CHAPTER 11 Small Bowel Resection
Case Study
Supine and upright abdominal radiographs show dilated loops of small bowel, air–fluid levels, and minimal air in the colon, consistent with a small bowel obstruction. A computed tomography (CT) scan of the abdomen and pelvis shows dilated loops of small bowel and a point of transition to collapsed bowel in the right lower quadrant (Fig. 11-1).


INDICATIONS FOR SMALL BOWEL RESECTION
PREOPERATIVE EVALUATION
The preoperative evaluation for a small bowel resection frequently includes:
COMPONENTS OF THE PROCEDURE
Preoperative Considerations
Incision and Exposure
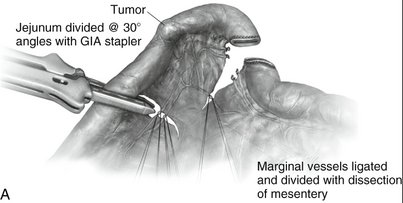
Resection
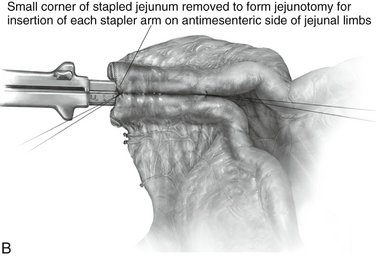
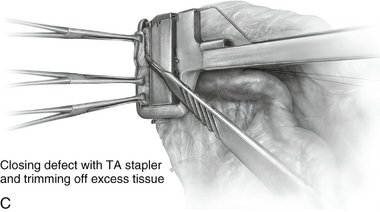
Stapled Anastomosis
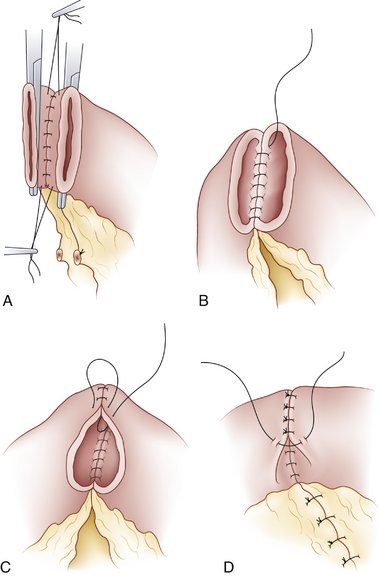
Hand-Sewn Anastomosis
POTENTIAL COMPLICATIONS
Dayton MT. Small bowel obstruction. In: Cameron JL, editor. Current Surgical Therapy. 8th ed. Philadelphia: Mosby; 2004:105-110.
Evers BM. Small intestine. In: Townsend CM, Beauchamp RD, Evers BM, Mattox KL, editors. Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice. 17th ed. Philadelphia: Saunders; 2004:1323-1380.
Liu KJM, Walker FW. Surgical procedures on the small intestines. In: Zuidema GD, editor. Shackelford’s Surgery of the Alimentary Tract. 3rd ed. Philadelphia: Saunders; 1991:264-285.
Smith CE. Gastrointestinal surgery. In: Rothrock JC, McEwen DR, editors. Alexander’s Care of the Patient in Surgery. 13th ed. St. Louis: Mosby; 2007:297-355.