The pharmacology of atropine, scopolamine, and glycopyrrolate
Scopolamine
Scopolamine, another belladonna alkaloid, sometimes referred to as hyoscine, has stronger antisalivary actions and much more potent central nervous system effects than does atropine (Table 84-1). It is a strong amnesic that usually also produces sedation. Restlessness and delirium are not unusual and can make patients difficult to manage. Elderly patients who take scopolamine are at risk for incurring injury from falls when unsupervised. Scopolamine produces less cardiac acceleration than does atropine, and both drugs can produce paradoxical bradycardia when used in low doses, possibly through a weak peripheral cholinergic agonist effect.
Table 84-1
Duration of Action and Effects of Atropine, Scopolamine, and Glycopyrrolate
| Duration | Effect | |||||
| Drug | IV | IM | CNS | GI Tone | Antisialagogue | HR |
| Atropine | 5-30 min | 2-4 h | Stimulation | – – | + | +++* |
| Scopolamine | 0.5-1 h | 4-6 h | Sedation† | − | +++ | 0/+* |
| Glycopyrrolate | 2-4 h | 6-8 h | None | – – – | ++++ | + |
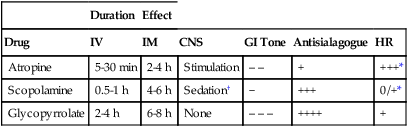
†CNS effects often manifest as sedation before stimulation.
Adapted, with permission, from Lawson NW, Meyer J. Autonomic nervous system physiology and pharmacology. In: Barash PG, Cullen BF, Stoelting RF, eds. Clinical Anesthesia. 3rd ed. Philadelphia; Lippincott Williams & Wilkins: 1997:243-327.
Glycopyrrolate
Glycopyrrolate is a synthetic antimuscarinic with a quaternary ammonium with anticholinergic properties similar to those of atropine (see Table 84-1); however, unlike atropine, glycopyrrolate is completely ionized at physiologic pH.



