[level-membership-for-neonatal-and-perinatal-medicine-category]
29 Tissue Doppler Imaging in the Fetus
I. HOW TISSUE DOPPLER WORKS
A. Blood versus tissue velocities
1. One of the new techniques that is being investigated in many centers is myocardial velocities as a way to assess fetal ventricular function. Grouped together, these techniques are jointly known as tissue Doppler.
2. The movements of the myocardium are much slower than the flow of blood into and out of the ventricles.
a. Inflow and outflow velocities in the human fetus are in the range of 0.5 to 1.0 m/s (50-100 cm/s).
b. Myocardial velocities, albeit stronger signals, average about one tenth of these velocities, ranging from 0.05 to 0.1 m/s (5-10 cm/s).
2. These low-velocity signals are complex in their orientation due to the three-dimensional (3-D) nature of ventricular contraction.
B. Heart motion
a. Classically, ventricular function has been described as radial changes in diameter (fractional shortening).
b. Radial change is the difference in the diastolic and systolic dimensions divided by the diastolic dimension.
c. These movements are known as radial changes in dimension and are accompanied by longitudinal ones (base-to-apex changes).
d. Each radial motion is not in just one plane but in two. Thus, the complex spatial movements of the heart require simplification into simple linear movements.
a. The normal movement of the heart is for the base to move downward toward the apex in systole.
b. Following this, the muscle actively relaxes back upward in a biphasic pattern of early and late diastolic movements.
c. These are analogous to the biphasic nature of the velocities of ventricular inflow, the E and A waves of early and late diastole.
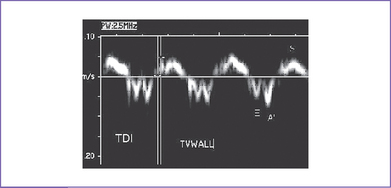
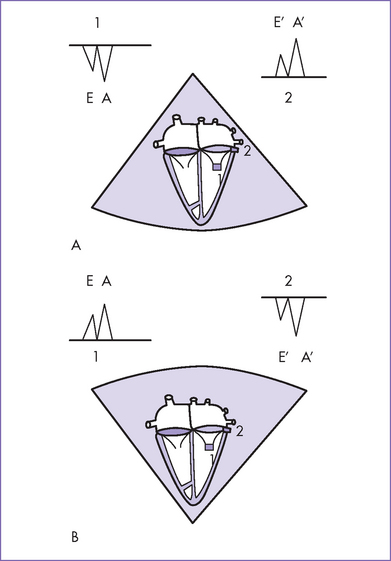
d. E and A waves in the fetus always have a pattern such that the A wave is larger than the E wave (Fig. 29-1).
e. It is intriguing to find that the longitudinal myocardial tissue Doppler velocities in the fetus are similar to the E’ wave or early diastolic relaxation velocity, being smaller than the later diastolic A’ velocity (Fig. 29-2).
II. NORMAL AND ABNORMAL VALUES
A. Normal values
1. Early results in examining normal changes of longitudinal myocardial velocities with increasing gestational age have appeared recently.
2. In both ventricles, there were significant correlations between tissue Doppler E’/A and pulsed Doppler E/A. In the left ventricle (LV), r = 0.56; in the right ventricle (RV), r = 0.60 (P < 0.01).
3. Assessment of myocardial tissue velocities in fetuses was feasible with tissue Doppler imaging.
4. Age-related alterations in tissue Doppler velocities might suggest age-related maturational changes in diastolic function. Reference charts were constructed by Chan and colleagues (2005).
B. Tissue doppler in abnormal fetuses
1. Aoki and colleagues (2004) studied fetuses with and without heart failure.
a. Compared with control fetuses, the mean E’ was significantly lower and the mean E was significantly higher in fetuses with heart failure, although these parameters did overlap between the two groups.
b. The mean RV myocardial wall-motion velocity during atrial contraction, ratio of E’ to A’ for RV myocardial wall motion velocity during atrial contraction, and RV myocardial wall motion velocity during systole did not differ between the two groups.
c. In fetuses with heart failure compared with control fetuses:
d. In addition, the DTI–Tei index z score was greater than 2 in all fetuses with heart failure.
2. They concluded that although DTI velocities were not sufficiently sensitive to identify fetuses with heart failure versus control fetuses, the DTI–Tei index and E/E’ were useful and sensitive indicators of global RV dysfunction.
III. FUTURE DIRECTIONS
A. Challenges
1. Fetal tissue Doppler is so new that the technology to accurately measure these velocities is still in development.
2. There has been no validating experimental work to assess these ventricular wall changes by other techniques and to calibrate, so to speak, our ultrasound machines. A recent paper studied the TO1 changes with fetal acidosis.
a. The gross spatial movement of the heart with systole and diastole is not of interest in quantifying myocardial velocities and actually contaminates the required signal.
b. New methods to subtract these velocities are currently being developed.
B. Tissue doppler gating
1. In a study by Brekke and colleagues (2004), tissue Doppler gating was introduced.
a. In this technique, tissue Doppler data are used to calculate a gating signal.
b. They applied this cardiac gating method to dynamic 3-D reconstructions of the heart of eight fetuses aged 20 to 24 weeks.
c. The gating signal was derived from the amplitude and frequency contents of the tissue Doppler signal.
d. They then used this signal as a replacement for ECG in a 3-D volume reconstruction and visualization, using techniques established in ECG-gated 3-D echocardiography.
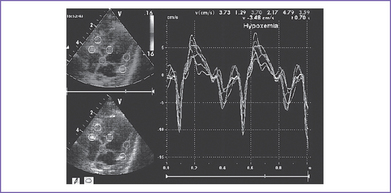
2. Fetal lamb models have the potential for correlative studies of the meaning of changes in the myocardial velocities during changes in ventricular loading (Fig. 29-3).
IV. TAKE-HOME MESSAGE
1. Assessment of myocardial tissue velocities in fetuses is feasible with tissue Doppler imaging.
2. Age-related alterations in tissue Doppler velocities might suggest age-related maturational changes in diastolic function.
3. Fetal tissue Doppler is a promising new technology; however, validating experimental work is needed to assess these ventricular wall changes by other techniques and to calibrate our ultrasound machines.
Acharya G, Räsänen J, Mäkikallio K, et al. Metabolic acidosis decreases fetal myocardial isovolumic velocities in a chronic sheep model of increased placental vascular resistance. Am J Physiol Heart Circ. 2007;294(1):H498-H504. Epub
Aoki M, Harada K, Ogawa M, et al. Quantitative assessment of right ventricular function using Doppler tissue imaging in fetuses with and without heart failure. J Am Soc Echocardiogr. 2004;17(1):28-35.
Brekke S, Tegnander E, Torp HG, et al. Tissue Doppler gated (TDOG) dynamic three-dimensional ultrasound imaging of the fetal heart. Ultrasound Obstet Gynecol. 2004;24(2):192-198.
Chan LY, Fok WY, Wong JT, et al. Reference charts of gestation-specific tissue Doppler imaging indices of systolic and diastolic functions in the normal fetal heart. Am Heart J. 2005;150(4):750-755.
Harada K, Tsuda A, Orino T, et al. Tissue Doppler imaging in the normal fetus. Int J Cardiol. 1999;71(3):227-234.
Huhta JC, Kales E, Casbohm A. Fetal tissue Doppler—a new technique for perinatal cardiology. Curr Opin Pediatr. 2003;15(5):472-474.
[/level-membership-for-neonatal-and-perinatal-medicine-category][not-level-membership-for-neonatal-and-perinatal-medicine-category]
29 Tissue Doppler Imaging in the Fetus
I. HOW TISSUE DOPPLER WORKS
A. Blood versus tissue velocities
1. One of the new techniques that is being investigated in many centers is myocardial velocities as a way to assess fetal ventricular function. Grouped together, these techniques are jointly known as tissue Doppler.
2. The movements of the myocardium are much slower than the flow of blood into and out of the ventricles.
a. Inflow and outflow velocities in the human fetus are in the range of 0.5 to 1.0 m/s (50-100 cm/s).
b. Myocardial velocities, albeit stronger signals, average about one tenth of these velocities, ranging from 0.05 to 0.1 m/s (5-10 cm/s).
2. These low-velocity signals are complex in their orientation due to the three-dimensional (3-D) nature of ventricular contraction.
B. Heart motion
a. Classically, ventricular function has been described as radial changes in diameter (fractional shortening).
b. Radial change is the difference in the diastolic and systolic dimensions divided by the diastolic dimension.
c. These movements are known as radial changes in dimension and are accompanied by longitudinal ones (base-to-apex changes).
d. Each radial motion is not in just one plane but in two. Thus, the complex spatial movements of the heart require simplification into simple linear movements.
a. The normal movement of the heart is for the base to move downward toward the apex in systole.
b. Following this, the muscle actively relaxes back upward in a biphasic pattern of early and late diastolic movements.
c. These are analogous to the biphasic nature of the velocities of ventricular inflow, the E and A waves of early and late diastole.
d. E and A waves in the fetus always have a pattern such that the A wave is larger than the E wave (Fig. 29-1).
e. It is intriguing to find that the longitudinal myocardial tissue Doppler velocities in the fetus are similar to the E’ wave or early diastolic relaxation velocity, being smaller than the later diastolic A’ velocity (Fig. 29-2).
