[level-membership-for-dermatology-category]
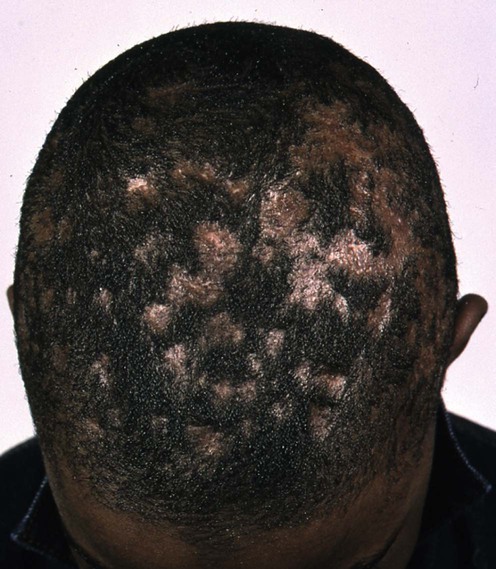
Tinea capitis
Specific investigations



First-line therapies
 Griseofulvin
Griseofulvin Terbinafine
Terbinafine Itraconazole
ItraconazoleSecond-line therapies
 Fluconazole
Fluconazole Short-duration terbinafine
Short-duration terbinafine Short-duration itraconazole
Short-duration itraconazoleThird-line therapies
 2% ketoconazole
2% ketoconazole Selenium sulfide shampoo
Selenium sulfide shampoo Prednisolone
Prednisolone
[/level-membership-for-dermatology-category][not-level-membership-for-dermatology-category]
Tinea capitis
Specific investigations
Tinea capitis: predictive value of symptoms and time to cure with griseofulvin treatment.
Lorch-Dauk KC, Comrov E, Blumer JL, O’Riordan MA, Furman LM. Clin Pediatr 2010; 49: 280–6.
Buy Membership for Dermatology Category to continue reading. Learn more here
[/not-level-membership-for-dermatology-category]
