28 Fetal Three-Dimensional Echocardiography
I. WHY A FETAL SCAN IS A CHALLENGE
A. Obstacles
1. In the pediatric or adult patient, predetermined windows are used to obtain standardized views of the heart.
2. Obstacles to views in the fetus.
a. The size of the heart varies as a function of gestational age.
b. The fetal position can vary during the examination.
c. Fetal movement during the examination can result in not acquiring all of the diagnostic images for analysis.
B. Evaluation
1. For effective conversation with the parents, interpretation must be done in real time, either during the examination or quickly after reviewing digital records.
2. Given these potential obstacles, evaluation of the fetal heart is one of the most challenging diagnostic tasks the fetal examiner encounters during an early second- or third-trimester ultrasound examination.
II. OVERVIEW
A. Superiority to two-dimensional echocardiography
1. Accurate quantification of:
a. Volumes of the right ventricle (RV) and left ventricle (LV).
c. LV ejection fraction without the need for geometric assumptions.
a. Spatial relations between cardiac structures, which is important when assessing complex congenital heart disease.
III. THREE-DIMENSIONAL TERMINOLOGY AND PHYSICS
B. Physics
a. It is generally stated that the human eye and brain retain a visual impression for about 1/10 to 1/30 of a second, equivalent to a frame or volume rate of 10 to 30 Hz.
b. The exact time depends on the brightness and clarity of the image and pattern recognition.
c. When referring to real-time imaging, we are actually talking about whether an imaging system can achieve the visual continuity that will satisfy the human eye and brain.
2. Built-in, spatial, and temporal realignment of 4-D data.
a. It is hard to consistently find a stationary volume of interest in utero due to unwanted patient movements (e.g., fetal activity, maternal respiration) and/or environmental movements such as abdominal deformation from probe movement when using conventional approaches.
b. Real-time 3-D systems can acquire a volume data set without manual displacement of the transducer.
3. Sufficient temporal resolution for the time scale of interest.
a. For general analysis of dynamic anatomy of the fetal heart, a minimum volume rate of about 15 to 25 Hz is required with fetal heart rates of 150 bpm or more. This is equivalent to a maximum of 40 ms for each imaging volume sampling period.
b. Except for isovolumetric contraction and relaxation, other cardiac phases each rarely last longer than 80 ms (rounded numbers are used in this discussion for mathematical simplicity) and can be fully sampled at least once in one imaging volume per cardiac cycle.
c. To achieve 90% accuracy for the measurement, a 500-Hz volume rate may be necessary.
IV. THREE-DIMENSIONAL ECHOCARDIOGRAPHY SYSTEMS
A. Rapidly oscillating cross-sectional transducer
a. Volumetric scanning is less dependent on the angle of acquisition, and thus less dependent on fetal lie or operator expertise, than 2-D scanning.
b. The most promising aspect is the possibility of storing and compressing a volume of 4-D information for later offline evaluation by an expert.
c. Because the heart is beating, nongated acquisition produces artifacts in the reconstructed volume data.
2. Spatiotemporal image correlation (STIC).
B. Matrix-array transducer
1. Philips Sonos 7500 System with Live 3D Echo: The recently developed full-matrix array transducer (x4 xMatrix; Philips Medical Systems, Andover, Mass.) can circumvent many of the above-mentioned limitations.
a. This probe uses approximately 3000 elements, resulting in image quality that is comparable with traditional phased-array transducers. In contrast to the sparse array probe, the full-matrix array transducer uses all its channels to transmit ultrasound pulses.
b. As a result, this transducer has:
c. This novel transducer provides instantaneous 3-D volume-rendered images on the ultrasound system and can display two simultaneous 2-D imaging planes (biplane imaging).
d. Biplane imaging can help to decrease the time required to:
2. The present technology has lower than optimal frequency because most fetal heart scans are performed at a frequency of 5 to 8 MHz (Fig. 28-2).
V. ACQUIRING LIVE THREE-DIMENSIONAL VIEWS
A. Using acquisition modes with a matrix-array transducer
1. A narrow-angled acquisition.
a. In this mode, a 60- by 30–degree pyramidal scan is acquired in real time without the need for respiratory gating.
b. This mode enables the operator to rapidly visualize cardiac structures in three dimensions using familiar 2-D-like cut planes.
c. Manipulation of threshold (gain and time gain control [TGC]) is often required for optimal visualization of cardiac structures in three dimensions.
2. Magnified view of the narrow-angled acquisition display for assessment of valvar structures in the fetal heart.
a. In this mode, the operator defines a region of interest, which is magnified into a 30 by 30–degree pyramidal volume in high resolution.
b. Images of the heart valves acquired in this manner provide unique views that are not readily obtainable using conventional 2-D echocardiography.
3. A wide-angled acquisition can be performed to collect the entire cardiac volume over 60 by 60 degrees of:
a. 3-D for color Doppler images over 4 beats.
b. 4-D for color Doppler images over 7 beats.
4. With the wide-angled transducer, it is possible to change image resolution during narrow-angle and wide-angle imaging, which in turn affects the size of the volume imaged. The LV (apical four-, three-, and two-chamber format) is usually acquired using a wide-angled acquisition.
B. Using the rapidly oscillating cross-sectional transducer
1. As an alternative to spatiotemporal realignment methods, several of these manufacturers have adopted mechanical rapid sweeping of the transducer array to show fetal behavior, changing facial expressions, and other movements.
2. Some of these methods, with sweep rates up to 25 per second, can be used to image the moving fetal heart in 4-D, and they are better than STIC at times when fetal motion and respiration are a problem for the longer slower sweeps used for STIC.
3. These are interim solutions while these manufacturers are developing more advanced matrix-array technology.
VI. CLINICAL APPLICATIONS OF THREE-DIMENSIONAL ECHOCARDIOGRAPHY
A. Quantification of biventricular function
1. Multiple studies of adult heart images have found 3-D LV volumes, ejection fractions, and mass values to be comparable with values obtained with nuclear imaging and magnetic resonance imaging (MRI).
2. Because gated-acquisition methods (including free-hand scanning) are tedious, time consuming, and relatively more portable, calculations of LV ejection fraction from 3-D reconstructions have not been incorporated into routine echocardiographic studies (Fig. 28-3).
3. In one study using the Philips Sonos 7500 system, we could quantify fetal ventricular volumes between 18 and 38 weeks’ gestation.
a. Both RV and LV volume measurements for the live 3-D scans correlated closely with fetal gestational age (r = 0.86 [RV], r = 0.80 [LV]).
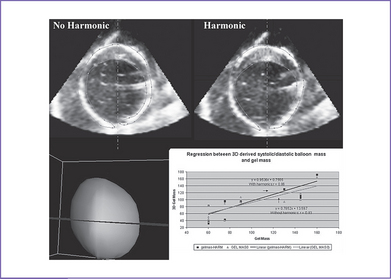
b. A study of pulsating balloon phantoms we have performed suggests that live 3-D is accurate enough to compute volumes greater than 0.5 mL (Fig. 28-4).
c. In contrast to 2-D echocardiography, 3-D echocardiography does not rely on geometric assumptions, which is a real advantage in ventricles with complex shapes and wall-motion abnormalities.
d. Similarly, due to the complex geometrical shape of the RV, quantification is not performed using traditional echocardiographic methods.
e. Three-dimensional echocardiography has the potential to overcome these limitations, resulting in accurate measurements of LV size and function.
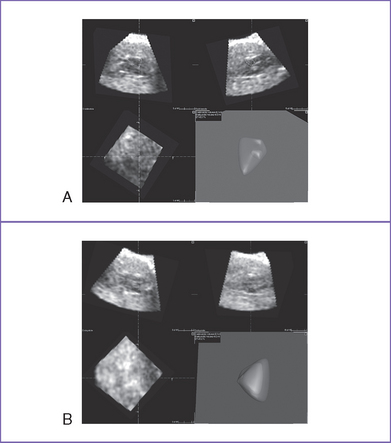
Fig. 28-3 Left (A) and right (B) ventricular (LV and RV) volume reconstruction (offline) with TomTec software in a 24-week fetus with a normal heart. Note that the stroke volume and fractional shortening are automatically generated by the software. See also color version of Fig. 28-3A in color insert.
B. Valvar assessment
1. Using the spark-gap method of acquisition, 3-D echocardiography investigators have described the mitral valve annulus and leaflet relationship as nonplanar. With 3-D, the diagnosis of mitral valve prolapse was refined because it was possible not only to identify the prolapsing scallop but also to measure the extent of the defect.
2. Three-dimensional echocardiography might also aid in the evaluation of aortic valve disease. Bicuspid aortic valves can be readily imaged from both the aortic and outflow tract orientations. As resolution improves, estimation of the effective aortic valve area in fetuses with aortic stenosis will be possible.
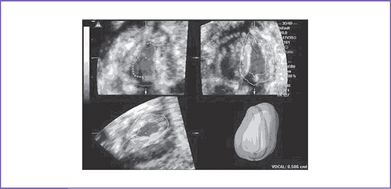
3. Pulmonic valves are also difficult to image (Fig. 28-5). However, with this technique it is possible to obtain unique views of the pulmonic valve from the pulmonary artery as well as the tricuspid valve leaflets and annulus, which are impossible to obtain during a routine 2-D examination.
4. The addition of 3-D color flow will further enhance the ability of this technique to evaluate traces of valvar flow events.

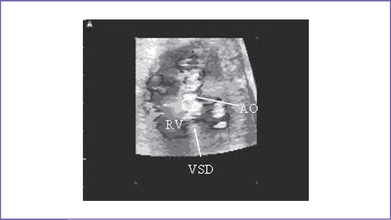
C. Congenital abnormalities of the heart
1. Fetal 3-D imaging of these abnormalities enables localization and en-face measurement of the VSD area.
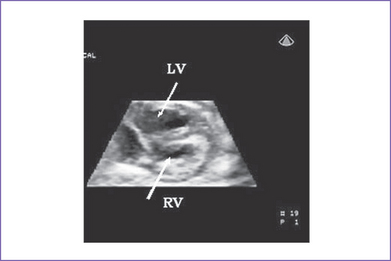
2. The 3-D echocardiography might also identify complex congenital heart disease in utero, as in our cases of transposition of great arteries, double outlet RV, tetralogy of Fallot (Fig. 28-6), hypoplastic right heart, and others.
3. The addition of 3-D color flow will further enhance the ability of this technique to differentiate left-to-right shunt in utero, as demonstrated in our study, including restricted atrial foramen ovale or retrograde aortic arch filling in hypoplastic left heart syndrome.
4. This information is of major significance in timing of delivery and in counseling women and couples with complex congenital heart diseases diagnosed prenatally.
VII. REAL-TIME THREE-DIMENSIONAL SYSTEMS
A. Advantages
1. They provide the examiner with a huge number of images for review.
2. They allow correlation between image planes that are perpendicular to the main image acquisition plane.
3. They can shorten the evaluation time, especially when complex heart defects are suspected.
4. They enable the reconstruction of a 3-D rendered image that contains depth and volume, which can provide additional information that is not available from the thin 2-D image slices.
5. The data volume can be stored and reviewed offline by the examiner or it can be viewed by experts at a remote site.
6. They allow the examiner to review all images in a cineloop format.
B. Disadvantages
1. Images are acquired over multiple heart cycles.
2. Data processing is slow and time consuming and requires a considerable degree of skill and understanding.
3. Calculation of LV volumes was performed on offline systems that required manual tracing of endocardial borders.
4. The 3-D data sets were displayed using static wire-frame or surface-rendered reconstructions. Although this display mode failed to provide anatomic detail, this was not a critical issue when calculating volumes or frequency below that displayed using static wire-frame or surface-rendered reconstructions.
VIII. FUTURE DIRECTIONS
1. In the next few years, real-time 3-D and 4-D echocardiography with color-flow Doppler will become part of the routine echocardiographic examination.
2. In the near future, 3-D will become available to improve our ability to quantify the severity of different valvar lesions.
3. Further miniaturization and increase in frequency of the matrix-array transducer technology or production of other types of transducers (annular arrays, curved matrix) will enable the visualization of real-time 3-D and 4-D for a larger portion of fetal heart studies.
4. Performing 3-D or 4-D transvaginal first-trimester echocardiography is potentially feasible.
IX. TAKE-HOME MESSAGE
1. Three-dimensional data can be considered a bank of information from which different aspects and details can be extracted in the future, at the same or a different site or center, and by the same or a different specialist.
2. The aortic arch and venous anatomy features that are typically challenging in 2-D studies often can be developed with ease, regardless of fetal lie, in 3-D echocardiography.
3. Fetal color 3-D studies combine morphology with directional and velocity information to aid imaging of fetal anatomy and cardiac function.
Belohlavek M, Tanabe K, Jakrapanichakul D, et al. Rapid three-dimensional echocardiography: Clinically feasible alternative for precise and accurate measurement of left ventricular volumes. Circulation. 2001;103(24):2882-2884.
Bhat AH, Corbett V, Carpenter N, et al. Fetal ventricular mass determination on three-dimensional echocardiography: Studies in normal fetuses and validation experiments. Circulation. 2004;110(9):1054-1060.
Bonnet D, Coltri A, Butera G, et al. Detection of transposition of the great arteries in fetuses reduces neonatal morbidity and mortality. Circulation. 1999;99(7):916-918.
Deng J, Sullivan ID, Yates R, et al. Real-time three-dimensional fetal echocardiography—optimal imaging windows. Ultrasound Med Biol. 2002;28(9):1099-1105.
DeVore GR, Falkensammer P, Sklansky MS, Platt LD. Spatio-temporal image correlation (STIC): New technology for evaluation of the fetal heart. Ultrasound Obstet Gynecol. 2003;22(4):380-387.
Garne E, Stoll C, Clementi M. Evaluation of prenatal diagnosis of congenital heart diseases by ultrasound: Experience from 20 European registries. Ultrasound Obstet Gynecol. 2001;17(5):386-391.
Gopal AS, Schnellbaecher MJ, Shen Z, et al. Freehand three-dimensional echocardiography for determination of left ventricular volume and mass in patients with abnormal ventricles: Comparison with magnetic resonance imaging. J Am Soc Echocardiogr. 1997;10(8):853-861.
Handke M, Schafer DM, Heinrichs G, et al. Quantitative assessment of aortic stenosis by three-dimensional anyplane and three-dimensional volume-rendered echocardiography. Echocardiography. 2002;19(1):45-53.
Hull AD, James G, Salerno CC, et al. Three-dimensional ultrasonography and assessment of the first-trimester fetus. J Ultrasound Med. 2001;20(4):287-293.
Jiang L, Levine RA, Weyman AE. Echocardiographic assessment of right ventricular volume and function. Echocardiography. 1997;14(2):189-206.
Kasprzak JD, Salustri A, Roelandt JR, Ten Cate FJ. Three-dimensional echocardiography of the aortic valve: Feasibility, clinical potential, and limitations. Echocardiography. 1998;15(2):127-138.
Levine RA, Handschumacher MD, Sanfilippo AJ, et al. Three-dimensional echocardiographic reconstruction of the mitral valve, with implications for the diagnosis of mitral valve prolapse. Circulation. 1989;80(3):589-598.
Li X, Ashraf M, Thiele K, et al. A novel method for the assessment of the accuracy of computing laminar flow stroke volumes using a real-time 3D ultrasound system: In vitro studies. Eur J Echocardiogr. 2005;6(6):396-404.
Michailidis GD, Simpson JM, Karidas C, Economides DL. Detailed three-dimensional fetal echocardiography facilitated by an Internet link. Ultrasound Obstet Gynecol. 2001;18(4):325-328.
Nelson TR, Pretorius DH, Sklansky M, Hagen-Ansert S. Three-dimensional echocardiographic evaluation of fetal heart anatomy and function: Acquisition, analysis, and display. J Ultrasound Med. 1996;15(1):1-9.
Nixon JV, Saffer SI, Lipscomb K, Blomqvist CG. Three-dimensional echoventriculography. Am Heart J. 1983;106(3):435-443.
Schindera ST, Mehwald PS, Sahn DJ, Kececioglu D. Accuracy of real-time three-dimensional echocardiography for quantifying right ventricular volume: static and pulsatile flow studies in an anatomic in vitro model. J Ultrasound Med. 2002;21(10):1069-1075.
Siu SC, Levine RA, Rivera JM, et al. Three-dimensional echocardiography improves noninvasive assessment of left ventricular volume and performance. Am Heart J. 1995;130(4):812-822.
Verheijen PM, Lisowski LA, Stoutenbeek P, et al. Prenatal diagnosis of congenital heart disease affects preoperative acidosis in the newborn patient. J Thorac Cardiovasc Surg. 2001;121(4):798-803.






