The big picture165
12.2 Upper thorax, brachial plexus, pectoral girdle, scapula166
12.3 Shoulder region171
12.4 Axilla175
12.5 Arm, elbow, cubital fossa, supination, pronation176
12.6 Flexor compartment of the forearm, carpus, carpal tunnel180
12.7 Hand185
12.8 Innervation, nerve testing, surface anatomy190
Beware!
‘Arm’ means upper limb from shoulder to elbow, not the entire upper limb. ‘Forearm’ means upper limb from elbow to wrist.
Radial, ulnar, lateral, medial
Particularly in the forearm and hand, the terms radial and ulnar are used in preference to lateral and medial (respectively). This avoids confusion which may arise depending upon the position of the hand. The thumb is always on the radial side, and the little finger always on the ulnar side.
12.1. The big picture
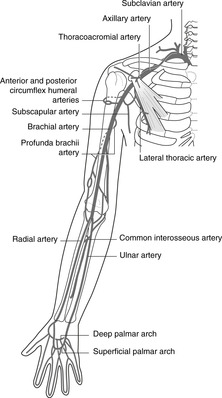
Arteries (see Fig. 7.1, p. 44; Fig. 12.1)
Arterial blood to the upper limb comes from the subclavian and axillary arteries.
• Subclavian: extends from its origin to the lateral border of the first rib.
• Axillary: extends from the lateral border of the first rib to the lateral border of teres major muscle.
• Brachial: extends from the lateral border of teres major to the cubital fossa, where it bifurcates to give:
• Radial (lateral) and ulnar (medial) arteries. These pass down the respective sides of the forearm to the hand where they form two anastomoses in the palm:
• Superficial and deep palmar arterial arches.
 |
| Fig. 12.1 |
Veins (see Fig. 7.2, p. 45)
Venous blood drains to the subclavian veins, thence to the brachiocephalic veins and the superior vena cava.
Superficial veins are immediately subcutaneous, superficial to the deep fascia which surrounds the muscles, bones and other deeper structures like a sleeve. These veins are visible or palpable (unless the patient is very fat) and are easily accessible for venepuncture. The pattern of superficial veins is very variable: you need only bother with:
• the dorsal venous arch on the back of the hand, very variable pattern, from which arise:
– the cephalic vein: lateral side of the upper limb to the deltopectoral groove between the deltoid and pectoralis major muscles
– the basilic vein: medial side of the upper limb, piercing the deep fascia as it approaches the axilla and contributing to the formation of the axillary vein
– veins in front of the elbow (often injection sites): these are very variable, but there is usually a median cubital vein (see Fig. 12.20 and look at your own).
 |
| Fig. 12.20 |
• Deep veins, within the fascial sleeve, accompany the arteries and are thus named venae comitantes (Latin: accompanying veins). They receive connections from the superficial veins and in the axillary region unite to form the axillary vein, which then becomes the subclavian.
The subclavian vein crosses the superior surface of the first rib, anterior to the attachment of scalenus anterior (the artery is posterior to it). This joins the internal jugular vein behind the sternoclavicular joint) to form the brachiocephalic vein.
Lymph
All lymph drains to axillary nodes.
• From the radial side of the upper limb, lymph drains alongside the cephalic vein to the deltopectoral (infraclavicular) nodes, outposts of the axillary nodes to which they drain. The deltopectoral nodes are the only lymph nodes on this pathway and are the first nodes to be involved in, for example, an infection of the thumb.
• From the ulnar side of the upper limb, lymph drains alongside the basilic vein to the epitrochlear nodes, just above the elbow, thence to the axillary nodes.
Nerves
All nerves come from the ventral rami of C5, 6, 7, 8 and T1, which form the brachial plexus.
Dermatomes and myotomes. In the body wall, the muscles and skin supplied by one segmental nerve are roughly coexistent. This is not so in the limbs. The dermatomes (sensory) are shown in Figure 6.6 (p. 36), but the muscles supplied by the same spinal segments are often far distant. For example, T1 dermatome is in the axilla, but muscles supplied by T1 are in the hand. An embryology book will explain why, but the ‘big picture’ is that dermatomes are arranged roughly from cephalic (above) to caudal (below) if you hold out your arm horizontally with the palms facing forwards, and the myotomes are arranged from proximal (C5 for shoulder movements) to distal (T1 for small muscles of the hand). See Chapter 6, p. 31.
12.2. Upper thorax, brachial plexus, pectoral girdle, scapula
The subclavian, axillary and branchial arteries, together with their branches, supply the upper limb. Easily palpable pulses are the brachial, radial and ulnar. Upper limb nerves come from the brachial plexus formed by ventral rami of spinal nerves C5, 6, 7, 8 and T1. Extensor muscles and skin over the posterior aspect of the upper limb are supplied by the radial and axillary nerves and their branches. The principal nerves supplying flexor muscles and anterior skin are the median, ulnar and musculocutaneous. The clavicle and scapula articulate with the thorax at the sternoclavicular joint, and with each other at the acromioclavicular joint, diseases of both joints hindering upper limb movements.
You should:
• describe the main arterial tree of the upper limb, and the position of the brachial, radial and ulnar pulses
• explain the principles of venous and lymph drainage of the upper limb
• describe the formation, position and main branches of the brachial plexus
• describe the principal features of the clavicle and scapula, and understand the manner in which they move on the thorax.
Vessels (Fig. 12.1)
Subclavian artery
Subclavian pulse. The subclavian pulse is palpable above and behind the middle of the clavicle. The artery is deep to the vein here.
Axillary artery
This is divided into three parts by pectoralis minor muscle.
• Branches of first part (medial to pectoralis minor):
– supreme or highest thoracic (unimportant).
• Branches of second part (behind pectoralis minor):
– thoracoacromial: to upper chest and acromial region, breast
– lateral thoracic: to breast and chest.
• Branches of third part (between pectoralis minor and lateral border of teres major):
– subscapular: to scapular muscles, scapular anastomosis
– anterior circumflex humeral
– posterior circumflex humeral.
These last two may arise by a common trunk. They form an arterial circle round the surgical neck of the humerus (see Fig. 12.9) and supply the neighbouring bone, muscles and shoulder joint.
Scapular anastomosis
The arterial anastomosis around the shoulder joint receives blood from branches of the subclavian and axillary arteries, and has connections with the intercostals. It may be involved in bypassing a blocked distal subclavian or proximal axillary artery, blood flowing retrogradely up the subscapular to reach the distal axillary; and in bypassing an aortic coarctation (see Fig. 10.25, p. 88).
Veins
All veins from the upper limb, pectoral and scapular regions, together with the external jugular veins from the neck, drain into the subclavian vein. The only details worth committing to memory are:
• The cephalic vein penetrates the clavipectoral fascia (a fascial sheet between the clavicle and pectoralis minor muscle, occupying the deltopectoral triangle) to become deep before it joins the axillary vein. This is one place where central lines (catheters inserted into the heart) may be inserted.
• The subclavian vein is accessible for catheters, etc. just behind the middle of the clavicle. Aim the catheter downwards and medially: the vein is superficial here.
• The subclavian vein joins the internal jugular to form the brachiocephalic behind the sternoclavicular joint.
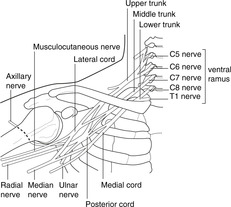
Brachial plexus and main branches (Fig. 12.2)
Roots and trunks
Roots of the plexus: ventral rami of C5–T1.
• The ventral rami of C5 and 6 join to form the upper trunk.
• The ventral rami of C8 and T1 join to form the lower trunk.
 |
| Fig. 12.2 |
Branches of roots and trunks, in order of importance
• Long thoracic (supplies serratus anterior), from C5, 6, 7 roots.
• Suprascapular (supplies infra- and supraspinatus), upper trunk C5, 6.
• Dorsal scapular (supplies rhomboids), C5 root; nerve to subclavius, C5, 6 roots (don’t bother with either the nerve or the muscle).
Divisions, cords
Each trunk divides into an anterior and a posterior division, the divisions uniting to form cords as described. The cords are named by the position in respect to the axillary artery: posterior, lateral, medial.
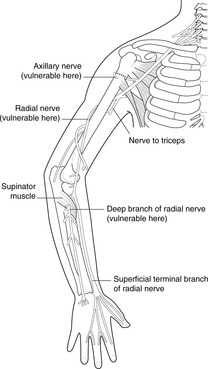
Posterior cord and branches (Fig. 12.3)
Posterior divisions all unite to form the posterior cord, branches of which supply the posterior skin of the upper limb and all the extensor muscles. Its branches are:
• axillary, C5, 6: to deltoid muscle (shoulder abduction), skin over deltoid muscle
• radial, C5–T1: to all extensor muscles, posterior skin of entire upper limb
• other branches: subscapular nerves, thoracodorsal nerves: to posterior scapular muscles and latissimus dorsi.
 |
| Fig. 12.3 |
Lateral cord and branches (Fig. 12.4)
The anterior divisions of the upper and middle trunks unite to form the lateral cord. Its branches are:
• musculocutaneous nerve, C5, 6, 7: to elbow flexors and lateral skin of the forearm
• contribution to the median nerve (see below)
• lateral pectoral: to pectoral muscles (not important).
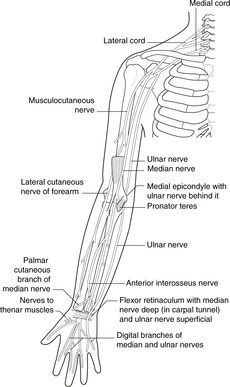
Medial cord and branches (Fig. 12.4)
Median nerve, plexus position and variations
• The median nerve is formed from all roots, C5–T1. The contributions from the lateral and medial cords may unite within a short distance, or they may remain separate until well down the arm. It supplies most forearm flexors, the thenar muscles of the hand, and skin of the radial side of the palm of the hand.
• The brachial plexus is found at the top of the rib cage. It is behind and beneath the clavicle and first rib, and trauma or disease in the posterior triangle of the neck may damage the upper trunk.
• The plexus may arise from C4–8 (prefixed), or C5–T2 (postfixed).
Bones of the pectoral girdle (Fig. 4.1, p. 20; Figs 12.5, 12.6)
Clavicle
The only feature of note is the tuberosity near the lateral end, for the attachment of the coracoclavicular ligaments. The clavicle tends to fracture immediately medial to this ligamentous attachment (see later).
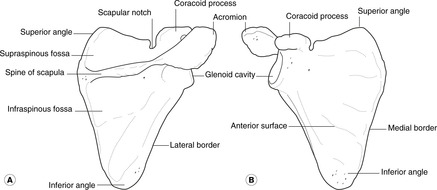
Scapula
• The anterior or costal surface is plain and is the subscapular fossa (sub- because it is ‘underneath’ in the quadruped).
• The posterior or dorsal surface is divided by the spine into the supraspinous and infraspinous fossas.
• The spine is prolonged laterally to form the acromion, which articulates with the clavicle.
• The glenoid fossa is the articular surface for the head of the humerus.
Movements and muscles of the pectoral girdle
Every time you move your upper limb, you move the clavicle and scapula. The joints that link them to the trunk are therefore important and disease of them will limit upper limb movement.
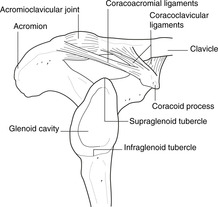
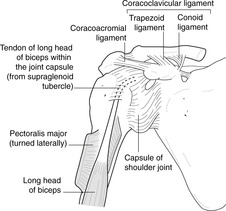
Joints and ligaments (Fig. 12.6)
Sternum–clavicle–scapula
• Sternoclavicular joint: synovial. Important relation: immediately posterior is the formation of the brachiocephalic vein from the subclavian and internal jugular veins. This joint sometimes disarticulates, the medial end of the clavicle appearing as a lump. It may or may not be painful, and often happens for no very obvious reason.
• Acromioclavicular joint: synovial.
• Coracoacromial ‘articulation’. A strong ligament.
• Coracoclavicular ‘articulation’. Strong ligaments, conoid and trapezoid, form an axis around which some rotation of the scapula on the clavicle (or vice versa) takes place, and the union is sufficiently strong for force transmitted up the arm from, say, a fall on the outstretched hand to fracture the clavicle medial to the attachment of the coracoclavicular ligament. The lateral portion of the fractured clavicle is displaced downwards by the weight of the upper limb.
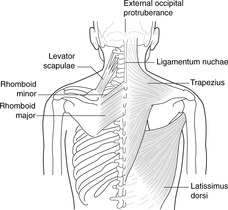
Muscles (Figs 12.7, 12.8)
Trapezius. Attachments: external occipital protuberance, spines of cervical (through ligamentum nuchae) and thoracic vertebrae–clavicle, acromion and lateral part of spine of scapula. Upper fibres pass to the clavicle, acromion and lateral end of the spine; lower fibres pass to the medial end of the spine.
 |
| Fig. 12.7 |
 |
| Fig. 12.8 |
Nerve supply to muscles
Accessory (eleventh cranial) nerve. (See Neck, page 256.)
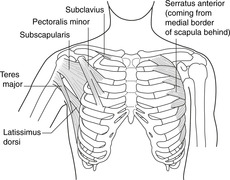
Serratus anterior. Attachments: medial border of scapula – upper eight ribs. This runs laterally and anteriorly from the medial border of the scapula, between the scapula and the rib cage. It is important in a quadruped since it is one of the muscles that suspends the trunk from the limbs. Because of the separate digitations to the eight ribs, the anterior border appears serrated, hence the name serratus. (Serratus posterior muscle: don’t even think about it.)
Long thoracic nerve (of Bell)
This nerve runs on the medial wall of the axilla, or, if you prefer, on the lateral surface of the rib cage, and may be damaged in axillary surgery, or by trauma to the chest wall. Paralysis or weakness would result in winging of the scapula in which the medial border of the scapula was no longer closely apposed to the back of the rib cage. Shoulder protraction and abduction would be impaired.
Levator scapulae. Attachments: C1–4 vertebrae – upper medial border of scapula.
Branches from C3, 4, 5 ventral rami. Unimportant
Rhomboids. Attachments: medial border of scapula – spines of thoracic vertebrae T2–5.
Dorsal scapular nerve
Pectoralis minor. Attachments: coracoid process–anterior aspect of ribs 3–5.
Pectoral nerves (details not necessary)
Latissimus dorsi. Attachments: thoracolumbar vertebrae and lumbar fascia–humerus. It is considered later, but a small portion of it attaches to the inferior angle of the scapula, and so it may be involved in scapular rotation.
Thoracodorsal nerve from posterior cord
Movements of the scapula
The scapula moves over the chest wall, but there are no distinct anatomical joints. Instead, muscles pull the scapula forward and backwards (protraction and retraction), and they rotate it so that the inferior angle moves laterally and up, and the superomedial angle medially and down.
• Protraction: serratus anterior, pectoralis minor.
• Retraction: trapezius (lower fibres), rhomboids (latissimus dorsi possibly).
• Rotation: trapezius (upper fibres), serratus anterior. Upper fibres of trapezius pull the acromioclavicular region superomedially, and the lower fibres of serratus anterior pull the inferior angle laterally and forwards. This means that the glenoid cavity faces upwards, and this movement is a necessary accompaniment of shoulder abduction (see later).
12.3. Shoulder region
The glenohumeral joint, an articulation between scapula and humerus, sacrifices stability for mobility. Movements in all planes are possible, ligaments and the rotator cuff muscles providing stability lacking in the bony conformation. These may be damaged giving rise to limitation of movement. Dislocations of the humeral head, or fractures of the surgical neck of the humerus, may damage the axillary nerve which supplies the principal shoulder abductor, deltoid.
You should:
• describe the surface anatomy of the shoulder region
• describe the principal features of the upper humerus and scapula
• list the main muscle groups producing shoulder movements, and their innervation
• describe how stability is provided at the joint, and the medical conditions that can arise.
Bones and ligaments
Scapula
Glenoid fossa. This relatively shallow articular surface is made deeper by a circumferential lip of cartilage, the glenoid labrum. Above and below the fossa are two areas, the supra- and infraglenoid tubercles, to which the long heads of, respectively, biceps and triceps are attached.
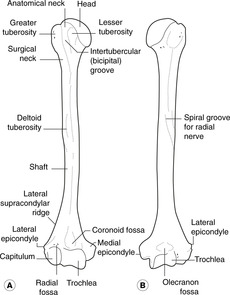
Upper humerus (Figs 12.9, 12.10)
• Head. This articulates with the glenoid fossa of the scapula.
• Greater (lateral) and lesser (anteromedial) tuberosities provide attachments for muscles and are separated by the intertubercular sulcus or groove which, because it transmits the tendon of the long head of biceps is also known as the bicipital groove (the name used in this text).
• Surgical neck. This is important since it is a site of fracture and is related to the axillary nerve that passes from medial to lateral behind the surgical neck. It may be damaged in surgical neck fractures or by shoulder dislocations. The circumflex humeral arteries are also related to it.
• Deltoid tuberosity. This is a roughness just above midway down the lateral aspect of the humerus. Deltoid muscle is attached here.
• Spiral groove. You will see a ‘spiral’ impression running from the upper medial aspect of the bone, behind the shaft and appearing on the lower lateral aspect. This is formed by the attachments of triceps muscle, but its importance lies in the fact that the radial nerve is close to the bone throughout the length of the groove. Mid-shaft fractures of the humerus may damage the radial nerve leading to paralysis or weakness of all extensor muscles distal to the injury. See later: wrist drop (section 12.8, p. 190).
 |
| Fig. 12.10 |
Muscles of the shoulder region
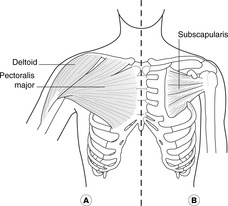
• Pectoralis major (Fig. 12.11). Attachments: medial half of clavicle (the clavicular head) and sternum, ribs and external oblique aponeurosis (the sternocostal head)–lateral lip of the bicipital groove of the humerus. The two heads can work separately. To demonstrate this, put your hand in front of your chest underneath a desk surface and pull up, feeling the muscle. Now put your hand on top of the desk and push down. Despite its size, we could live well enough without it. It flexes the shoulder (bringing the humerus in front of the chest) and adducts it (although gravity more often than not does this). It is large in creatures that swing from tree to tree and some athletes.
– Nerve supply: medial and lateral pectoral nerves.
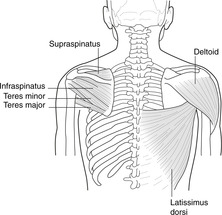
• Latissimus dorsi and teres major (Fig. 12.12). Latissimus dorsi attachments: lumbosacral fascia, spines of vertebrae L5 up to T7–floor of the bicipital groove of the humerus. It has an extensive trunk attachment but a small humeral attachment. It is the posterior counterpart of pectoralis major, and extends and adducts the shoulder. As it sweeps past the inferior angle of the scapula it is joined by some fibres attached to that bone. It is very closely associated with teres major muscle.
Teres major attachments: lower lateral part of the scapula–medial edge of the bicipital groove of the humerus.
– Nerve supply of both muscles: branches of the posterior cord of the brachial plexus (as befits extensors), the nerve to latissimus dorsi being the thoracodorsal nerve.
• Deltoid (Figs 12.11, 12.12). Attachments: lateral end of spine of the scapula, acromion, acromioclavicular joint, lateral clavicle–deltoid tuberosity of the humerus.
– Nerve supply; axillary nerve C5, 6. This muscle is often the site of intramuscular injections. If you insert the needle within 4 cm of the acromion you are unlikely to damage the axillary nerve as it enters the muscle from behind the surgical neck of the humerus. If you go lower than this, you deserve to be prosecuted for incompetence.
• Rotator cuff muscles (Figs 12.12, 12.13). The four muscles of the rotator cuff form a protective sheath for the shoulder joint behind, on top and in front. They are, from back to front:
– Teres minor: lateral aspect of scapula (above teres major)–posterior surface of greater tuberosity of humerus. It is really a slightly detached part of the infraspinatus. Nerve supply: axillary nerve (C5, 6).
– Infraspinatus: infraspinous fossa of the scapula–greater tuberosity of humerus. Nerve supply: suprascapular nerve (C5, 6).
– Supraspinatus: supraspinous fossa of the scapula–upper part of greater tuberosity of humerus. Nerve supply: suprascapular nerve (C5, 6).
– Subscapularis: anterior (costal) surface of scapula (subscapular fossa)–lesser tuberosity of humerus. Nerve supply: subscapular nerves from posterior cord of brachial plexus.
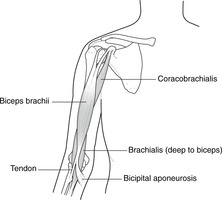
• Biceps and coracobrachialis (Fig. 12.14). Biceps has two heads: the long head is attached to the supraglenoid tubercle of the scapula; the short head is attached to the coracoid process. The tendon of the long head originates within the shoulder joint capsule and passes between the capsule and the synovium to emerge at the bicipital groove of the humerus through which it runs. The two bellies of biceps unite inferiorly to attach to the radius and to the fascia over forearm flexor muscles. Biceps crosses two joints, shoulder and elbow, flexing them both. It is also considered in relation to the elbow joint (see section 12.5, p. 176).
 |
| Fig. 12.14 |
• Coracobrachialis (unimportant): coracoid process of the scapula–upper humerus.
Both muscles contribute to shoulder flexion.
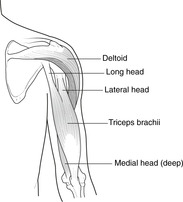
• Triceps (Fig. 12.15). Attachments: scapula and humerus–ulna. Triceps has three heads:
– long, from the infraglenoid tubercle of the scapula
– lateral, from the back of the humerus, above and lateral to the radial groove (more superficial than lateral)
– medial, from the back of the humerus, below and medial to the radial groove (more deep than medial).
 |
| Fig. 12.15 |
The radial nerve runs through the muscle in the spiral groove of the humerus between the lateral and medial heads.
– Nerve supply: radial nerve (C7, 8).
Movements and stability of the shoulder
The articular surfaces of the shoulder are not a good fit. This means that although the range of movement is very extensive, the joint is unstable and liable to disarticulation with the head of the humerus dislocating, usually anteroinferiorly. Compensating to some extent for the lack of bony stability are the rotator cuff muscles and the glenohumeral ligaments.
Abduction
Deltoid is the main abductor. Supraspinatus is said to initiate the movement by holding the head of the humerus on the scapula so that the deltoid can get some purchase on the movement, but electromyography studies show that both muscles act throughout. When the arm is abducted to about 90°, the greater tuberosity of the humerus comes in contact with the acromion and there is some lateral rotation of the humerus so that more movement is possible.
The accepted wisdom handed down from text to text is that after 90° of abduction the scapula rotates as a result of the action of serratus anterior and trapezius (see above), which allows the arm to be abducted much further. This is wrong, as you will see if you use your eyes: the scapula begins to rotate well before even 45° abduction is reached. Inability to abduct beyond 90°, such as might result from weakness of trapezius and serratus anterior is a nuisance: it would mean that you could not groom your hair, scratch your head, reach for high shelves, and so on.
Nerve supply of abduction
• deltoid and supraspinatus: axillary, suprascapular nerves (both C5, 6)
• scapular rotation: long thoracic nerve (C5, 6, 7); accessory (eleventh cranial) nerve.
Flexion, extension
See above – pectoralis major, biceps, coracobrachialis, latissimus dorsi.
Rotation
• Lateral rotation: mainly by infraspinatus, teres minor and posterior fibres of deltoid.
• Medial rotation: mainly by pectoralis major, subscapularis and teres major.
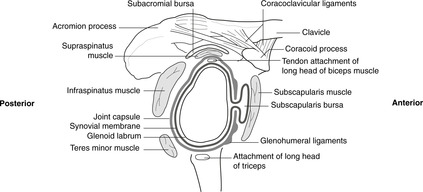
Shoulder joint capsule, glenohumeral ligaments, dislocations (Fig. 12.13)
The joint capsule is reinforced by the tendons of the rotator cuff muscles and anteriorly also by three thickenings, the glenohumeral ligaments (Fig. 12.13). With the rotator cuff muscles, these help to compensate for the poor fit of the articular surfaces. Inferior to the joint there is neither rotator cuff muscle nor capsular reinforcement – a potential weakness taken advantage of by shoulder dislocations. Sports players (particularly of racquet sports) and others who habitually hyperextend their shoulder joints may stretch the anterior wall of the capsule and subscapularis tendon so that joint dislocation becomes more common. This can be managed surgically by tightening the glenohumeral ligaments and/or the subscapularis tendon.
Blood supply of the shoulder joint
The blood supply of any joint is profuse. It is necessary to know only that branches of the anterior and posterior circumflex humerals, axillary and brachial arteries supply the shoulder.
Nerve supply of the shoulder joint
As usual (Hilton’s law), sensory fibres from the joint are carried in nerves which supply muscles acting on the joint, particularly the axillary nerve C5, 6.
Synovial cavity and bursas (Fig. 12.13)
The synovial cavity extends inferiorly for some distance, presumably to allow for hyperabduction.
• Subacromial or subdeltoid bursa. This lies between supraspinatus tendon (below) and the acromioclavicular articulation and the attachment of deltoid (above). It has two names because in adduction the bursa is more lateral (subdeltoid), but in abduction it is more medial (subacromial). It is separate from the joint cavity unless supraspinatus tendon is torn.
• Other bursas. There is usually a bursa, an extension of the joint space, deep to subscapularis muscle. Other bursas may also be found.
Nerve injuries
• Axillary nerve: this may be damaged by fractures of the surgical neck of the humerus, or by shoulder dislocations.
• Radial nerve: this may be damaged in the spiral groove by midshaft humeral fractures.
Other conditions
Inflammation of the attachment of supraspinatus to the greater tuberosity is one cause of ‘frozen shoulder’, rotator cuff syndromes, or impingement syndromes (all meaning much the same). It can be very painful and disabling, substantially limiting movement.
Surface anatomy
Normally the most lateral bony point of the skeleton is the greater tuberosity of the humerus. In shoulder dislocations, the head of the humerus is displaced down and medially, and the most lateral point is then the acromion process.
12.4. Axilla
The axilla is bounded by the anterior and posterior axillary folds, the humerus and the rib cage. It contains axillary vessels, components of the brachial plexus, and lymph nodes so often involved in breast disease.
Spatial considerations (Fig. 12.16)
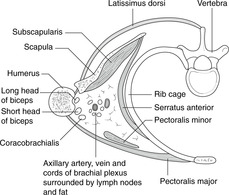
The axilla is like a distorted four-sided pyramid:
• base: skin of the armpit
• anterior wall: anterior axillary fold made up of pectoralis major muscle
• medial wall: chest wall with the long thoracic nerve (to serratus anterior) and the lateral thoracic artery passing down
• posterior wall: posterior axillary fold made up of latissimus dorsi and teres major muscles
• lateral ‘wall’: the anterior and posterior walls converge on the bicipital groove of the humerus that contains the tendon of the long head of biceps.
 |
| Fig. 12.16 |
Contents
• Vessels: axillary artery and vein with branches and tributaries (see section 12.2, p. 167).
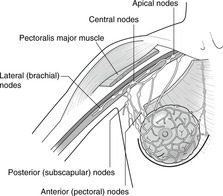
• Lymph nodes (Fig. 12.17):
– anterior or pectoral group: lymph from most of the breast
– posterior or subscapular group: lymph from the upper trunk and axillary tail of the breast
– lateral group: lymph from the ulnar side of the upper limb
– central group: lymph from all the above groups
– apical group: lymph from the central group (i.e. all the above) and the deltopectoral (infraclavicular) nodes (lymph from radial side of upper limb, alongside the cephalic vein).
 |
| Fig. 12.17 |
From the apical group, which gathers all together, lymph passes to the origin of the brachiocephalic veins where it enters the venous system.
• Fascia. The clavipectoral fascia extends from the clavicle down in the floor of the deltopectoral groove (triangle) and splits to enclose pectoralis minor muscle. Below this, it continues as the suspensory ligament of the axilla that attaches to the axillary skin. None of these details is important.
Long thoracic nerve (of Bell)
It is important in axillary surgery (e.g. for breast cancer) not to damage the long thoracic nerve. This would result in winging of the scapula, impaired shoulder abduction and loss of function. The nerve may also be damaged in those poor unfortunates who fall asleep, for whatever reason, with their arms over the back of a chair.
Lymph from the upper limb
Breast surgery in which the lymphatic channels from the upper limb are occluded will result in lymphoedema (lymphatic engorgement) of the upper limb. This is fortunately less common now with improved pharmacological treatments available.
12.5. Arm, elbow, cubital fossa, supination, pronation
At the elbow, the radiohumeral articulation permits flexion and extension, and the superior radioulnar joint permits pronation and supination. The cubital fossa anterior to the elbow contains the termination of the brachial artery and the median nerve, and is covered by the bicipital aponeurosis. The ulnar nerve passes posterior to the medial epicondyle. Elbow flexion is supplied by C5, 6; extension by C7, 8; pronation and supination by C5, 6.
Bones, joints and ligaments
Mid- and lower humerus (Fig. 12.9)
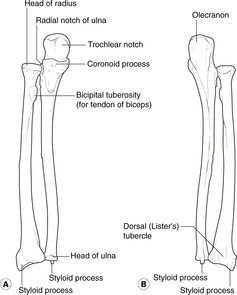
Proximal ulna (Fig. 12.18)
• Olecranon process: triceps attachment.
• Coronoid process: brachialis is attached to its anterior aspect.
• Between the olecranon and coronoid processes is the articular surface for the humerus at which flexion and extension take place.
• Articular surface for radius.
• Interosseous border.
Ulna or ulnar?
Ulna is the name of the bone; ulnar is an adjective that describes other things, as in the ulnar side of the hand.
Proximal radius (Fig. 12.18)
• Head. This articulates with:
– the capitulum of the humerus, as part of the elbow flexion-extension mechanism; and
– the ulna, as part of the pronation-supination mechanism (see below).
• Neck: immediately distal to the head; the deep branch of the radial nerve (posterior interosseous nerve) is vulnerable here. Damage to it (e.g. radial neck fractures, radial head dislocations) would impair function of the wrist and digital extension.
• Bicipital tuberosity. The tendon of biceps attaches here.
Annular ligament: pronation and supination (Fig. 12.19)
The head of the radius is held against the ulna by the annular ligament attached to the upper and lower margins of the ulnar facet for the superior radioulnar joint. During pronation and supination the head of the radius rotates within this (see below).
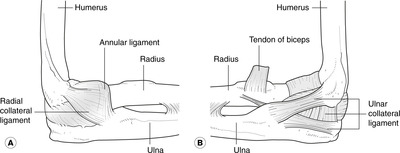
Elbow joint (Fig. 12.19)
Functionally, there are two joints although only one synovial cavity:
• Humerus–ulna: synovial hinge joint for flexion and extension.
• Superior (proximal) radioulnar joint: for pronation and supination. See above.
Injuries
• The ulna can be dislocated posteriorly.
• The head of the radius may be pulled distally, with or without damaging the annular ligament. This is more common in children since the head of the radius is still cartilaginous and the annular ligament is not such a tight fit as in the adult. The deep branch of the radial nerve may be damaged.
Surface anatomy of the elbow region
• The olecranon and the medial and lateral epicondyles are all palpable. Viewed from behind, these should form an almost isosceles triangle with the olecranon at the apex. This arrangement is disrupted in elbow dislocations.
• The head of the radius is also palpable about 2 cm distal to the lateral epicondyle. You can confirm that it is the head of the radius by feeling it rotate during pronation and supination.
Brachial artery (Fig. 12.20)
• The brachial artery is a continuation of the axillary at the lower border of teres major. It descends in the flexor compartment of the arm. Soon after its origin it gives off:
• The profunda brachii artery, or deep branch (it usually retains its Latin title), which passes laterally with the radial nerve into the spiral groove.
Brachial pulse
The brachial pulse is palpable by pressing the artery from the medial aspect against the humerus. The artery passes anterior to the elbow joint, and bifurcates in the cubital fossa into the radial and ulnar arteries. Occasionally this bifurcation may occur much higher, in the arm itself.
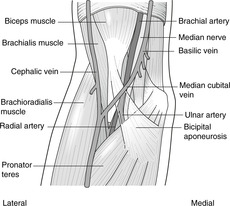
Cubital fossa (Fig. 12.20)
The triangular area in front of and slightly distal to the elbow is the cubital, or antecubital, fossa. Cubit means variously ulna, elbow or pertaining to the forearm (the Biblical unit of measurement, the cubit, was the length of the forearm). The fossa is bounded proximally by an imaginary line joining the two humeral epicondyles, and distally by the pronator teres muscle on the ulnar side and the brachioradialis on the radial side.
The cubital fossa is often the site of injections into superficial veins. Its major contents are:
• the biceps tendon (easily palpable), medial (ulnar) to which is
• the brachial artery and its bifurcation, medial (ulnar) to which is
• the median nerve.
Fortunately, from the point of view of inserting needles into superficial veins, these important structures are covered by a sheet of tough fascia extending from the biceps muscle and tendon medially to the deep fascia over the forearm flexor muscles: this is the bicipital aponeurosis and is part of the distal attachment of biceps (see later).
The floor of the fossa is formed by brachialis muscle (lower anterior humerus – coronoid process of ulna) which is an elbow flexor.
Nerves of the elbow region
• Radial nerve. From the spiral groove, the nerve emerges laterally deep between brachialis and brachioradialis. At the elbow it divides into:
– the superficial branch, usually known simply as the radial nerve, which runs down the radial side of the forearm and supplies overlying skin and that of the back of the hand; and
– the deep branch (posterior interosseous nerve), which passes through supinator muscle, winds round the neck of the radius and enters the posterior compartment of the forearm to supply extensor muscles.
• Ulnar nerve. From its origin from the medial cord of the brachial plexus, the nerve passes down the medial side of the arm, behind the medial epicondyle of the humerus (where it is vulnerable), through the forearm where it supplies flexor muscles and anterior skin, to the hand (see section 12.7, p. 185).
• Median nerve. From its origin from the lateral and medial cords of the brachial plexus, the nerve passes down the arm on brachialis to the cubital fossa where it is medial to the brachial artery. In the forearm it penetrates pronator teres muscle and continues deep to flexor digitorum superficialis into the forearm and hand flexor muscles and anterior skin.
• Other nerves:
– Lateral cutaneous nerve of the forearm, the nerve known at its origin as the musculocutaneous, supplying elbow flexors. Its new name indicates its distal function. It is otherwise unimportant.
– Medial cutaneous nerve of the forearm. Unimportant.
Muscles and movements of the elbow
Flexion (Figs 12.14, 12.19)
Flexion of the elbow is performed by: brachialis, biceps – musculocutaneous nerve, C5, 6, and brachioradialis – radial nerve, C5, 6.
• Brachialis. Attachments: anterior lower humerus–coronoid process of ulna.
• Biceps. Attachments: scapula–radius. Biceps was considered as a flexor of the shoulder (see section 12.3, p. 171). It also flexes the elbow and supinates the forearm. The proximal attachment is to the scapula (long and short heads – see section 12.3). The distal attachment has two components:
– the tendon of biceps, which attaches to the bicipital tuberosity of the radius
– the bicipital aponeurosis, which passes medially from the lower part of the muscle belly and neighbouring tendon, protecting the contents of the cubital fossa, and blending with the fascia over the forearm flexor muscles.
There are two bellies that unite inferiorly to attach to the ulna and to the fascia over forearm flexor muscles (see later). The biceps tendon jerk (C5, 6), elicited by tapping the biceps tendon in the cubital fossa, is a commonly used neurological test (see section 12.8, p. 190).
• Brachioradialis. Attachments: humerus–radius. embryologically this is an extensor muscle (thus radial nerve) that has strayed from the straight and narrow path. It forms the radial (lateral) edge of the forearm, and the radial border of the cubital fossa. When you are lifting a heavy object held in the hand with the thumb uppermost, this muscle forms the sloping upper edge of the forearm. It is also involved in supination. It is possible to elicit a reflex by tapping the tendon of brachioradialis: this is still often known as the ‘supinator’ reflex because the old name for the muscle was supinator longus.
Extension (Fig. 12.15)
The extensor muscle of the elbow is triceps, supplied by the radial nerve (C7, 8). Attachments: scapula, humerus–ulna. Triceps has three heads:
• long, from the infraglenoid tubercle of the scapula
• lateral, from the back of the humerus, above and lateral to the radial groove, more superficial than lateral
• medial, from the back of the humerus, below and medial to the radial groove, more deep than medial.
The radial nerve thus runs through the muscle between the attachments of the lateral and medial heads to the humerus. The triceps tendon jerk (C7, 8), elicited by tapping the attachment of triceps just above the olecranon, is a commonly used neurological test (see section 12.8, p. 190).
An accessory extensor of the elbow is anconeus – entirely trivial and unimportant.
Pronation and supination (Figs 12.19, 12.21)
As described earlier, the head of the radius rotates within the annular ligament. This occurs in pronation and supination as you can demonstrate to yourself. First, flex your elbow to about 90° with the palm of your hand facing up and the thumb lateral: this is the supine position. Now turn the palm down, so that the thumb comes to be medial: this is the action of pronation and the forearm is now pronated, or in the prone position. Throughout this movement, the ulna remains almost stationary (as you can feel); it is the radius that moves with its head rotating as above and its distal (inferior) end moving in an arc over the ulna.
• Pronation: pronator teres, pronator quadratus, median nerve, C6.
• Supination: biceps and supinator, musculocutaneous and radial nerves, C5, 6.

Biceps as a supinator: using a screwdriver. With the elbow flexed at 90° the tendon of biceps approaches the bicipital tuberosity of the radius directly from above and is perfectly placed to cause rotation of the radius within the annular ligament. Also, the bicipital aponeurosis aids supination by traction on the fascia over the superficial forearm flexors. Biceps is a very powerful supinator.
Tightening a screw for a right-handed person involves supination against resistance, whereas for a left-handed person it involved pronation against resistance; this is why right-handed people are better screwers and left-handed people are better unscrewers (unless you buy special left-handed screws).
Supinator: humerus, ulna, joint capsule–radius. It is attached to the posterior surface of the proximal ulna, the back of the annular ligament and the adjacent elbow joint capsule and the lateral humeral epicondyle. It sweeps laterally and wraps itself around the lateral aspect of the radius. When it contracts it ‘unwraps’ the radius so that supination takes place. It is supplied by the radial nerve (C6) which divides into superficial and deep branches on its surface, the deep (posterior interosseous nerve) passing through the substance of the muscle as it approaches the neck of the radius (Fig. 12.3).
12.6. Flexor compartment of the forearm, carpus, carpal tunnel
The distal radius articulates with the scaphoid and lunate. The radius and scaphoid may be fractured by a fall on the outstretched hand. The radial and ulnar pulses are commonly felt at the wrist, and the surface anatomy of this region is important since it is often injured. Forearm flexor muscles are supplied by the median and ulnar nerves, and extensors by the radial nerve. Flexor tendons pass from the forearm to the hand through the carpal tunnel, which also contains the median nerve, which is therefore vulnerable in carpal tunnel syndrome.
You should:
• describe the innervation of the principal muscles acting on the wrist
• describe the surface markings of the bones, nerves and vessels at the wrist
• describe the surface markings of flexor retinaculum and its attachments
• explain the anatomy and the clinical manifestations of carpal tunnel syndrome.
Bones
Revise the cubital fossa, pronation and supination.
Interosseous membrane
This structure is attached to the interosseous borders of the radius and ulna, occupying most of the area between the bones. It separates the flexor compartment anteriorly from the extensor compartment posteriorly and helps to stabilise the two bones, playing a role in weightbearing. Some people regard it as an intermediate radioulnar joint.
Distal radius (Fig. 12.18)
Distal ulna (Fig. 12.18)
The distal end of the ulna is smaller than the proximal end. The head of the ulna is the smaller, distal, end. Note the following:
• interosseous border
• articular surface for radius
• styloid process
• distal end.
The ulna does not articulate with the carpal bones at all: between the ulna and the carpal bones is the triangular fibrocartilage of the wrist joint.
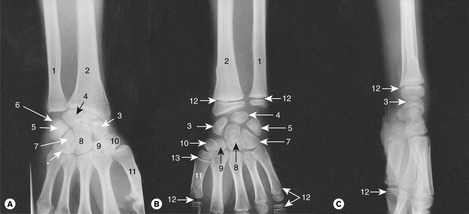
Carpal bones (Fig. 12.22)
For most bones it is simply necessary to know only the names. But you must be able to identify them on a skeleton, on a radiograph and know where to palpate the hamate, scaphoid and trapezium.
• Proximal row, radial side to ulnar side:
– Scaphoid. Articulates with the radius. Palpable in the anatomical snuffbox. The shape and blood supply of the scaphoid are important. It has a narrow waist which is prone to fracture as a result of a fall on the outstretched hand. Because the proximal portion articulates with the radius, blood vessels can enter the proximal portion only through the waist from the distal portion, and if the waist is fractured, the proximal portion may undergo avascular necrosis.
– Lunate. Articulates with the radius. May dislocate and damage the median nerve.
– Triquetral.
– Pisiform. This is actually a sesamoid bone in the tendon of flexor carpi ulnaris. It is easily palpable.
The wrist joint
It is not necessary to go into details, but you should know that the radius articulates with the scaphoid and lunate (you can see this on the distal end of the radius), and that movements take place at all the joints between the carpal bones, the radius and the metacarpals. Numerous ligaments connect the bones together: details of these are unnecessary.
Arteries, pulses
The ulnar and radial arteries arise in the cubital fossa and pass down the forearm to the wrist and hand.
• The common interosseous is an early branch of the ulnar artery. It divides into anterior and posterior interosseous arteries supplying, respectively, the flexor and extensor compartments of the forearm muscles.
• The radial pulse is palpated just proximal to the wrist joint by pressing the artery on to the anterior surface of the radius, lateral to flexor carpi radialis tendon. It is the most commonly palpated pulse. Distal to this, the radial artery passes laterally to the anatomical snuffbox.
• The ulnar pulse is also easily palpated just proximal to the wrist on the radial side of flexor carpi ulnaris tendon.
Nerves
• The ulnar nerve passes down the ulnar side of the forearm. It is vulnerable to slash wounds in the distal forearm.
• The median nerve passes more or less in the midline of the forearm (hence its name) on the posterior surface of flexor digitorum superficialis muscle. It is less vulnerable, being deep to flexor digitorum superficialis muscle and tendons.
• The radial nerve (the superficial branch: cutaneous only) passes on the radial side of the forearm.
Muscles and movements
Flexor muscles: C6, 7 (Fig. 12.23)
The forearm flexor muscles act upon the wrist joint and fingers. They are for power, unlike the small muscles of the hand (see below) which are for precision. They arise from the common flexor origin (medial epicondyle of the humerus), the proximal radius and ulna and the interosseous membrane. Precise details are not necessary. There are three groups, from superficial to deep:
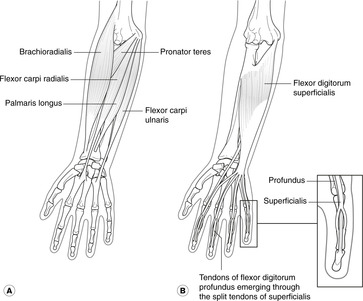
Superficial flexors (Fig. 12.23A)
Four muscles radiate from the common flexor origin. From radial to ulnar sides, these are:
• Pronator teres. Attachments: common flexor origin–mid-shaft of the radius.
• Flexor carpi radialis. Attachments: common flexor origin–first and second metacarpals. This is the large tendon on the radial side of the wrist.
• Palmaris longus. Attachments: common flexor origin–palmar aponeurosis. This is the small tendon more or less in the midline at the wrist. It may be absent on one or both sides.
• Flexor carpi ulnaris. Attachments: common flexor origin–fifth metacarpal by means of the pisiform (sesamoid bone).
Nerve supply: median nerve, except for flexor carpi ulnaris, which is supplied by the ulnar nerve.
Intermediate flexors (Fig. 12.23B)
Flexor digitorum superficialis. Attachments: radius, ulna, interosseous membrane–middle phalanx of each finger (digits 2–5). Nerve supply: median nerve, which passes immediately deep to this muscle.
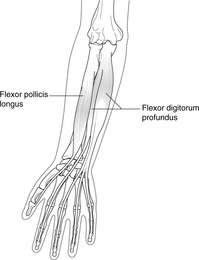
Deep flexors (Fig. 12.24):
• Flexor digitorum profundus. Attachments: radius, ulna, interosseous membrane–terminal phalanx of each finger (digits 2–5).
• Flexor pollicis longus. Attachments: radius, interosseous membrane–distal phalanx of thumb.
• Pronator quadratus. Attachments: ulna–radius. This is a quadrilateral muscle running from side to side in the distal forearm. It wraps itself over the front of the radius to attach to the lateral side of the radius, so that when it contracts it pulls the distal end of the radius over the ulna in pronation.
 |
| Fig. 12.24 |
Nerve supply: median nerve, except for the two bellies of flexor digitorum profundus to digits 4 and 5 which are supplied by the ulnar nerve.
Extensor muscles (Fig. 12.25)
These are all supplied by branches of the radial nerve. Details of these are certainly unnecessary. They include: extensor pollicis longus (thumb), extensor pollicis brevis (thumb), abductor pollicis longus (thumb), extensor digitorum (fingers); extensor indicis (the index finger is singled out for special treatment); extensor carpi radialis longus and brevis (to the metacarpals), extensor carpi ulnaris (to the metacarpals). Knowledge of detailed attachments is not necessary. Nerve supply: radial nerve, C6, 7, 8. See wrist drop (12.8, p. 190).

Anatomical snuffbox (Fig. 12.25)
Other movements
Lateral flexion in both ulnar and radial directions takes place at the radiocarpal joint. Muscles causing these movements are predictable. For example, flexor carpi radialis acts as a radial flexor when used with extensor carpi radialis muscles, but as a flexor when used with flexor carpi ulnaris.
Carpus, carpal tunnel
Wrist creases and surface anatomy
Proximal and distal wrist creases are found on the flexor aspect of the distal forearm. The distal crease marks the approximate level of the radius–scaphoid–lunate articulation. All the carpal bones are distal to the distal wrist crease.
Palpable bones are:
• scaphoid and trapezium on the radial side
• pisiform and hamate on the ulnar side.
Carpal tunnel and flexor retinaculum (Fig. 12.26)
The proximal and distal rows of carpal bones fit together forming a concavity facing anteriorly (as viewed from the palmar aspect), which is maintained by the flexor retinaculum – attached like a tiebeam to the trapezium and scaphoid laterally and the pisiform and hamate medially. Between the tiebeam and the bones is thus an enclosed space, the carpal tunnel, through which most of the structures pass between hand and forearm.
Surface markings of flexor retinaculum. These are an approximately 2 cm square immediately distal to the middle of the distal wrist crease.
Contents of the carpal tunnel
• Tendons of flexor digitorum superficialis, flexor digitorum profundus and flexor pollicis longus. (The tendon of flexor carpi radialis is in a separate compartment and is unimportant here.)
• Median nerve (the ulnar nerve passes superficial to the tunnel, not through it).
Carpal tunnel syndrome
Swelling in the carpal tunnel (for example caused by fluid retention in pregnancy), or a space-occupying lesion here, may compress the median nerve in the carpal tunnel causing:
• motor loss in the thenar muscles
• sensory changes over the palmar aspect of (usually) the radial three and a half digits.
This is carpal tunnel syndrome. The thenar muscles are involved because the thenar (or recurrent) branch of the median nerve which supplies them does not leave the main trunk of the nerve until after it has passed through the tunnel. The skin over the thenar muscles is not affected because the palmar cutaneous branch is given off by the median nerve proximal to the wrist in the forearm. Carpal tunnel syndrome may require incision of the flexor retinaculum to relieve the pressure.
Ossification of the carpal bones (Fig. 12.22)
It is sometimes useful to know that carpal bones ossify in order of size approximately annually beginning with the capitate (the largest) in year 1. The pisiform, though, does not usually ossify until about year 12. This is relevant to the radiographic appearance of the wrist of a child and may be used to assess chronological age in relation to ‘metabolic’ age.
12.7. Hand
You should:
• list the names and give the surface anatomy of all carpal bones, and be able to recognise them on radiographs
• describe the surface markings of the nerves and vessels of the hand
• describe the innervation of the thenar and hypothenar muscles
• explain the anatomical basis of dermatome testing in the hand
• explain the anatomical basis of motor nerve testing in the hand.
Digits: names or numbers?
Digit 1 is the thumb or pollux (adjective: pollicis); digit 2 is the index finger; 3 is the middle finger, 4 is the ring finger; 5 is the little finger (pinkie).
Bones (Fig. 12.22)
Revise carpal bones.
• Metacarpals 1–5
• Phalanges. The thumb (digit 1) has two phalanges, proximal and distal. The fingers (digits 2–5) have three phalanges, proximal, intermediate and distal.
Despite accepted terminology, the first metacarpal is embryologically a phalanx, so the thumb has three phalanges (like the other digits) but no metacarpal. You can see this in a radiograph of an immature hand: the epiphyseal line in the first metacarpal is distal, as for a phalanx, rather than proximal, as for a true metacarpal (Fig. 12.22).
Joints
• Carpometacarpal, metacarpophalangeal and interphalangeal joints are all synovial.
• The first carpometacarpal joint, trapezium – first metacarpal, has reciprocal saddle-shaped articular surfaces to allow for all the movements of which the thumb is capable. Involvement of this joint in a fractured first metacarpal (Bennett’s fracture) is potentially serious since poor healing may result in significant loss of mobility.
Movements and muscles
• Flexion, extension, adduction and abduction are defined differently in the thumb as compared with the fingers.
– For the fingers, these movements are as you would expect them to be.
– The thumb, though, is abducted when it is moved forwards from the anatomical position, away from and in a plane at right angles to the palm of the hand, and adducted when it is moved back again. It is extended when it is moved laterally, away from and in the same plane as the palm of the hand, and flexed when this is reversed.
• Digits 2, 4 and 5 are adducted towards the middle finger (3), and abducted away from it. The middle finger can be ‘abducted’ to both sides.
• Opposition is movement of the thumb across the palm of the hand as in bringing together the thumb and little finger. It is an important component of the precision grip.
Muscles (Fig. 12.26)
Movements of the digits are brought about by:
• the intrinsic muscles of the hand, which include:
– thenar muscles
– hypothenar muscles
– interosseous muscles
– lumbricals
• the tendons of the forearm flexors
• the tendons of the forearm extensors.
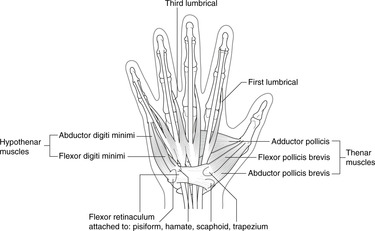
Thenar muscles (Fig. 12.26)
The fleshy mound at the base of the thumb is the thenar eminence. It contains:
• Abductor pollicis brevis. Attachments: lateral carpal bones–proximal phalanx of thumb.
• Flexor pollicis brevis. Attachments: lateral carpal bones–proximal phalanx of thumb.
• Opponens pollicis. Attachments: lateral carpal bones–lateral border of first metacarpal, so lying underneath the first two.
Nerve supply of the above three muscles: median nerve (thenar branch, see above), C8, T1.
Deep to these is the:
• Adductor pollicis. Attachments: capitate and metacarpals 2 and 3–proximal first phalanx. Nerve supply: ulnar nerve, deep branch, C8, T1.
Hypothenar muscles (Fig. 12.26)
The fleshy mound at the base of the little finger is the hypothenar eminence. It contains three muscles corresponding to the superficial thenar muscles (abductor brevis, flexor brevis, opponens) with digiti minimi substituted for pollicis. Details are not necessary. Nerve supply: ulnar nerve, C8, T1.
Long flexor tendons (Figs 12.23, 12.24)
As the tendons of flexor digitorum superficialis approach the phalanges, each splits into two components which pass on either side of the tendon of flexor digitorum profundus to attach to the intermediate phalanx, so superficialis acts at the proximal interphalangeal joint. Profundus tendon attaches to the terminal phalanx, so this muscle acts at the distal interphalangeal joint.
A similar arrangement is found in the thumb: the tendon of flexor pollicis brevis splits to let that of flexor pollicis longus pass through.
Extensor tendons (Fig. 12.25)
• Extensor carpi radialis and ulnaris tendons are attached to the dorsal surface of the metacarpals.
• Extensor digitorum tendons are attached to the dorsal aspects of all the phalanges by the dorsal extensor expansions. The details are complex and you do not need to know them.
Nerve supply: radial nerve, C6, 7
Lumbricals: straight finger flexion (Fig. 12.26)
These four muscles, like short worms (Latin: lumbricus), are attached to the tendons of flexor digitorum profundus in the region of the mid-palm. They pass on the radial side of the bones to the extensor expansion of the same digit in such a way that they flex the metacarpophalangeal joint, but because they attach to the extensor expansion, they extend the interphalangeal joints. The resultant movement is straight finger flexion. You can sometimes see a bulge (or at any rate feel something) caused by the first lumbrical (index finger) when you flex the metacarpophalangeal joint, keeping the finger straight. Nerve supply: ulnar and median nerves, two each, in accordance with the supply of flexor digitorum profundus, of which they are really extensions.
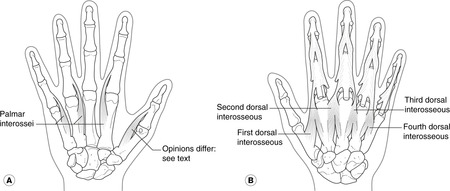
Interosseous muscles: abduction, adduction (Fig. 12.27)
Three (or four) palmar, four dorsal. Palmar interossei adduct, dorsal interossei abduct (PAD, DAB).
• Dorsal: deep to the palmar interossei. Each arises from the sides of adjacent metacarpals and the tendons pass to proximal phalanges and the extensor expansion of digits 2 (radial side), 3 (one muscle radial side, one muscle ulnar side) and 4 (ulnar side). The first dorsal interosseous is the fleshy muscle on the back of the hand between the first and second metacarpals.
 |
| Fig. 12.27 |
Nerve supply: ulnar nerve, deep branch, C8, T1
Functional considerations, nerve injuries
• The hand muscles act in concert. Fine movements, like threading a needle, or writing, depend upon fine movements of all these components.
• If you see a patient with hypothenar muscle weakness, think of ulnar nerve lesion.
• If you see a patient with thenar muscle weakness, think of median nerve lesion.
• If you see a patient with both hypothenar and thenar muscle weakness, think of brachial plexus root lesion, T1. The thenar muscles, hypothenar muscles and interossei, whether supplied by the ulnar nerve or the median nerve, are all supplied by neurons with cell bodies in the ventral grey horn of spinal cord segment T1 (and possibly C8). Damage to T1 ventral horn cells, nerve roots or T1 nerve itself (e.g. Pancoast’s tumour; see 10.4, p. 91) may present as a loss of manual dexterity.
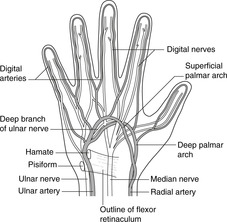
Vessels of the hand (Fig. 12.28)
Arteries
• Ulnar artery: passes from forearm to hand superficial to the flexor retinaculum, between the pisiform and hook of the hamate (both of which are palpable). It is usually the main contributor to the superficial palmar arterial arch. The deep branch, to the deep palmar arch, grooves the ulnar aspect of the hook of the hamate.
• Radial artery: passes from forearm to hand, avoiding the flexor retinaculum, by running dorsally deep to the tendons bounding the anatomical snuffbox, then penetrating the first dorsal interosseous muscle and the adductor pollicis muscle. It is usually the main contributor to the deep palmar arterial arch. Its superficial branch, to the superficial palmar arch, is superficial to the flexor retinaculum.
• Superficial and deep palmar arterial arches. Both radial and ulnar arteries usually contribute to these.
– Superficial arch: approximately level with the tip of the fully extended thumb.
– Deep arch: approximately level with the base of the extended thumb.
 |
| Fig. 12.28 |
Both arches give branches to the distal portions of the hand and the digits.
Allen’s test
Revise the positions of the radial and ulnar pulses. Ask a friend to clench his fist very tightly as if to squeeze all the blood from the palm of the hand. While the fist is still tightly clenched, press very firmly on both the radial and ulnar pulses to prevent blood from entering the palm. Now, while still pressing the arteries, tell the friend to open the fist: the palm should be very pale. Now release one of the arteries and see how long it takes for the palm to become pink again. Repeat the whole procedure, this time releasing the other artery. Amongst other things, this tests:
• the patency of the arteries
• the level of the friendship.
Veins
The only important thing to note is that the pattern of superficial veins is, as usual, very variable. There is often a dorsal venous arch on the back of the palm, from either side of which arise the cephalic and basilic veins. Look at your own hand.
Nerves of the hand
Ulnar nerve (see Fig. 12.4)
This passes superficial to the flexor retinaculum with the ulnar artery.
• Palmar and digital branches: these supply hypothenar muscles and palmar skin of the ulnar one and a half digits, and the adjacent palm.
• Dorsal branch: this is given off in the distal forearm and supplies dorsal skin of the ulnar one and a half digits.
• Deep branch: this is given off near the hamate, accompanies the deep branch of the ulnar artery, and supplies interossei and adductor pollicis.
Median nerve (see Fig. 12.4)
After giving off the palmar cutaneous branch in the forearm, which supplies skin over the thenar eminence, the median nerve passes through the carpal tunnel.
• Palmar and digital branches: these supply palmar skin of the radial three and a half digits, and the adjacent palm.
• Thenar, or recurrent, branch: this is given off distal to the flexor retinaculum, and supplies thenar eminence muscles.
Radial nerve (see Fig. 12.3)
In the hand, this is entirely sensory and there are no special points of clinical significance. The territory of the radial nerve is the dorsal skin of the radial three and a half digits (thus mirroring the median nerve).
Cutaneous overlap, variation, clinical considerations
• There is a significant degree of overlap between these cutaneous territories such that:
– the skin that is supplied only by the radial nerve is on the dorsal aspect of the first dorsal interosseous muscle
– the skin that is supplied only by the median nerve is over the thenar eminence
– the skin that is supplied only by the ulnar nerve is on the ulnar edge of the hand.
• Variations in the borders between the territories of the ulnar and median nerves are encountered.
• Weakness and wasting of the thenar muscles means a lesion of the median nerve. Weakness and wasting of the hypothenar muscles means a lesion of the ulnar nerve. Weakness and wasting of both thenar and hypothenar muscles means a lesion of T1 root, probably at the apex of the lung or in the brachial plexus. Make sure you understand this.
Palmar aponeurosis, fascial spaces
The palmar aponeurosis is a tough triangular sheet which expands from the tendon of palmaris longus. Deep to it there are several fascial ‘spaces’, important only because of infections from piercing wounds. Unfortunately, there is no standardised nomenclature, and different authorities use the same terms for different things. I suggest that:
• the thenar space contains the thenar muscles
• the hypothenar space contains the hypothenar muscles
• the midpalmar space, between the thenar and hypothenar spaces, contains the long flexor tendons and lumbricals; this space is often subdivided by thin septa
• the adductor space lies between adductor pollicis and the first dorsal interosseous muscle.
If necessary, these spaces can be drained by surgical incisions.
Dupuytren’s contracture
A thickening and shortening of part of the palmar aponeurosis may result in flexion of the metacarpophalangeal joints, usually beginning (inexplicably) with that of the ring finger. It occurs more frequently as one gets older and in certain chronic conditions (e.g. liver disease – again inexplicably).
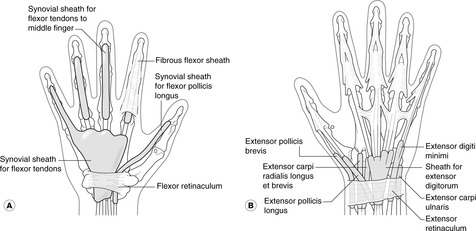
Synovial sheaths (Fig. 12.29)
Also important clinically, and for similar reasons, are the synovial sheaths or bursas of the palm. In the palm (Fig. 12.29A) the common synovial sheath extends through the carpal tunnel into the forearm, and inflammation of the sheath is a potential cause of carpal tunnel syndrome. Dorsally (Fig. 12.29B), synovial sheaths surround the extensor tendons as they pass deep to the restraining extensor retinaculum (of which you need to know nothing other than that it exists). These sheaths may be inflamed in, for example, racquet players and others who habitually flex and extend their wrists more than most of us.
A fall on the outstretched hand may cause:
• fractured clavicle
• Colles’ fracture (distal radius)
• fractured scaphoid: tenderness in the anatomical snuffbox
• dislocated lunate: median nerve injury
• Bennett’s fracture (first metacarpal)
• mid-shaft humeral fracture: radial nerve damage.
12.8. Innervation, nerve testing, surface anatomy
Nerves: a revision of some important points
Dermatomes (see Fig. 6.6, p. 36)
Remember these:
• C5 over deltoid
• C6 over the thumb
• C8 on the medial forearm
• T1, 2 axillary skin.
Sensory nerves
• Over deltoid:
– axillary nerve.
• Anterior arm:
– axillary nerve (laterally)
– medial cutaneous nerve of the arm.
• Anterior forearm:
– lateral cutaneous nerve of the forearm (continuation of musculocutaneous)
– medial cutaneous nerve of the forearm.
• Posterior arm and forearm:
– branches of radial nerve.
• Hand:
– radial nerve: dorsum of radial three and a half digits
– ulnar nerve: dorsal and palmar aspects of ulnar one and a half digits
– median nerve: palmar aspect of radial three and a half digits.
Segmental values for upper limb movements (Table 12.1)
The most frequently tested upper limb reflexes can be remembered thus: biceps jerk C5, 6; triceps jerk C7, 8.
Sites where injuries may damage upper limb nerves (Figs 12.3, 12.4)
• Shoulder dislocation: axillary nerve.
• Fractured surgical neck of humerus: axillary nerve.
• Fractured mid-shaft of humerus: radial nerve.
• Medial epicondyle of humerus: ulnar nerve.
• Neck of radius, fracture or dislocation: deep branch of radial (posterior interosseous) nerve.
• Slashed wrist: ulnar nerve, palmar cutaneous branch of median nerve.
• Dislocated lunate: median nerve.
• Stabbing in thenar eminence: thenar branch of median nerve (thenar muscles).
Nerve injuries
• Upper trunk of brachial plexus (C5, 6), e.g. from forcible separation of the shoulder (downward) and the neck (as in a motorcycle accident, or during a difficult birth): deltoid, biceps and brachialis are all affected, so the arm is adducted, extended and pronated (‘waiter’s tip’ position). This is Erb’s paralysis.
• Radial nerve: wrist drop. Since the radial nerve supplies all the extensors including those of the wrist, damage to it causes the forelimb to adopt a characteristic position with a flexed, limp wrist. In this state, grip strength is lost since for maximum power in the digital long flexors, the wrist has to be held in extension. Radial nerve damage may occur:
– in the arm, e.g. from a mid-shaft fracture of the humerus: wrist drop, elbow extension also affected, inability to extend fingers.
– at the elbow, e.g. from dislocation of the superior radioulnar joint: wrist drop, inability to extend fingers.
• Ulnar nerve:
– at the elbow, e.g. from trauma at the medial epicondyle (this is ‘banging the funny bone’). Because the median and ulnar nerves both supply forearm muscles, there is no dramatic motor loss except for abduction and adduction of the fingers, though there may be some clumsiness. There is no very characteristic appearance.
– at the wrist, e.g. from slashed wrist: see above. In this case, though, the finger flexors supplied by the ulnar nerve are not affected (they are in the forearm) and so the ring and little fingers will be more flexed than if the nerve is sectioned at the elbow. Paradoxically, therefore, the hand looks ‘worse’ although fewer muscles are inactivated. Some people refer to this as the ulnar paradox.
• Median nerve
– in the cubital fossa, e.g. from a supracondylar humeral fracture.
– at the wrist, e.g. from carpal tunnel syndrome. As with ulnar nerve lesions, there is no dramatic motor loss or very characteristic appearance.
• T1 segment or nerve root, e.g. from Pancoast’s tumour: paralysis of the intrinsic muscles of the hand with loss of manual dexterity (see 10.4, p. 91).
Testing peripheral nerves
• Musculocutaneous: skin on lateral side of forearm, biceps tendon reflex.
• Axillary: skin over humeral attachment of deltoid, shoulder abduction.
• Radial: skin over first dorsal interosseous muscle, wrist or elbow extension.
• Median: ask the patient to abduct the thumb against resistance.
• Ulnar: finger abduction/adduction – try to stop the patient spreading the fingers (abduction, dorsal interossei), ask the patient to grasp a sheet of paper between the fingers without using the thumb (adduction, palmar interossei).
Testing spinal segments
• C5, 6: biceps tendon jerk; skin over lateral side of arm.
• C7, 8: triceps tendon jerk; skin over centre and medial side of forearm and hand.
• T1: finger abduction/adduction, thumb opposition; skin of medial side of arm, axilla.
| Joint | Movement | Segmental value |
|---|---|---|
| Shoulder | Abduction, lateral rotation | C5 |
| Adduction, medial rotation | C6, 7, 8 | |
| Elbow | Flexion | C5, 6 |
| Extension | C7, 8 | |
| Forearm | Pronation | C6 |
| Supination | C5, 6 | |
| Wrist | Flexion | C6, 7 |
| Extension | C6, 7 | |
| Fingers | Flexion, extension (long muscles) | C7, 8 |
| Hand | Intrinsic muscles | T1 |
Revise dermatomes: Figure 6.6 (p. 36)
Is it a dermatome/myotome lesion or a peripheral nerve lesion?
Because of the brachial plexus, the main nerves to the limb (e.g. radial, ulnar, median) carry fibres from several spinal cord segments. You may have to decide whether a patient’s sensory and/or motor loss signifies a dermatome/myotome problem, such as a spinal cord or spinal nerve root lesion, or a peripheral nerve condition, such as nerve damage more distally.
• If the symptoms are confined to a single dermatome (allowing for overlap and variation) the condition probably results from a nerve root or spinal cord lesion in or near the vertebral column (that is, proximal to the plexus).
• If the symptoms are spread over several dermatomes but are all in the same region, the condition probably results from a peripheral nerve lesion (that is, distal to the plexus).
Surface anatomy: a revision of some important points
Shoulder, axilla
• Most lateral bony point: greater tuberosity of humerus except in shoulder dislocations when it is the acromion process.
• Acromioclavicular joint and coracoid process palpable.
• Deltopectoral triangle: cephalic vein passes deep, lymph nodes may be palpable.
• Axillary lymph nodes may be palpable.
• Long thoracic nerve on medial wall of axilla, more or less vertical in the midaxillary line.
Arm, cubital fossa and elbow region
• Biceps tendon and aponeurosis.
• Brachial pulse: medial to biceps tendon, with median nerve medial to the pulse.
• Ulnar nerve: behind medial epicondyle.
• Head of the radius palpable about 1.5 cm distal to the lateral epicondyle.
Wrist and hand
• Radial pulse: just proximal to the wrist joint lateral to flexor carpi radialis tendon.
• Ulnar pulse: just proximal to the wrist on the radial side of flexor carpi ulnaris tendon.
• Flexor retinaculum: about 2 cm square in the midline just distal to the distal wrist crease – it is in the hand not the forearm.
• Anatomical snuffbox: scaphoid, trapezium, radial artery.
• Pisiform and hook of hamate are palpable.
• Superficial palmar arterial arch: level with tip of fully extended thumb.
• Deep palmar arterial arch: level with base of extended thumb.
Single best answer questions
For each numbered question, only ONE of the options lettered a–d is correct
26. Concerning the hand and carpal region:
a. a dislocated lunate may damage the median nerve in the carpal tunnel.
b. lumbricals extend metacarpophalangeal joints.
c. the capitate is the last carpal bone to ossify.
d. the pisiform bone is palpable on the lateral side of the wrist.
27. The following symptoms and signs in the upper limb could be caused by a nerve lesion as stated:
a. anaesthesia over deltoid – brachial plexus lower trunk lesion.
b. hyporeflexia of the biceps tendon reflex – C4 lesion.
c. loss of digital dexterity – T1 lesion.
d. weakness of shoulder abduction – musculocutaneous nerve lesion.
28. Concerning the hand and carpal region:
a. hypothenar muscles are supplied by the nerve that passes through the carpal tunnel.
b. the flexor retinaculum is attached to the pisiform, hamate, scaphoid and trapezoid bones.
d. the scaphoid bone is palpable in the anatomical snuff box.
29. In the hand:
a. the radial nerve supplies the first dorsal interosseous muscle.
b. the radial nerve supplies the palmar skin of the three radial digits.
c. the radial nerve supplies the skin on the dorsal aspect of the first dorsal interosseous muscle.
d. the superficial palmar arterial arch is formed mainly by the radial artery.
30. Concerning joints and related structures of the pectoral girdle:
a. after fracture of the clavicle, the medial portion is lower than the lateral.
b. the sternoclavicular joint is cartilaginous.
c. the sternoclavicular joint overlies the union of the internal jugular and subclavian veins.
d. the subacromial bursa normally communicates with the shoulder joint.
31. At the elbow and in the cubital fossa:
a. biceps is the principal elbow flexor.
b. brachialis is attached to the olecranon process of the ulna.
c. the brachial pulse is palpable immediately medial to the biceps tendon.
d. the head of the ulna is surrounded by the annular ligament.
32. In the shoulder region:
a. paralysis of serratus anterior muscle causes weakened abduction of the shoulder.
b. the radial nerve is at risk in dislocation of the shoulder.
c. the shoulder is a very stable joint.
d. the surgical neck of the humerus is within the shoulder joint cavity.
33. Nerve damage at the given site is likely to be associated with the stated lesion:
a. carpal tunnel – inability to grip paper between straightened fingers.
b. medial epicondyle – hypothenar anaesthesia.
c. midshaft humerus – weakness of shoulder abduction.
d. midshaft humerus – wrist drop.
34. Damage C5 root of the brachial plexus would most likely impair:
a. cutaneous sensation of the axilla.
b. cutaneous sensation of the medial arm.
c. shoulder abduction.
d. elbow flexion.
35. Left-handed people are better unscrewers than screwers (assuming normal screws) because:
a. biceps is a powerful pronator.
b. biceps is a powerful supinator.
c. supination is weaker than pronation.
d. they always use power tools.
Matching item questions
Questions 36–45: nerves and vessels
Match the numbered item to the lettered response. Each lettered response may be used once, more than once, or not at all.
a. axillary artery
b. subclavian artery
c. related to the spiral groove of the humerus
d. related to the medial humeral epicondyle
e. related to the surgical neck of the humerus
36. vertebral artery
37. lateral thoracic artery
38. internal thoracic artery
39. profunda brachii artery
40. thoracoacromial artery
41. nerve supplying shoulder abductor muscle
42. nerve supplying hypothenar muscles
43. nerve which when sectioned would give wrist drop
44. nerve supplying skin on the dorsum of the little finger
45. abduction of the fingers
Questions 46–50: spinal segments
Match the numbered item to the lettered response. Each lettered response may be used once, more than once, or not at all.
a. C5, 6
b. C7, 8
c. T1
d. branch of nerve involved in carpal tunnel syndrome
e. nerve damaged by dislocated lunate
46. hypothenar muscles
47. biceps tendon reflex.
48. triceps tendon reflex
49. axillary skin
50. upper trunk of brachial plexus
Questions requiring short answers
51. Describe the factors responsible for maintaining stability of the shoulder joint.
52. Describe the axilla and the structures passing through it. Why is it important clinically?
53. How may blood in the subclavian artery reach the axillary artery following occlusion of the third part of the subclavian artery?
54. Name the muscles that are attached to the bicipital groove of the humerus. Give the innervation and function of each.
55. Describe the attachments, function and innervation of biceps brachii muscle.
56. Explain why a left-handed person is likely to find it more difficult to tighten screws with a manual screwdriver than a right-handed person.
57. Explain why, when you forcibly pull a child by the hand, there is more likely to be nerve damage than in an adult. Which nerve is involved, and what would be the consequence?
58. Describe the anatomical basis of carpal tunnel syndrome.
59. How is the hand supplied with arterial blood? Where may peripheral pulses easily be palpated in this region? What is Allen’s test?
60. In the hand:
a. how would you test the sensory function of the ulnar, median and radial nerves?
b. how would you test the motor function of each nerve?
Single best answers
26. a.
27. c.
28. d.
29. c.
30. c.
31. c.
32. a.
33. b.
34. c.
35. b. (though d would be wise, I guess).
Matching item answers
36. b.
37. a.
38. b.
39. c.
40. a.
41. e. The axillary nerve, which passes from medial to lateral behind the surgical neck of the humerus, supplies the deltoid muscle.
42. d. The ulnar nerve passes posterior to the medial epicondyle to supply muscles of the hand.
43. c. The radial nerve is close to the bone in the spiral groove of the humerus, where it may be damaged by midshaft fractures.
44. d. The ulnar nerve supplies skin on the ulnar side of the hand.
45. d.
46. c.
47. a.
48. b.
49. c.
50. a.
Short answers
51. Stability at the shoulder joint is maintained by rotator cuff muscles (supraspinatus, infraspinatus, subscapularis, teres minor) and glenohumeral ligaments. These are important and should be elaborated giving, if you have time, the attachments of the muscles and their nerve supply. The glenoid labrum has a minor role.
52. Describe the distorted pyramidal shape, the anterior and posterior axillary folds and the floor. The important contents are the brachial plexus, axillary artery and branches, and lymph nodes, which you could describe in some detail. No account of the axilla should omit its relevance to the spread of breast cancer. See section 12.4 (p. 175).
53. The scapular anastomosis may be involved in bypassing a blocked distal subclavian artery. Blood from the subclavian passes into branches which communicate with the anastomosis round the scapula, e.g. dorsal scapular artery, internal thoracic artery (via intercostals and connections). Blood passes the ‘wrong way’ up the subscapular artery and reaches the third part of the axillary artery. See also Figure 10.25 (p. 88).
54. Latissimus dorsi and teres major are attached to the floor and medial edge of the bicipital groove of the humerus; pectoralis major is attached to its lateral edge. The nerve supply of latissimus dorsi and teres major is through branches of the posterior cord of the brachial plexus. Their functions are shoulder adduction, extension, and medial rotation. Pectoralis major, supplied by medial and lateral pectoral nerves, flexes and adducts the shoulder.
55. The long head of biceps brachii is attached to the supraglenoid tubercle, and the tendon passes inside the capsule of the shoulder joint to the bicipital groove of the humerus. The short head is attached to the coracoid process of the scapula. Distally the attachment is to the bicipital tuberosity of the radius. The muscle functions as a flexor and supinator at the elbow, and as a flexor at the shoulder. Nerve supply is by the musculocutaneous nerve, C5, 6.
56. See Biceps as a supinator: using a screwdriver (12.5, p. 179).
58. The median nerve passes through the carpal tunnel and may be compressed within it. This would result in altered sensation (e.g. tingling, numbness) in the cutaneous distribution of the nerve (palmar aspect of hand and radial three and a half digits, but not over the thenar eminence because the branch that supplies this comes off in the forearm, before the nerve reaches the carpal tunnel), and weakness or paralysis of the muscles supplied distal to the carpal tunnel (thenar muscles). This is most easily tested by opposition of the thumb.
59. Blood supply to the hand is via the radial and ulnar arteries, which form deep and superficial arches. See Allen’s test in section 12.7 (p. 188).
60.
a. Sensory function is tested as follows:
• median nerve – skin over thenar eminence
• ulnar nerve – skin over medial edge of palm
• radial nerve – skin on dorsal aspect of first dorsal interosseous.
b. Motor function is tested as follows:
• median nerve – abduction of the thumb against resistance
• ulnar nerve – abduction and adduction of the fingers
• radial nerve – extension of the wrist or fingers.