symptoms of haematuria or recurrent urinary tract infections are of concern and merit urological assessment of both upper and lower urinary tracts.
Prolapse will coexist with stress incontinence in over 50% of cases, and an enquiry about symptoms is essential. Similarly, although the symptoms are often unvoiced, anal incontinence is often present in association with urinary incontinence and must be sought. A full medical history and drug history will allow assessment of whether these problems are contributory to the patient’s incontinence.
As mentioned in the introduction, urinary incontinence is a major quality-of-life issue and it is essential to assess to what degree the woman’s symptoms are impacting on her lifestyle. Incontinence can prevent a woman from socializing and following her pastimes and in severe cases, have a significant detrimental effect on personality. It is not unheard of for incontinence to render someone incapable of leaving the house. It can also have a significant negative impact upon a woman’s sex life, and incontinence during intercourse is a common but usually unvoiced problem. Nocturia is a significant problem, leaving the sufferer lacking sleep and often having difficulty with concentration and even working. Nocturia in the elderly also carries the risk of falls, with fractured neck of femur the common outcome. The various effects upon QOL that have been identified are given in Table 17.1. It should be noted that in the elderly, urinary incontinence is the second commonest reason for a patient being unable to return to independent living.
Table 17.1
Effect of urinary incontinence upon quality-of-life
| Emotions | Feelings of stigma and humiliation. Social and recreational withdrawal. Fear and anxiety related to being incontinent in public |
| Relationships | Reduced intimacy, affection and physical proximity. Marriage breakdown and subsequent divorce |
| Employment | Absence from work. Loss of concentration. Interruption of work for toilet breaks |
| Sleep | Nocturia is common and quality and amount of sleep is affected. Tiredness the next day. Risk of falls especially in the elderly |
| Exercise and sport | A barrier to exercise |
| Travel and holidays | Reluctance to visit new places. Need to pack protective materials |
Diagnostic evaluation
Clinical examination
All women should undergo an abdominal and pelvic examination. This should be done after she has emptied her bladder. Abdominal examination may reveal a palpable bladder suggesting urinary retention, and infrequently an otherwise unsuspected pelvic mass may be palpable. Pelvic examination may reveal pelvic organ prolapse or vaginal atrophy. Coexisting symptomatic prolapse will suggest a surgical solution for the incontinence, while atrophic changes require treatment with vaginal oestrogens. Stress urinary incontinence may be demonstrable; the woman should be asked to give a single sharp cough. A brief neurological assessment of the S2,3,4 dermatomes should be performed and, if symptoms of anal incontinence are present, the anal sphincter tone should be determined by digital examination.
Further assessment
Urinalysis
Every woman presenting with lower urinary tract symptoms should have a urinalysis performed. The presence of leucocytes and nitrites suggests a urinary tract infection and this may be causing or worsening the patient’s symptoms. Treatment with a broad-spectrum antibiotic should be started and a mid-stream specimen of urine sent if there is no response. The presence of haematuria should prompt cystoscopy, and ultrasound of the upper renal tracts. The presence of glycosuria may suggest diabetes, which can predispose to recurrent urinary tract infections and urinary frequency.
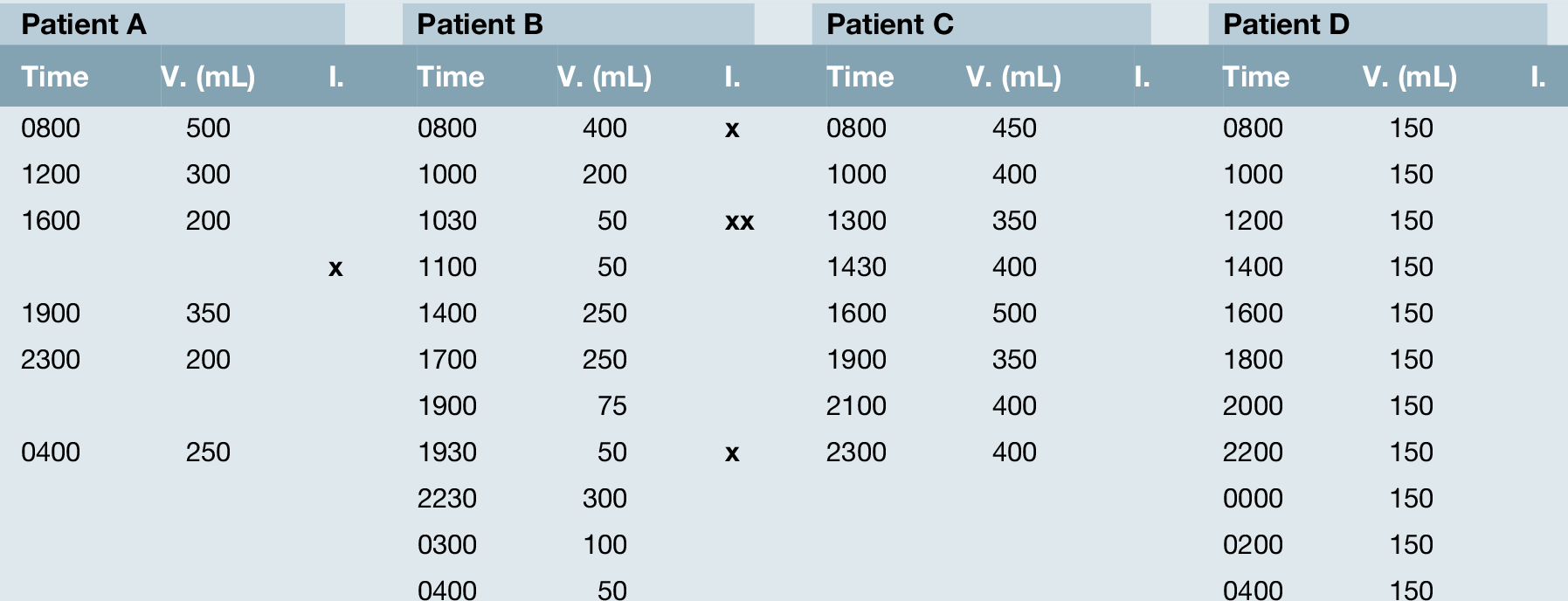
Frequency-volume chart
This simple non-invasive assessment (sometimes also called a bladder chart or bladder diary) can be extremely useful in determining the cause of a woman’s symptoms; she keeps a note of how often she voids (‘V’) and how much she passes each time. In addition, she can mark down if she is incontinent (‘I’ on the chart). Preferably 2–3 days should be monitored. Table 17.2 shows an example from four patients. Patient A has normal frequency but is incontinent when not needing the toilet. This is likely to represent SUI. Patient B has a normal bladder capacity (400 ml) but is emptying her bladder with as little as 50 ml in it, and this is typical of an overactive bladder. In addition, she is wet when going to the toilet; further evidence of OAB. Patient C is over-drinking and this is giving her urinary frequency and high urinary output. Patient D has a pathologically small bladder – probably inflammatory in nature. As the woman responds to treatment, her frequency volume chart will improve, acting as a simple form of biofeedback.
Cystoscopy
Cystoscopy is required only for the assessment of haematuria or recurrent urinary tract infections. It is not required for those suffering purely from an overactive bladder.
Ultrasound measurement of post-void residual
This is a simple non-invasive test that should be performed in the presence of symptoms of voiding difficulty or in an elderly patient with incontinence.
Quality-of-life questionnaires
Much more emphasis is being placed upon QOL and a woman’s subjective assessment of her problem and response to treatment than has previously been the case. With this in mind, several QOL questionnaires have been developed and validated for women suffering from lower urinary tract symptoms. This should be a part of the assessment of every woman both before and after treatment, along with an impression of what she expects from treatment; shared goals will improve patient satisfaction.
Urodynamic studies
These tests are a dynamic assessment of the lower urinary tract and offer objective information about bladder and urethral function. They are, however, invasive, embarrassing, expensive and time-consuming. Furthermore, they are not foolproof in providing a diagnosis. All of these facts have led to a trend in putting less emphasis on the result of urodynamic studies and more on the patient’s perspective of her symptoms. The aim of urodynamics is to achieve a diagnosis, and differentiating between SUI and OAB in a woman with a mixture of symptoms, is arguably the most useful information these tests provide. They can also predict the success of surgery and the complications of surgery. The indications for urodynamic studies are listed in Box 17.1.
Box 17.1
Indications for urodynamic studies
 In patients with symptoms of voiding difficulty
In patients with symptoms of voiding difficulty
 In patients with neurological disease
In patients with neurological disease
 When conservative treatment has been tried and failed
When conservative treatment has been tried and failed
 Prior to surgery
Prior to surgery
 When surgery has failed
When surgery has failed
Treatment
Treatment options for urinary incontinence comprise:
 conservative treatment (lifestyle interventions and bladder retraining)
conservative treatment (lifestyle interventions and bladder retraining)
 physiotherapy
physiotherapy
 drug therapy
drug therapy
 surgery.
surgery.
Treatment should start with conservative treatment and this usually includes two distinct approaches: lifestyle interventions and bladder retraining. The GP or practice nurse can provide these; however, in reality, the time and experience these require mean it is probably better to involve a trained continence advisor or clinical nurse specialist.
Lifestyle interventions
Appropriate lifestyle changes are shown in Box 17.2. These changes are often difficult to achieve, but that is no reason for not educating the patient about what she can do to improve things herself. Indeed, it is imperative that we do, as often more invasive therapies are not without significant potential side-effects.
Box 17.2
 Normalize fluid intake. Many women drink too much, worsening frequency and incontinence, though many people with OAB over-restrict the amount of fluid they drink, increasing the risk of bladder irritation; 1.5 litres per day is the aim
Normalize fluid intake. Many women drink too much, worsening frequency and incontinence, though many people with OAB over-restrict the amount of fluid they drink, increasing the risk of bladder irritation; 1.5 litres per day is the aim
 Cut down alcohol and restrict caffeine. These drinks should constitute no more than a third of the total daily fluid intake
Cut down alcohol and restrict caffeine. These drinks should constitute no more than a third of the total daily fluid intake
 Lose weight if BMI > 30
Lose weight if BMI > 30
 Stop smoking
Stop smoking
 Avoid carbonated drinks
Avoid carbonated drinks
 Treat chronic constipation and chronic cough
Treat chronic constipation and chronic cough
Bladder retraining
This physical therapy is another common non-pharmacological intervention, the objective of which is to re-establish cortical control over voiding. The patient emptying her bladder to a strict time schedule, usually hourly to begin with, achieves this. The time interval between voids is then increased to achieve a normal micturition pattern. The best results are achieved when done under the supervision of a continence nurse or specialist physiotherapist. To aid bladder retraining the following techniques are usually taught:
 distraction techniques, or doing something that requires concentration
distraction techniques, or doing something that requires concentration
 sitting on a hard seat or across a tightly rolled towel
sitting on a hard seat or across a tightly rolled towel
 pelvic floor squeezes.
pelvic floor squeezes.
Physiotherapy
Physiotherapy is the first-line treatment for incontinence caused by pelvic floor dysfunction, but is also of some benefit to those with OAB. Treatment involves muscle training using pelvic floor exercises, which are regular voluntary contractions and relaxations of the pelvic floor muscles. It aims to both improve urethral resistance and pelvic visceral support by increasing the strength of the voluntary pelvic floor muscle contraction, and teach voluntary contraction of the muscles before increases in abdominal pressure. It may take 6 months to train muscles effectively, and women should be advised of this.
Biofeedback can be used as an adjunct to physiotherapy. It allows the patient to recognize the strength of an appropriate pelvic floor muscle contraction by verbal feedback during digital palpation, or electromyogenic feedback using vaginal electrodes.
Cones can be inserted vaginally for short periods to produce contractions in an attempt to retain them. Patients exercise daily with increasing weights, retaining the cone for 10–20 min each time. Cure or improvement rates after physiotherapy as high as 60% have been noted. Programmes cannot be successful in women who cannot locate and properly contract their pelvic floor muscles. An instructor followed-up training programme is more effective than home exercise. It appears that the most benefit occurs in women with mild or moderate incontinence, although improvement can still be seen in those with severe symptoms.
Drug therapy
Conservative measures and physiotherapy can help up to three out of four women and are the only available interventions with no side-effects. If these fail, medical therapy should be prescribed. The mainstay of medical treatment for the overactive bladder over the last 30 years has been the antimuscarinics with all of the following agents currently licensed for treatment of OAB in the UK:
 solifenacin (Vesicare)
solifenacin (Vesicare)
 fesoterodine (Toviaz)
fesoterodine (Toviaz)
 oxybutynin (Lyrinel XL, Ditropan, Kentera)
oxybutynin (Lyrinel XL, Ditropan, Kentera)
 darifenacin (Emselex)
darifenacin (Emselex)
 tolterodine (Detrusitol and Detrusitol XL)
tolterodine (Detrusitol and Detrusitol XL)
 trospium (Regurin XL)
trospium (Regurin XL)
 propiverine (Detrunorm XL).
propiverine (Detrunorm XL).
The best estimate of the effectiveness of antimuscarinics is that on average about 50% of women will have up to 50% improvement. Side-effects – including dry mouth, dizziness, nausea and constipation – remain problematic; however, given that if drug therapy fails, further treatments for OAB are either very serious or unlikely to be effective, one must ensure that several if not all of the above drugs have been tried before abandoning medical treatment.
In 2013, a new class of drug Mirabegron was launched for the treatment of OAB. Mirabegron is a Beta3 adrenoreceptor agonist, so acts in an entirely different way from the antimuscarinics. While clinical trials have shown promising results in terms of efficacy and tolerability, at the time of writing, it is too early to say what impact it will have in clinical practice.
Medical therapy for SUI comprises oestrogens or Duloxetine. Vaginal oestrogens should be prescribed to all women with urinary incontinence who are postmenopausal and who are not taking a systemic HRT preparation. Duloxetine is a combined serotonin and noradrenaline reuptake inhibitor licensed for use in moderate to severe SUI. Blockade of serotonin and noradrenaline reuptake in the spinal cord stimulates pudendal motor neurons, increasing stimulation of urethral striated muscles in the sphincter, and enhancing contraction. Duloxetine improves SUI by increasing urethral closure pressure and electrical activity of the sphincter. Adverse effects are related to increases in noradrenaline and serotonin, and include gastrointestinal disturbances, dry mouth, headache and, rarely, suicidal ideology.
Surgery
Surgical treatment of SUI and OAB are entirely different, with the former condition usually responding to minimally invasive procedures. OAB, however, requires major surgery with significant complications, and here, surgery is very much a last resort.
Surgery for SUI
The first-line surgical treatment of SUI is to insert a suburethral tape, of which there are several types. The tapes currently in use are made of polypropylene and are macroporous (Fig. 17.1). The principle of all tapes is the same; the tape is left under the mid-urethra without tension, being anchored by its serrated polypropylene edges into one or other part of the patient’s connective tissue, the site of attachment being different with each procedure. The urethra is compressed against the tape at times of increased intra-abdominal pressure, thus preventing leakage. Although the tape is effective from day 1, it takes several months before the tape is invaded by fibroblasts and connective tissue is laid down in and around the tape making it permanently fixated into the tissues. For this reason, it is essential that the patient avoids any straining, heavy lifting or any other causes of increased intra-abdominal pressure for up to 3 months. Any of the tapes may be combined with a prolapse repair.

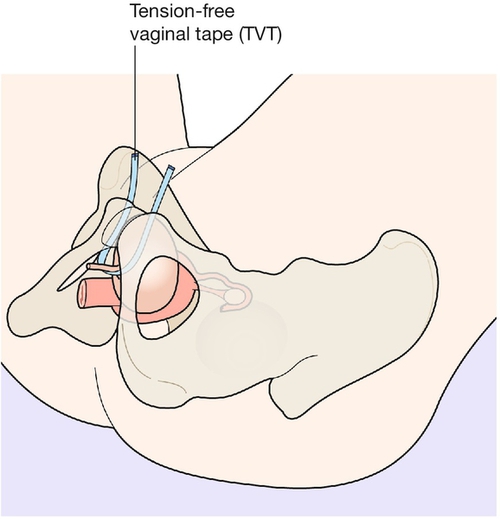
Tension-free vaginal tape (transvaginal tape, TVT)
This was the first tape to be developed and used clinically. It was introduced to UK practice in 1998. The tape is inserted vaginally on two trocars, bypasses the bladder neck and bladder and exits suprapubically (Fig. 17.2).
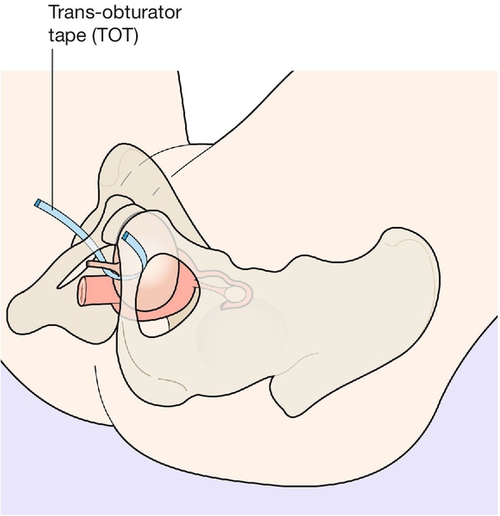
Trans-obturator tape (TVT-O, TVT Abbrevo)
This procedure was first described in 2002. Here, after the same insertion point in the vagina, the tape is channelled through the obturator membrane on either side and out towards the adipose tissue of the thigh (Fig. 17.3). Trans-obturator tape has the advantage over TVT of avoiding blind entry into the retropubic space, therefore reducing the risk of damage to the internal organs. The TVT-O procedure was complicated by unacceptably high rates of thigh pain, which has been corrected by the introduction of the TVT Abbrevo. The insertion is exactly the same but in the latter procedure, the outer third of the tape on each side is replaced by nylon threads, which are removed at the end of the insertion leaving only the central 8 cm or so of tape anchored between the obturator membranes on either side.
Single incision tapes, ‘minitapes’ (TVT Secur, Mini tape, Mini Arc, Ajust)
The first ‘mini tape’ was introduced in 2006 as a modification of the tapes described above. The tapes were inserted again through a similar vaginal incision but then anchored into the patients tissues without exiting through the skin, hence the name ‘single incision slings’. The proposed benefit of these was that as there was much less passage through the tissues the likelihood of damage to vessels, nerve and pelvic organs was less. Protagonists hold that it is only the small portion of tape under the urethra that contributes to continence therefore the efficacy should be the same.
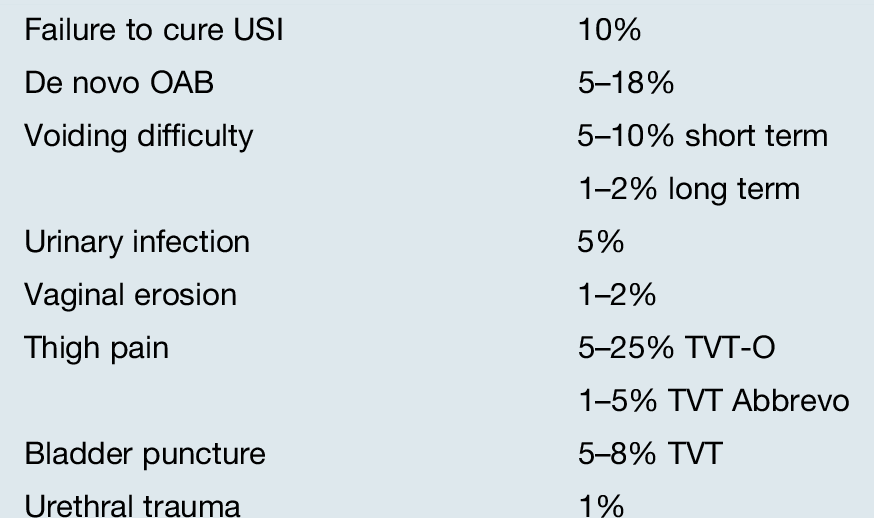
Cure rates for USI of around 90% are reported from the TVT, TVT-O and the best studies of the single incision tapes. Several studies of the minitapes have shown significantly poorer success rates however and some of the tapes are no longer being used. Complications of all of the tapes are similar and are shown in Table 17.3. Each surgeon has his or her preference for which tape they use and there is currently no, one clear favourite, among surgeons in the UK. It needs to be remembered that although the cure rate for USI is 90% that does not mean that 9 out of 10 patients are delighted with the final results of surgery. That is because either they may have one of the complications listed, or that they had a mixed pattern of both SUI and OAB prior to their tape procedure and the OAB symptoms remain. It is not wrong to put in a tape for a patient who has mixed SUI and OAB as long as: (a) stress incontinence is her biggest problem; (b) she understands that the tape will not cure her OAB symptoms and (c) she says her quality-of-life will be significantly improved if her stress incontinence is cured but her OAB symptoms remain.
More than 150 operations have been described for the treatment of SUI and, while most have been consigned to the annals of history, the following two operations are sometimes still performed as a secondary procedure when a tape procedure has failed.
Open (Burch) colposuspension
This is an abdominal operation where the bladder neck and base are elevated by suturing the upper lateral vaginal walls to the iliopectineal ligaments. This procedure is highly effective and appears to remain so with time. Throughout the 1970s and 1980s, this was the surgery of choice, with a success rate of 85% after 5 years. Complications following surgery are a high rate of voiding disorder, detrusor overactivity and genitourinary prolapse. A randomized control trial in 2004 showed the TVT to be as successful as a colposuspension in curing SUI, with a lower rate of the major complications.
Conventional sling surgery
Sling procedures using autologous or synthetic material have high efficacy rates that are sustained with time. When using autologous material, strips of rectus fascia are placed in a sling under the bladder neck and cause urethral closure when the sling is stretched.
Surgery for OAB
If medical treatment fails, then all of the following treatments have a place. All are specialized procedures and are typically the domain of the urologist or specialist urogynaecologist:
 sacral nerve root stimulation (neuro-modulation)
sacral nerve root stimulation (neuro-modulation)
 botulinum toxin A injections
botulinum toxin A injections
 detrusor myectomy
detrusor myectomy
 augmentation cystoplasty.
augmentation cystoplasty.
Treatment of voiding disorders
The treatment of voiding difficulty is first and foremost clean intermittent self-catheterization (CISC). This puts the woman in control of her voiding function and carries less risk of infection than does an indwelling catheter. If she does not have the mental agility or physical ability to perform CISC, an indwelling catheter (urethral or suprapubic) may be required.
Treatment of genitourinary fistulae
If a period of indwelling catheterization fails to close the fistula, surgical correction will be required.



