Chapter 177 Stabilization of the Subaxial Cervical Spine (C3–C7)
Fusions by anterior approaches have been widely used in cervical spine injuries, allowing anterior decompression of the spinal column. Anterior fusion techniques were first introduced in 1955 by Smith and Robinson1 and then popularized by Cloward.2
The first application of a metal plate as a supplement to an anterior bone graft in cases of cervical dislocation was performed in 1975 by Herrmann.3 In 1980, Böhler4 also used small plates as proposed by Orozco and Llovet.5 In 1980 Caspar subsequently popularized the use of anterior cervical plates, resulting in more widespread use of Caspar plating6,7 in the mid-1980s in both Europe and the United States.8
Anterior Stabilization Techniques
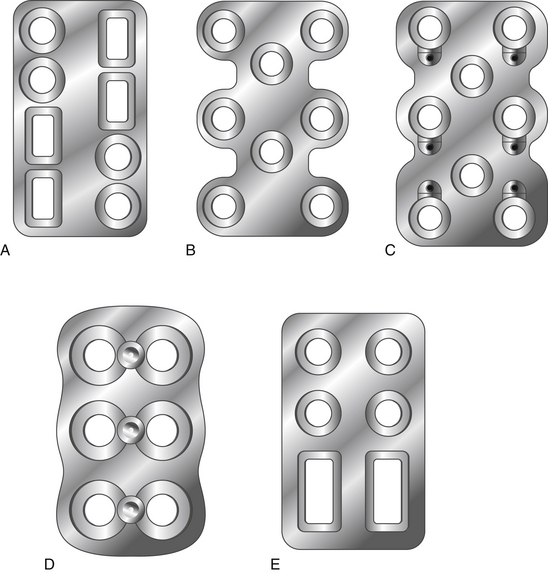
Anterior cervical plates have significantly changed since their early application in cervical trauma. They are now commonplace in anterior cervical decompression and fusion (ACDF) procedures, especially in cases requiring decompression of two or more levels. Routine use for the treatment of cervical spondylosis has caused plate design to change significantly in recent years. The first anterior cervical plates were unlocked and required bicortical purchase. Anterior cervical plates with constrained designs and locking plate–screw head connections then came into favor.9 The latest plates are semiconstrained dynamic plates that allow some movement in rotation and translation (Fig. 177-1).
Biomechanics of Cervical Plates
Screw choice and insertion technique also affect the biomechanical properties of anterior plating. For instance, hollow screws with small holes on the shaft were developed to allow improved osteointegration at the screw–bone interface.10 They were removed from the market because of high screw fracture rates and increased difficulty of removal.
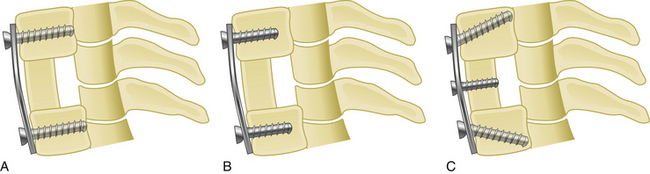
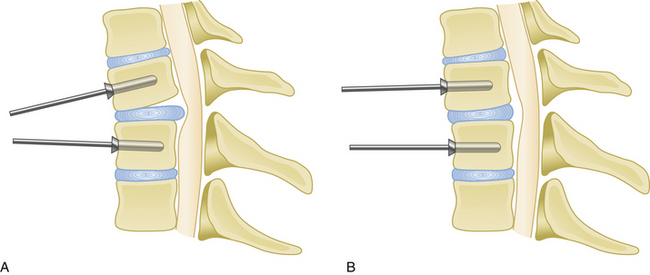
Medial or lateral angulation of anterior screws during insertion results in a triangulation in the axial plane, whereas cranial and caudal angulation results in sagittal plane triangulation. Varying the angle of trajectory provides improved construct strength and lessens the risk that the screw will back out (Fig. 177-2).
Although anterior cervical plates have undergone many improvements since their introduction, several questions still remain regarding the clinical application of this technique. Such questions include the following: Which plate should be used, constrained or nonconstrained? Should screws be placed in a unicortical or bicortical fashion? Should a screw be placed into the interbody bone graft? In the case of cervical corpectomy, should intermediate points of fixation should be added to improve construct stability?
Types of Plates
Static Plates
Second-generation plates are constrained plates (static plates). Constrained plates provide strong fixation between the plate surface and the screw heads. Examples include Synthes cervical spine locking plates (CSLPs), Orion plates, and Atlantis plates. These plates employ a fixed moment arm cantilever beam design. Screw backout is restricted in these models.11,12 The CSLP is an example of a second-generation anterior cervical plate and was first introduced by Morscher with fixed-angle screws. Small set screws are placed into the main screw heads, widening the screw head and locking the head to the plate. The CSLP variable-angle plate is a modification that allows up to 20 degrees of variability in the plate–screw angle. Other anterior cervical locking plates in this category use a special screw head design that expands when it incorporates into the plate.
Dynamic Plates
Third-generation plates are semiconstrained plates (dynamic) plates. These plates have designs that allow a variable amount of graft subsidence. Subsidence is observed during aging and after spine surgery and is accepted as a naturally occurring process. Although anterior cervical plates help to stabilize the spine, they also constrict subsidence. For that reason, an anterior plate that carries most of the axial load instead of sharing it with the bone graft has a high rate of failure.13 Dynamic plates were developed to avoid the late complications of rigid plates.
Screw loosening and screw and plate fracture are more common in cases of multilevel fusion with either a corpectomy or ACDF grafts.3 The main reason is graft absorbtion resulting in subsidence. Although it is a gradual process, if the loss of graft height cannot be accommodated by the plate–screw angle, the screw has increased risk of fracture.
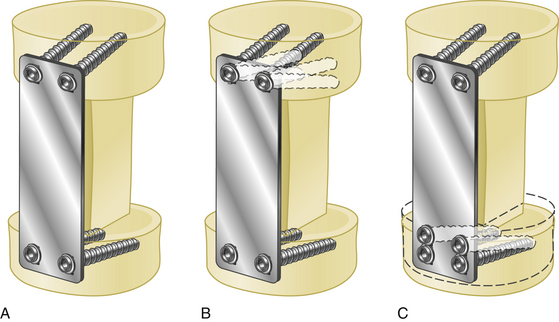
Such dynamic plates now restrict screw backout while also allowing some variability in translational and rotational movements. There are two main two kinds of dynamic anterior cervical plates manufactured by the spinal device companies, rotational and translational. In the semiconstrained rotational design, variable-angle screw systems allow the screws to toggle inside the bone. This rotational movement can also lead to instrumentation failure (Fig. 177-3). Examples include anterior cervical plates from Codman, Blackstone, Acufix, Zephir, and Atlantis (hybrid and variable). The semiconstrained translational design allows translational motion that is provided by the plate–screw interface. Examples include the ABC plate, DOC system, and Premier plate.
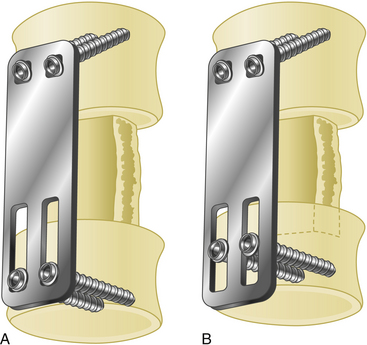
Dynamic implants allow natural subsidence to occur (Fig. 177-4) while effectively stabilizing the spine by preventing excessive movements in translation and rotation. Load sharing helps improve normal bone healing, resulting in earlier fusion. Decreased rates of construct failure have been reported with dynamic implants.13
Advantages and Disadvantages of Anterior Cervical Plates
Advantages
Anterior cervical plates have the following advantages:
• They augment stabilization, enhancing the likelihood of a solid fusion.
• They reduce the need for external bracing or halo vest placement, and they allow mobilization of the adjacent spinal segments.
• They reduce the risk of graft extrusion.
• They significantly reduce the rate of nonunion. Nonunion rates range from 11% to 63% in multilevel interbody fusion cases and from 25% to 45% in corpectomy and strut graft applications.14
If a cervical kyphosis is not severe, an anterior plate can also be used to reduce it. This is achieved by spreading the disc space with a vertebral body spreader, followed by lordotic graft and plate placement (Fig. 177-5).
Indications
Anterior cervical plates have been widely used in cases of trauma and after anterior corpectomy for cervical spondylotic myelopathy. 3,7,14,15 Anterior cervical plate placement is indicated in the following conditions:
• Cervical spine trauma with anterior column injury
• Cases of cervical spondylotic myelopathy requiring anterior decompression via ACDF
• In anterior surgery in patients who have been previously treated with a cervical laminectomy
• Following decompression and stabilization of cervical spine tumors involving the anterior column
• In post-laminectomy kyphosis following anterior decompression
In his first series, Caspar used plates only in cases of cervical trauma.6 This has given way to widespread use in cervical tumors and following decompressive surgery for cervical disc disease.7 In the case of plating following cervical corpectomy, vertebral body reconstruction can be performed using bone autograft or allograft, polymethyl methacrylate, or nonexpandable or expandable cages.
The diagnosis of cervical instability requires a subjective evaluation. White and Panjabi have developed a scoring system to easily determine spinal instability (Table 177-1).
Table 177-1 Instability Criteria of Subaxial Cervical Spine Injuries26
| Criteria | Point Value∗ |
|---|---|
| Anterior elements, nonfunctional | 2 |
| Posterior elements, nonfunctional | 2 |
| Sagittal plane translation > 3.5 mm | 2 |
| Sagittal plane angulation > 11 degrees | 2 |
| Positive stretch test | 2 |
| Spinal cord injury | 2 |
| Nerve root injury | 1 |
| Abnormal disc-space narrowing | 1 |
| Dangerous loading anticipated | 1 |
Related posts:
 Hearing Prosthetics: Surgical Techniques
Hearing Prosthetics: Surgical Techniques
 Surgical Management of Cerebrospinal Fluid Leakage after Spinal Surgery
Surgical Management of Cerebrospinal Fluid Leakage after Spinal Surgery
 Surgical Management of Sphenoid Wing Meningiomas
Surgical Management of Sphenoid Wing Meningiomas
 Surgical Management of Chronic Subdural Hematoma in Adults
Surgical Management of Chronic Subdural Hematoma in Adults
 Arachnoid, Suprasellar, and Rathke’s Cleft Cysts
Arachnoid, Suprasellar, and Rathke’s Cleft Cysts
 Management of Skull Base Trauma
Management of Skull Base Trauma
