[level-membership-for-rheumatology-category]Chapter 5
Shoulder Complex
Periarticular Connective Tissue and Other Supporting Structures
Scapulothoracic Posture and its Effect on Static Stability
Overall Kinematics of Shoulder Abduction: Establishing the Six Kinematic Principles of the Shoulder Complex
Innervation of the Muscles and Joints of the Shoulder Complex
Action of the Shoulder Muscles
Muscles of the Scapulothoracic Joint
Muscles That Elevate the Arm at the Glenohumeral Joint
Upward Rotators at the Scapulothoracic Joint
Function of the Rotator Cuff Muscles during Elevation of the Arm
The study of the upper extremity begins with the shoulder complex, a set of four articulations involving the sternum, clavicle, ribs, scapula, and humerus (Figure 5-1). This series of joints provides extensive range of motion to the upper extremity, thereby increasing the ability to reach and manipulate objects. Trauma or disease often limits shoulder motion, causing a significant reduction in the effectiveness of the entire upper limb.
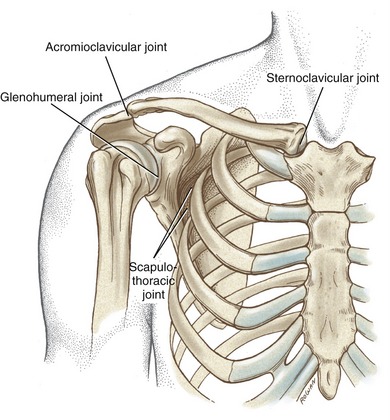
FIGURE 5-1. The joints of the right shoulder complex.
OSTEOLOGY
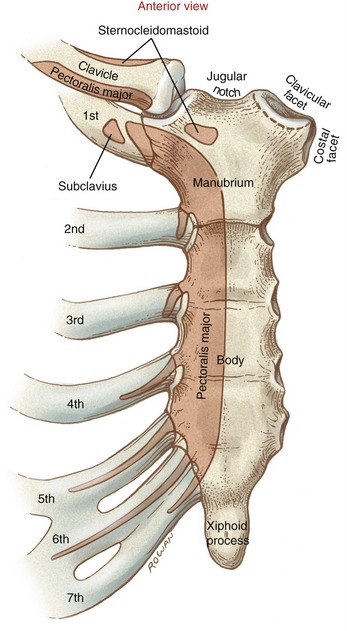
The sternum consists of the manubrium, body, and xiphoid process (Figure 5-2). The manubrium possesses a pair of oval-shaped clavicular facets, which articulate with the clavicles. The costal facets, located on the lateral edge of the manubrium, provide bilateral attachment sites for the first two ribs. The jugular notch is located at the superior aspect of the manubrium, between the clavicular facets.
Clavicle
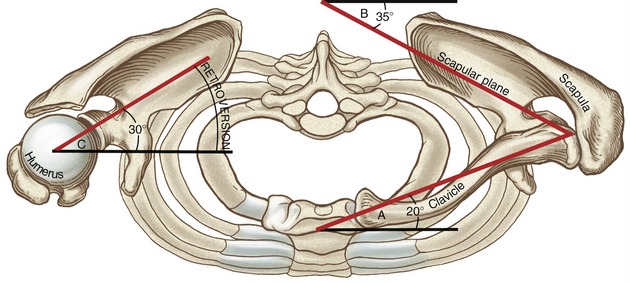
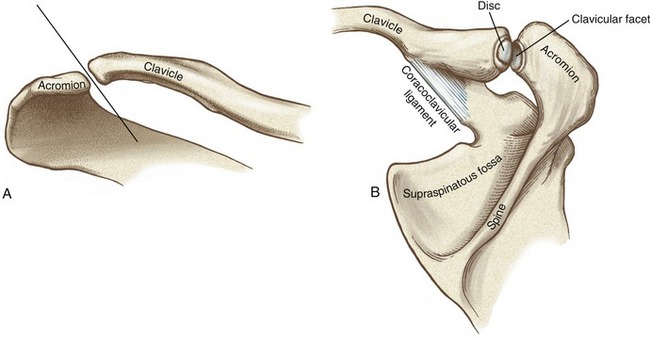
When one looks from above, it is evident that the shaft of the clavicle is curved, with its anterior surface being generally convex medially and concave laterally (Figure 5-3). With the arm in the anatomic position, the long axis of the clavicle is oriented slightly above the horizontal plane and about 20 degrees posterior to the frontal plane (Figure 5-4; angle A). The rounded and prominent medial or sternal end of the clavicle articulates with the sternum (see Figure 5-3). The costal facet of the clavicle (see Figure 5-3; inferior surface) rests against the first rib. Lateral and slightly posterior to the costal facet is the distinct costal tuberosity, an attachment for the costoclavicular ligament.
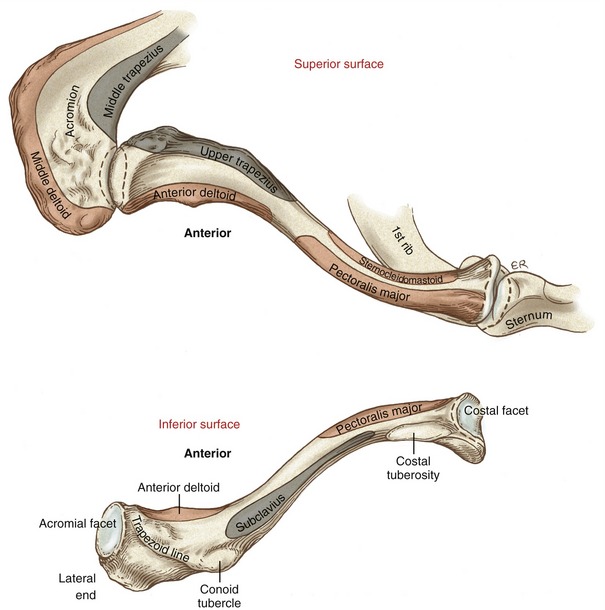
The lateral or acromial end of the clavicle articulates with the scapula at the oval-shaped acromial facet (see Figure 5-3; inferior surface). The inferior surface of the lateral end of the clavicle is well marked by the conoid tubercle and the trapezoid line.
Scapula
The triangular-shaped scapula has three angles: inferior, superior, and lateral (Figure 5-5). Palpation of the inferior angle provides a convenient method for following the movement of the scapula during arm motion. The scapula also has three borders. With the arm resting by the side, the medial or vertebral border runs almost parallel to the spinal column. The lateral or axillary border runs from the inferior angle to the lateral angle of the scapula. The superior border extends from the superior angle laterally toward the coracoid process.
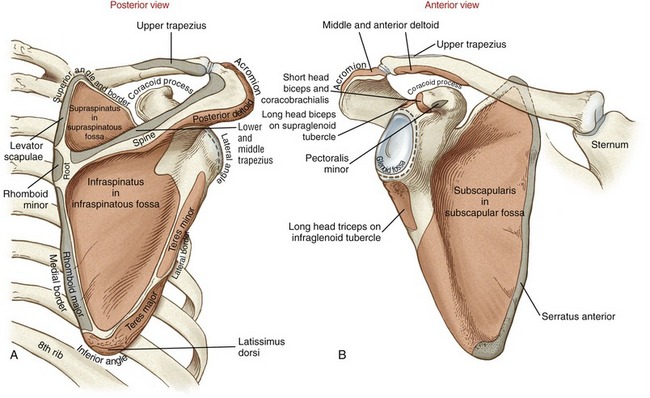
The posterior surface of the scapula is separated into a supraspinatous fossa and an infraspinatous fossa by the prominent spine. The depth of the supraspinatous fossa is filled by the supraspinatus muscle. The medial end of the spine diminishes in height at the root of the spine. In contrast, the lateral end of the spine gains considerable height and flattens into the broad and prominent acromion (from the Greek akros, meaning topmost, highest). The acromion extends in a lateral and anterior direction, forming a horizontal shelf over the glenoid fossa. The clavicular facet on the acromion forms part of the acromioclavicular joint (see Figure 5-16, B).
The scapula articulates with the head of the humerus at the slightly concave glenoid fossa (from the Greek root glene, socket of joint, + eidos, resembling) (see Figure 5-5, B). The slope of the glenoid fossa is inclined upward about 4 degrees relative to a horizontal axis through the body of the scapula.26 This inclination is highly variable, ranging from a downward inclination of 7 degrees to an upward inclination of nearly 16 degrees. At rest the scapula is normally positioned against the posterior-lateral surface of the thorax, with the glenoid fossa facing about 35 degrees anterior to the frontal plane (see Figure 5-4; angle B). This orientation of the scapula is referred to as the scapular plane. The scapula and humerus tend to follow this plane when the arm is naturally raised overhead.
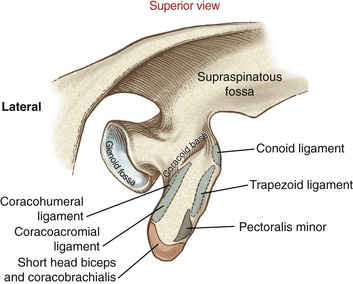
Located at the superior and inferior rim of the glenoid fossa are the supraglenoid and infraglenoid tubercles. These tubercles serve as the proximal attachment for the long head of the biceps and triceps brachii, respectively (see Figure 5-5, B). Near the superior rim of the glenoid fossa is the prominent coracoid process, meaning “the shape of a crow’s beak.” The coracoid process projects sharply from the scapula, providing multiple attachments for ligaments and muscles (Figure 5-6). The subscapular fossa is located on the anterior surface of the scapula (see Figure 5-5, B). The concavity within the fossa is filled with the thick subscapularis muscle.
Proximal-to-Mid Humerus
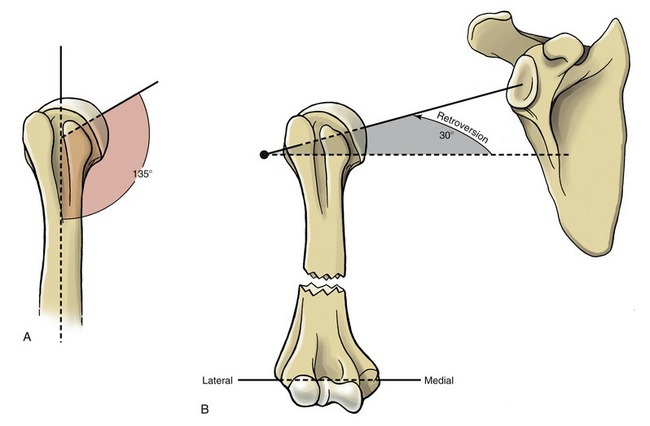
The head of the humerus, nearly one half of a full sphere, forms the convex component of the glenohumeral joint (Figure 5-7). The head faces medially and superiorly, forming an approximate 135-degree angle of inclination with the long axis of the humeral shaft (Figure 5-8, A). Relative to a medial-lateral axis through the elbow, the humeral head is rotated posteriorly about 30 degrees within the horizontal plane (see Figure 5-8, B). This rotation, known as retroversion (from the Latin retro, backward, + verto, to turn) aligns the humeral head within the scapular plane for articulation with the glenoid fossa (see Figure 5-4; angle C). Interestingly, researchers have shown that the dominant shoulder in elite baseball pitchers possesses greater humeral retroversion than the nondominant limb.24 This difference (which was not present in a control group of nonpitchers) was theorized to occur as an osseous adaptation to the large torsional stress generated during pitching.
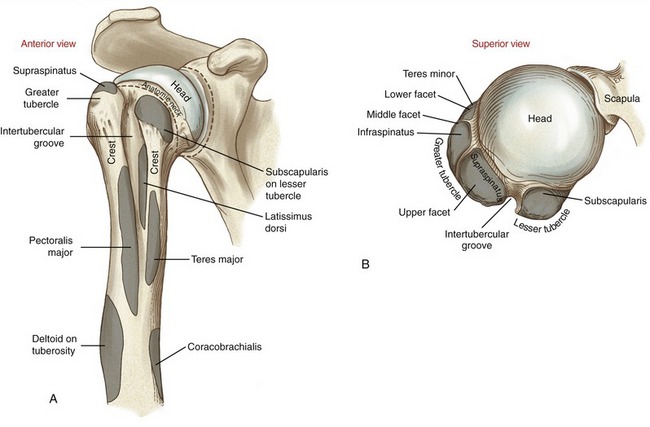
The anatomic neck of the humerus separates the smooth articular surface of the head from the proximal shaft (see Figure 5-7, A). The prominent lesser and greater tubercles surround the anterior and lateral circumference of the extreme proximal end of the humerus (see Figure 5-7, B). The lesser tubercle projects rather sharply and anteriorly for attachment of the subscapularis. The large and rounded greater tubercle has an upper, middle, and lower facet, marking the distal attachment of the supraspinatus, infraspinatus, and teres minor, respectively (see Figure 5-7, B and Figure 5-9).
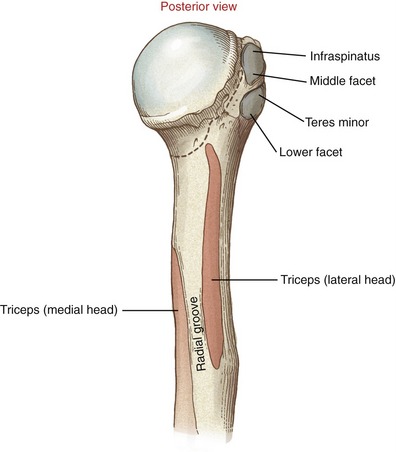
Sharp crests extend distally from the anterior side of the greater and lesser tubercles. These crests receive the distal attachments of the pectoralis major and teres major (see Figure 5-7, A). Between these crests is the intertubercular (bicipital) groove, which houses the tendon of the long head of the biceps brachii. The latissimus dorsi muscle attaches to the floor of the intertubercular groove, medial to the biceps tendon. Distal and lateral to the termination of the intertubercular groove is the deltoid tuberosity.
The radial (spiral) groove runs obliquely across the posterior surface of the humerus. The groove separates the proximal attachments of the lateral and medial head of the triceps (see Figure 5-9). Traveling distally, the radial nerve spirals around the posterior side of the humerus in the radial groove, heading toward the distal-lateral side of the humerus.
ARTHROLOGY
The most proximal articulation within the shoulder complex is the sternoclavicular joint (see Figure 5-1). The clavicle, through its attachment to the sternum, functions as a mechanical strut, or prop, holding the scapula at a relatively constant distance from the trunk. Located at the lateral end of the clavicle is the acromioclavicular joint. This joint, and associated ligaments, firmly attaches the scapula to the clavicle. The anterior surface of the scapula rests against the posterior-lateral surface of the thorax, forming the scapulothoracic joint. This articulation is not a true anatomic joint; rather, it is an interface between bones. Movements at the scapulothoracic joint are mechanically linked to the movements at both the sternoclavicular and acromioclavicular joints. The position of the scapula on the thorax provides a base of operation for the glenohumeral joint, the most distal and mobile link of the complex. The term “shoulder movement” describes the combined motions at both the glenohumeral and the scapulothoracic joints.
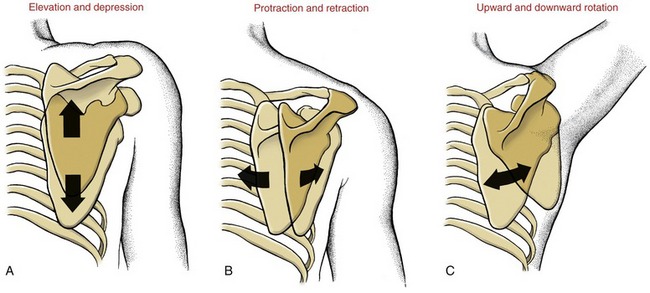
Before the kinematics of the sternoclavicular and acromioclavicular joints are described, the movements at the scapulothoracic joint must be defined (Figure 5-10). Primary movements at the scapulothoracic joint are traditionally described as elevation and depression, protraction and retraction, and upward and downward rotation. Additional movements of the scapula will be defined as the chapter unfolds.
Sternoclavicular Joint
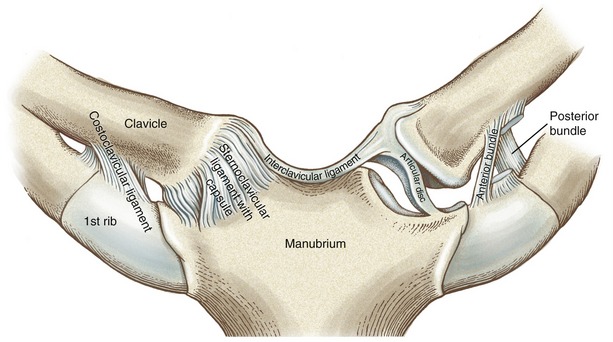
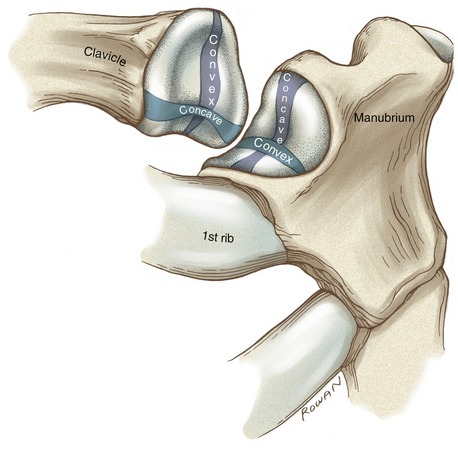
The sternoclavicular (SC) joint is a complex articulation, involving the medial end of the clavicle, the clavicular facet on the sternum, and the superior border of the cartilage of the first rib (Figure 5-11). The SC joint functions as the basilar joint of the entire upper extremity, linking the appendicular skeleton with the axial skeleton. The joint therefore must be firmly attached while simultaneously allowing considerable range of movement. These seemingly paradoxic functions are accomplished through extensive periarticular connective tissues, and an irregular saddle-shaped articular surface (Figure 5-12). Although highly variable, the medial end of the clavicle is usually convex along its longitudinal diameter and concave along its transverse diameter.178 The clavicular facet on the sternum typically is reciprocally shaped, with a slightly concave longitudinal diameter and a slightly convex transverse diameter.
PERIARTICULAR CONNECTIVE TISSUE
The SC joint is enclosed by a capsule reinforced by anterior and posterior sternoclavicular ligaments (see Figure 5-11).177 When active, muscles add further stability to the joint: anteriorly by the sternocleidomastoid, posteriorly by the sternothyroid and sternohyoid, and inferiorly by the subclavius. The interclavicular ligament spans the jugular notch, connecting the medial end of the right and left clavicles.
The costoclavicular ligament is a strong structure extending from the cartilage of the first rib to the costal tuberosity on the inferior surface of the clavicle. The ligament has two distinct fiber bundles running perpendicular to each other.178 The anterior bundle runs obliquely in a superior and lateral direction, and the posterior bundle runs obliquely in a superior and medial direction (see Figure 5-11). The crisscrossing of fibers assists with stabilizing the joint through all motions, except for a downward movement of the clavicle (i.e., depression).
The articular disc at the SC joint separates the joint into distinct medial and lateral joint cavities (see Figure 5-11).178 The disc is a flattened piece of fibrocartilage that attaches inferiorly near the lateral edge of the clavicular facet and superiorly at the sternal end of the clavicle and interclavicular ligament. The remaining outer edge of the disc attaches to the internal surface of the capsule. The disc not only strengthens the articulation but functions as a shock absorber by increasing the surface area of joint contact. This absorption mechanism apparently works well because significant age-related degenerative arthritis is relatively rare at this joint.35
The tremendous stability at the SC joint is due to the arrangement of the periarticular connective tissues and, to a lesser extent, the interlocking of the articular surfaces. Large forces through the clavicle often cause fracture of the bone before the SC joint dislocates. Clavicular fractures are most common in males under 30 years old—most often as the result of contact-sport or road-traffic accidents.164
KINEMATICS
The osteokinematics of the clavicle involve a rotation in all three degrees of freedom. Each degree of freedom is associated with one of the three cardinal planes of motion: sagittal, frontal, and horizontal. The clavicle elevates and depresses, protracts and retracts, and rotates around the bone’s longitudinal axis (Figure 5-13). The primary purpose of these movements is to place the scapula in an optimal position to accept the head of the humerus. Essentially all functional movements of the glenohumeral joint involve some movement of the clavicle around the SC joint. As described later in this chapter, the clavicle rotates in all three degrees of freedom as the arm is raised overhead.110,115,125,169
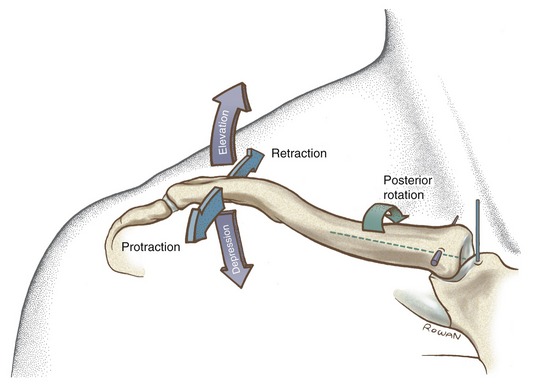
Elevation and Depression: Elevation and depression of the clavicle occur approximately parallel to the frontal plane, around a near anterior-posterior axis of rotation (see Figure 5-13). Maximums of approximately 45 degrees of elevation and 10 degrees of depression have been reported.27,140 Elevation and depression of the clavicle produce a similar path of movement of the scapula.73
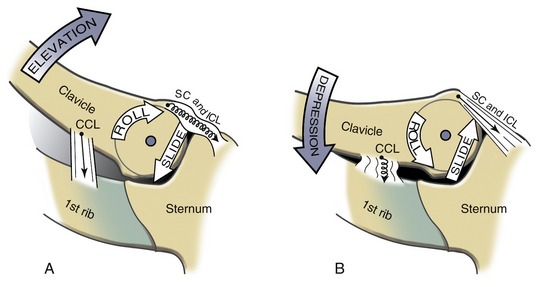
The arthrokinematics for elevation and depression of the clavicle occur along the SC joint’s longitudinal diameter (see Figure 5-12). Elevation of the clavicle occurs as its convex articular surface rolls superiorly and simultaneously slides inferiorly on the concavity of the sternum (Figure 5-14, A). The stretched costoclavicular ligament helps limit as well as stabilize the elevated position of the clavicle. Depression of the clavicle occurs by action of its convex surface rolling inferiorly and sliding superiorly (see Figure 5-14, B). A fully depressed clavicle elongates and stretches the interclavicular ligament and the superior portion of the capsular ligaments.
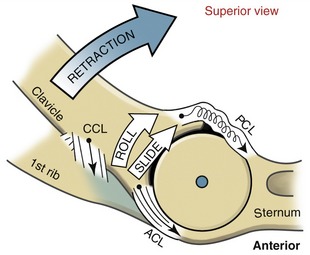
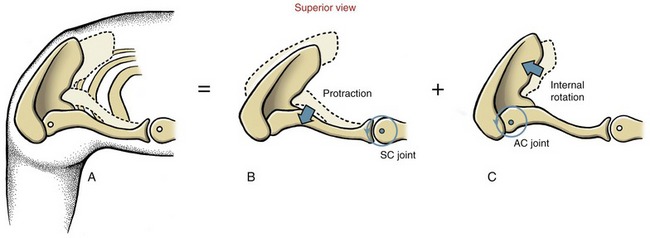
Protraction and Retraction: Protraction and retraction of the clavicle occur nearly parallel to the horizontal plane, around a vertical axis of rotation (see Figure 5-13). (The axis of rotation is shown in Figure 5-13 as intersecting the sternum because, by convention, the axis of rotation for a given motion intersects the convex member of the joint.) A maximum of 15 to 30 degrees of motion have been reported in each direction.27,140,179 The horizontal plane motions of the clavicle are strongly associated with protraction and retraction motions of the scapula.
The arthrokinematics for protraction and retraction of the clavicle occur along the SC joint’s transverse diameter (see Figure 5-12). Retraction occurs as the concave articular surface of the clavicle rolls and slides posteriorly on the convex surface of the sternum (Figure 5-15). The end ranges of retraction elongate the anterior bundles of the costoclavicular ligament and the anterior capsular ligaments.
Axial (Longitudinal) Rotation of the Clavicle: The third degree of freedom at the SC joint is a rotation of the clavicle around the bone’s longitudinal axis (see Figure 5-13). During shoulder abduction or flexion, a point on the superior aspect of the clavicle rotates posteriorly 20 to 35 degrees.62,84,115,194 As the arm is returned to the side, the clavicle rotates back to its original position. The arthrokinematics of clavicular rotation involve a spin of its sternal end relative to the lateral surface of the articular disc.
Acromioclavicular Joint
The acromioclavicular (AC) joint is the articulation between the lateral end of the clavicle and the acromion of the scapula (Figure 5-16, A). The clavicular facet on the acromion faces medially and slightly superiorly, providing a point of attachment with the corresponding acromial facet on the clavicle. An articular disc of varying form is present in most AC joints.
The AC joint is a gliding or plane joint, reflecting the predominantly flat contour of the joint surfaces. Joint surfaces vary, however, from flat to slightly convex or concave (see Figure 5-16, B). Because of the predominantly flat joint surfaces, roll-and-slide arthrokinematics are not described.
PERIARTICULAR CONNECTIVE TISSUE
The AC joint is surrounded by a capsule that is directly reinforced by superior and inferior ligaments (Figure 5-17).36,105 The superior capsular ligament is reinforced through attachments from the deltoid and trapezius.
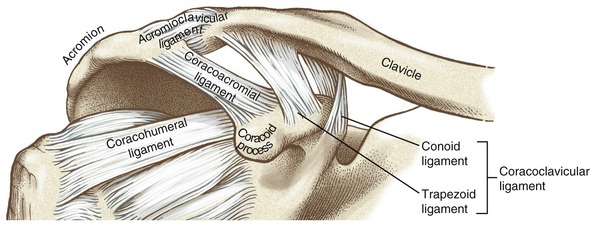
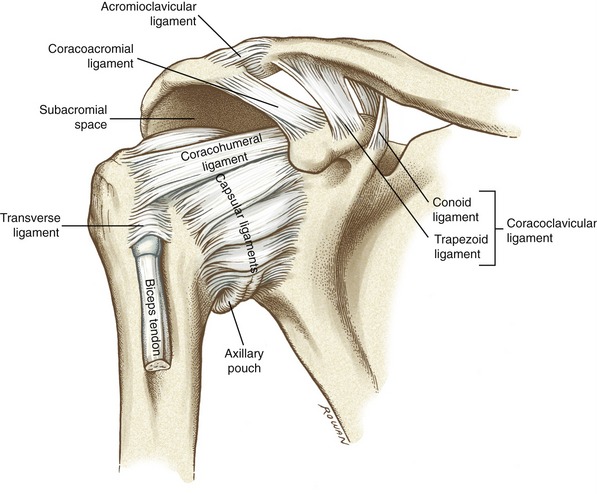
FIGURE 5-17. An anterior view of the right acromioclavicular joint including many surrounding ligaments.
The coracoclavicular ligament provides an important extrinsic source of stability to the AC joint (see Figure 5-17). This extensive ligament consists of two parts: the trapezoid and conoid ligaments. The trapezoid ligament extends in a superior-lateral direction from the superior surface of the coracoid process to the trapezoid line on the clavicle. The conoid ligament extends almost vertically from the proximal base of the coracoid process to the conoid tubercle on the clavicle.
Both parts of the coracoclavicular ligament are of similar length, cross-sectional area, stiffness, and tensile strength.31 As a whole, the entire ligament is stronger and absorbs more energy at the point of rupture than most other ligaments of the shoulder. These structural features, in conjunction with the coracoclavicular ligament’s near-vertical orientation, suggest an important role in suspending the scapula (and upper extremity) from the clavicle.
The articular surfaces at the AC joint are lined with a layer of fibrocartilage and often separated by a complete or incomplete articular disc. An extensive dissection of 223 sets of AC joints revealed complete discs in only about 10% of the joints.35 The majority of joints possessed incomplete discs, which appeared fragmented and worn. According to DePalma,35 the incomplete discs are not structural anomalies but rather indications of the degeneration that often affects this joint.
SPECIAL FOCUS 5-1  Acromioclavicular Joint Dislocation
Acromioclavicular Joint Dislocation
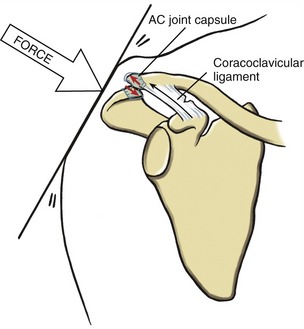
The acromioclavicular (AC) joint is inherently susceptible to dislocation (separation) because of the sloped nature of the articulation and the high probability of receiving large shearing forces. Consider a person falling and striking the tip of the shoulder abruptly against the ground (Figure 5-18). The resulting medially and inferiorly directed ground reaction force may displace the acromion medially and under the sloped articular facet of the well-stabilized clavicle. Such horizontal shear is resisted primarily by the joint’s superior and inferior capsular ligaments.36 The coracoclavicular ligament, however, offers a secondary resistance to horizontal shear, especially if severe.61 On occasion, the force applied to the scapula exceeds the tensile strength of all the ligaments, resulting in their rupture and complete dislocation of the AC joint. Trauma to the AC joint and associated ligaments can lead to instability and pain and possibly posttraumatic osteoarthritis. Extensive literature exists on the evaluation and the surgical and nonsurgical treatment of an injured AC joint, especially in athletes.22,30,59,121
KINEMATICS
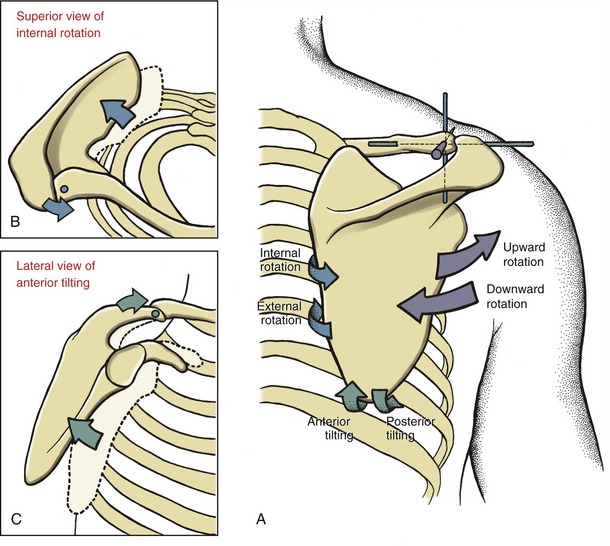
The motions of the AC joint are described by the movement of the scapula relative to the lateral end of the clavicle. Motion has been defined for 3 degrees of freedom (Figure 5-19, A). The primary, or most obvious, motions are called upward and downward rotation. Secondary motions—referred to as rotational adjustments—fine-tune the position of the scapula, in both the horizontal and sagittal planes. Measuring isolated motions at the AC joint is difficult and is not done in typical clinical situations.
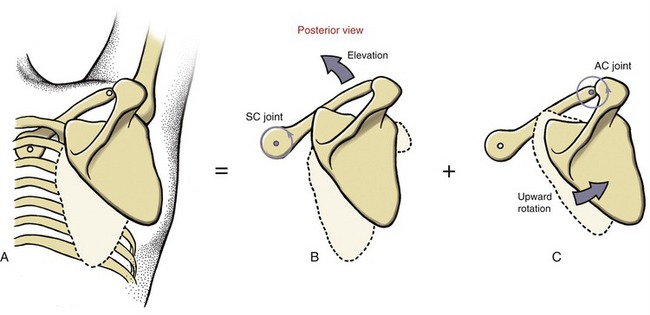
Upward and Downward Rotation: Upward rotation of the scapula at the AC joint occurs as the scapula “swings upwardly and outwardly” relative to the lateral end of the clavicle (see Figure 5-19, A). This motion occurs as a natural component of abduction or flexion of the shoulder. Reports vary widely, but up to 30 degrees of upward rotation at the AC joint occurs as the arm is raised fully over the head.84,115,185,194 The motion contributes a significant component of the overall upward rotation at the scapulothoracic joint. Downward rotation at the AC joint returns the scapula back toward the anatomic position, a motion mechanically associated with shoulder adduction or extension. Figure 5-19, A depicts the upward and downward rotation of the scapula as a frontal plane motion, although most natural motions occur within the scapular plane.
Horizontal and Sagittal Plane “Rotational Adjustments” at the Acromioclavicular Joint: Kinematic observations of the AC joint during shoulder movement reveal pivoting or twisting type motions of the scapula around the lateral end of the clavicle. These so-called “rotational adjustment motions” optimally align the scapula against the thorax, as well as adding to the total amount of its motion. Rotation adjustment motions at the AC joint are described within horizontal and sagittal planes (blue and green arrows in Figure 5-19, A, respectively).
Horizontal plane adjustments at the AC joint occur around a vertical axis, evident as the medial border of the scapula pivots away and toward the posterior surface of the thorax. These horizontal plane motions are described as internal and external rotation, defined by the direction of rotation of the glenoid fossa (see Figure 5-19, A). Sagittal plane adjustments at the AC joint occur around a near medial-lateral axis, evident as the inferior angle pivots away or toward the posterior surface of the thorax. The terms anterior tilting and posterior tilting describe the direction of this rotation, based on (as with horizontal plane motions) the direction of rotation of the glenoid fossa (see Figure 5-19).
The kinematics of the rotational adjustments at the AC joint are poorly understood, primarily because of the technical difficulties in isolating and measuring the relative small movements between the scapula and the clavicle. Moreover, the nomenclature used to describe these motions is not universally accepted. Differing magnitudes of motions have been reported during shoulder abduction or flexion, generally ranging from 5 to 30 degrees per plane.* Although the kinematics at the AC joint are not well defined, certainly it enhances both the quality and quantity of movement at the scapulothoracic joint. Qualitatively, for instance, during protraction of the scapulothoracic joint, the AC joint internally rotates slightly within the horizontal plane (see Figure 5-19, B). This rotation helps align the anterior surface of the scapula to the curved contour of the thorax. For similar reasons of alignment, the scapula is allowed to tilt anteriorly slightly during elevation of the scapulothoracic joint, as during “shrugging” of the shoulders (see Figure 5-19, C). Without these rotational adjustments, the scapula would be obligated to follow the exact path of the moving clavicle, without any freedom to fine-tune its position on the thorax.
Scapulothoracic Joint
The scapulothoracic joint is not a true joint per se but rather a point of contact between the anterior surface of the scapula and the posterior-lateral wall of the thorax.209 The two surfaces do not make direct contact; rather, they are separated by muscles, such as the subscapularis, serratus anterior, and erector spinae. The relatively thick and moist surfaces of these muscles likely reduce shear within the articulation during movement. An audible clicking sound during scapular movements may indicate abnormal contact within the articulation.
In the anatomic position, the scapula is usually positioned between the second and the seventh ribs, with the medial border located about 6 cm lateral to the spine. Although highly variable, the average “resting” posture of the scapula is about 10 degrees of anterior tilt, 5 to 10 degrees of upward rotation, and about 35 degrees of internal rotation—a position consistent with the previously described plane of the scapula.113,115
KINEMATICS
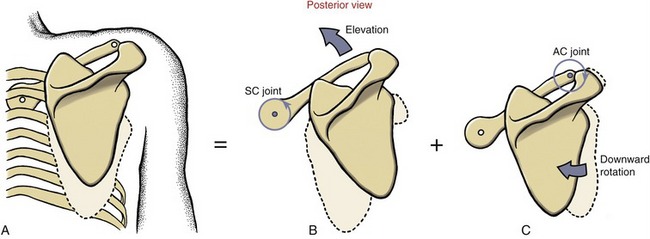
Elevation and Depression: Scapular elevation occurs as a composite of SC and AC joint rotations (Figure 5-20, A). For the most part, the motion of shrugging the shoulders is a direct result of the scapula following the path of the elevating clavicle around the SC joint (see Figure 5-20, B). Slight downward rotation of the scapula at the AC joint allows the scapula to remain nearly vertical throughout the elevation (see Figure 5-20, C). Additional adjustments at the AC joint help to keep the scapula flush with the slightly changing curvature of the thorax. Depression of the scapula occurs as the reverse action described for elevation.
Protraction and Retraction: Protraction of the scapula occurs through a summation of horizontal plane rotations at both the SC and AC joints (Figure 5-21, A). The scapula follows the general path of the protracting clavicle around the SC joint (see Figure 5-21, B). The AC joint can amplify, offset, or otherwise adjust the total amount of scapulothoracic protraction by contributing varying amounts of internal rotation (see Figure 5-21, C). Because scapulothoracic protraction occurs as a composite of motions at the SC and AC joints, a decrease in motion at one joint can be partially compensated for by an increase at the other. Consider, for example, an individual with severe degenerative arthritis and decreased motion at the AC joint. The SC joint may compensate by contributing a greater degree of protraction, thereby limiting the functional loss associated with forward reach of the upper limb.
Upward and Downward Rotation: Upward rotation of the scapulothoracic joint is an integral part of raising the arm overhead (Figure 5-22, A). This motion places the glenoid fossa in a position to support and stabilize the head of the abducted (i.e., raised) humerus. Complete upward rotation of the scapula occurs by a summation of clavicular elevation at the SC joint (see Figure 5-22, B) and scapular upward rotation at the AC joint (see Figure 5-22, C).62,84,110,115,169 These coupled rotations are essential to the full 60 degrees of upward rotation at the scapulothoracic joint.49 The scapula may rotate upwardly and strictly in the frontal plane as in true abduction but more often follows a path closer to its own “scapular” plane. Normally the AC and SC joints have the mobility to adjust to the virtually infinite number of paths that the scapula may take during elevation of the arm.
SPECIAL FOCUS 5-2  The Functional Importance of Full Upward Rotation of the Scapulothoracic Joint
The Functional Importance of Full Upward Rotation of the Scapulothoracic Joint
The ability to raise the arm fully overhead is a prerequisite for many functional activities. A fully upward rotated scapula is an important component of this movement, accounting for approximately one third of the near 180 degrees of shoulder abduction or flexion.5,84,123,134,194 As with all scapulothoracic motions, upward rotation is mechanically linked to the motions of the sternoclavicular and acromioclavicular joints.
The upward rotation of the scapula that occurs during full shoulder abduction in the plane of the scapula (about 35 degrees anterior to the frontal plane) serves at least three important functions. First, the upwardly rotated scapula projects the glenoid fossa upward and anterior-laterally, providing a structural base to maximize the upward and lateral reach of the upper limb. Second, the upwardly rotated scapula preserves the optimal length-tension relationship of the abductor muscles of the glenohumeral joint, such as the middle deltoid and supraspinatus. Third, the upwardly rotated scapula helps maintain the volume within the subacromial space: the area between the undersurface of the acromion and the humeral head (see Figures 5-24 and 5-25).135 A reduced subacromial space during abduction may lead to a painful and damaging impingement of the residing tissues, such as the supraspinatus tendon.116 Although more research is needed in this area, it is clear that the kinematics associated with upward rotation of the scapula are essential to optimal function of the shoulder, especially for full and pain-free range of abduction.
Glenohumeral Joint
The glenohumeral (GH) joint is the articulation formed between the large convex head of the humerus and the shallow concavity of the glenoid fossa (Figure 5-23). This joint operates in conjunction with the moving scapula to produce an extensive range of motion of the shoulder. In the anatomic position, the articular surface of the glenoid fossa is directed anterior-laterally in the scapular plane. In most people the glenoid fossa is upwardly rotated slightly: a position dependent on the amount of fixed upward inclination of the fossa and on the degree of upward rotation of the scapulothoracic joint.
In the anatomic position, the humeral head is directed medially and superiorly, as well as posteriorly because of its natural retroversion. This orientation places the head of the humerus directly into the scapular plane and therefore directly against the face of the glenoid fossa (see Figure 5-4, B and C).
PERIARTICULAR CONNECTIVE TISSUE AND OTHER SUPPORTING STRUCTURES
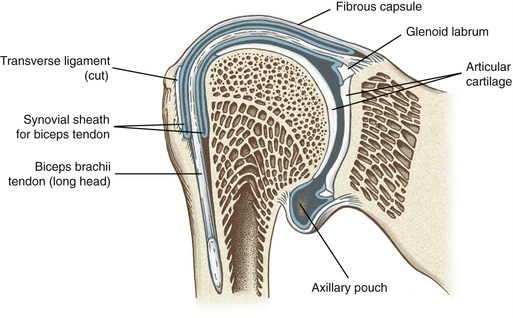
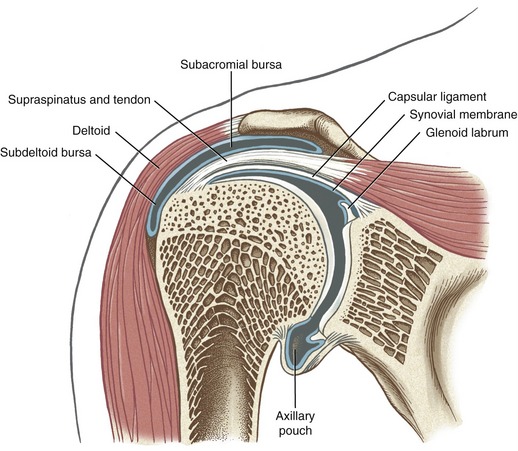
The GH joint is surrounded by a fibrous capsule that isolates the joint cavity from most surrounding tissues (see Figure 5-23). The capsule attaches along the rim of the glenoid fossa and extends to the anatomic neck of the humerus. A synovial membrane lines the inner wall of the joint capsule. An extension of this synovial membrane lines the intracapsular portion of the tendon of the long head of the biceps brachii. This synovial membrane continues to surround the biceps tendon as it exits the joint capsule and descends into the intertubercular (i.e., bicipital) groove. The head of the humerus and the glenoid fossa are both lined with articular cartilage.
SPECIAL FOCUS 5-3  The “Loose Fit” of the Glenohumeral Joint: an Inherent Problem of Instability
The “Loose Fit” of the Glenohumeral Joint: an Inherent Problem of Instability
Several anatomic features of the glenohumeral (GH) joint contribute to a design that favors mobility at the expense of stability. The articular surface of the glenoid fossa covers only about one third of the articular surface of the humeral head. This size difference allows only a small part of the humeral head to make contact with the glenoid fossa in any given shoulder position. In a typical adult, the longitudinal diameter of the humeral head is about 1.9 times larger than the longitudinal diameter of the glenoid fossa (Figure 5-24). The transverse diameter of the humeral head is about 2.3 times larger than the opposing transverse diameter of the glenoid fossa. The GH joint is often described as a ball-and-socket joint, although this description gives the erroneous impression that the head of the humerus fits into the glenoid fossa. The actual structure of the GH joint resembles more that of a golf ball pressed against a coin the size of a quarter. This bony fit offers little to no stability to the GH joint; instead, the mechanical integrity of the articulation is maintained primarily through mechanisms involving the surrounding muscles and capsular ligaments.
For a host of reasons, capsular ligaments may fail to adequately support and stabilize the GH joint. Such lack of support is manifested by excessive translation of the humeral head. Although some degree of laxity is normal at the GH joint, excessive laxity is not.201 A condition of excessive laxity, or “joint play,” associated with large translations of the proximal humerus relative to the glenoid is often referred to as shoulder instability. A diagnosis of shoulder instability typically means that the excessive laxity is associated with pain, apprehension, or a lack of function.76
Instability of the GH joint is often associated with less than optimal alignment and disrupted arthrokinematics, which over time can place damaging stress on the joint’s soft tissues. It is not always clear if shoulder instability is more the result or the cause of the abnormal arthrokinematics. The pathomechanics of shoulder instability are poorly understood and occupy the forefront of interest among clinicians, researchers, and surgeons.16,25,201
Capsular Ligaments: The external layers of the anterior and inferior walls of the joint capsule are thickened by fibrous connective tissue known simply as the glenohumeral capsular ligaments (Figure 5-25). Most of the fibers within the ligaments attach to the humerus, although a few more circular fibers spiral around the joint and reattach within the capsule.65 To generate stabilizing tensions across the joint, the inherently loose capsular ligaments must be elongated or twisted to varying degrees; the resulting passive tension generates mechanical support for the GH joint and limits the extremes of rotation and translation.
By reinforcing the walls of the capsule, the capsular ligaments also assist with maintaining a negative intra-articular pressure within the GH joint. This slight suction offers an additional source of stability.85 Puncturing (or venting) of the capsule equalizes the pressure on both sides, removing the slight suction force between the head and the fossa. Experimental release of the pressure by piercing the capsule with a needle has been shown to cause inferior subluxation of the humeral head.101
The following discussion describes the essential anatomy and functions of the GH joint capsular ligaments. Although a separate entity, the coracohumeral ligament will be considered with this group. The following material is essential for determining which ligament, or part of the capsule, is most responsible for restricting a particular movement. Such information assists the clinician and surgeon understand the mechanisms responsible for capsular injury and joint instability, and also provides guidance for manual therapy and surgical intervention38,88,139,202 Table 5-1 lists the distal attachments of the ligaments and specific motions that render each ligament taut. Considerably more detail exists on this subject and can be found in other sources.11,19,33,39,100,201
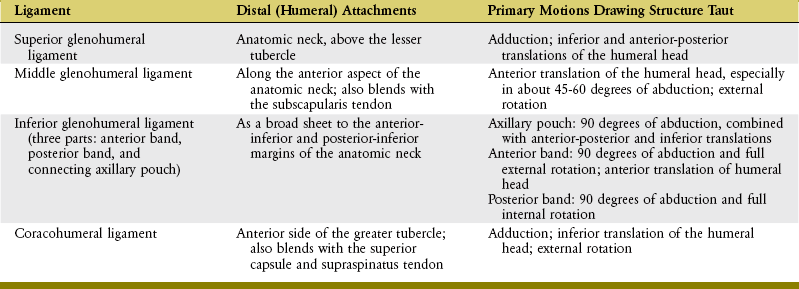
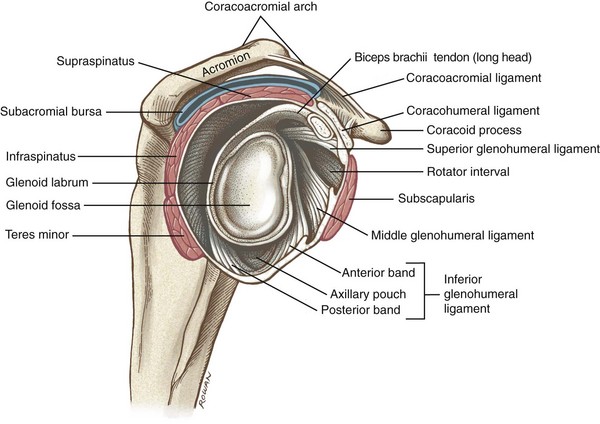
The GH joint’s capsular ligaments consist of complex bands of interlacing collagen fibers, divided into superior, middle, and inferior bands.65 The ligaments are best visualized from an internal view of the GH joint (Figure 5-26). The superior glenohumeral ligament has its proximal attachment near the supraglenoid tubercle, just anterior to the long head of the biceps. The ligament, with adjacent capsule, attaches near the anatomic neck of the humerus above the lesser tubercle. The ligament becomes particularly taut in full adduction. Once taut in adduction, the superior capsular ligament provides a restraint to inferior and anterior-posterior translations of the humeral head.37
The middle glenohumeral ligament has a wide proximal attachment to the superior and middle aspects of the anterior rim of the glenoid fossa. The ligament blends with the anterior capsule and broad tendon of the thick subscapularis muscle, then attaches along the anterior aspect of the anatomic neck. This ligament provides a substantial anterior restraint to the GH joint, especially in a position of 45 to 60 degrees of abduction.37,54 Based on its location, the middle glenohumeral ligament is very effective at limiting the extremes of external rotation.54,151
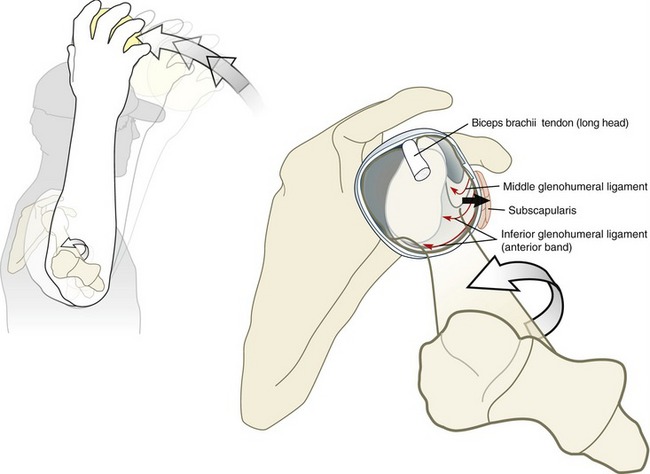
The extensive inferior glenohumeral ligament attaches proximally along the anterior-inferior rim of the glenoid fossa, including the glenoid labrum. Distally the inferior glenohumeral ligament attaches as a broad sheet to the anterior-inferior and posterior-inferior margins of the anatomic neck.128,129,182 The hammock-like inferior capsular ligament has three separate components: an anterior band, a posterior band, and a sheet of tissue connecting these bands known as an axillary pouch (see Figure 5-26).151 The axillary pouch and the surrounding inferior capsular ligaments become most taut in about 90 degrees of abduction. Acting as a sling, the taut axillary pouch supports the suspended humeral head and provides a cradling effect that resists inferior and anterior-posterior translations.176,188,204 From this abducted position, the anterior and posterior bands become further taut at the extremes of external and internal rotation, respectively.100,204 The anterior band—the strongest and thickest part of the entire capsule—is particularly important, as it furnishes the primary ligamentous restraint to anterior translation of the humeral head, both in an abducted and a neutral position.65,152 Forceful and dynamic activities involving abduction and external rotation specifically stress the anterior band of the inferior capsule. Such stress, for example, may occur during the “cocking phase” of throwing a baseball (Figure 5-27). Over many repetitions, this action can overstretch or tear the anterior band, thereby compromising one of the prime restraints to anterior translation of the humeral head.10,100 Injury and increased laxity of this portion of the anterior and inferior capsule are indeed associated with recurrent anterior dislocations of the GH joint.74,193 Whether the recurring anterior dislocation is caused by or results from tears or laxity in the anterior bands of the inferior capsule is not certain.138,201
The GH joint capsule is also strengthened by the coracohumeral ligament (see Figures 5-25 and 5-26). This ligament extends from the lateral border of the coracoid process to the anterior side of the greater tubercle of the humerus. The coracohumeral ligament also blends with the superior capsule and supraspinatus tendon. Similar to the superior capsular ligament, the position of adduction pulls the coracohumeral ligament taut. From this position, the coracohumeral ligament provides significant restraint to inferior translation and external rotation of the humeral head.13,86,100
Rotator Cuff Muscles and Long Head of the Biceps Brachii: As previously mentioned, the GH joint capsule receives significant structural reinforcement from the four rotator cuff muscles (see Figure 5-26). The subscapularis, the thickest of the four muscles,90 lies just anterior to the capsule. The supraspinatus, infraspinatus, and teres minor lie superior and posterior to the capsule. These four muscles form a cuff that protects and actively stabilizes the GH joint, especially during dynamic activities. In addition to the belly of the rotator cuff muscles being located very close to the joint, the tendons of these muscles actually blend into the capsule.178 This unique anatomic arrangement helps explain why the mechanical stability of the GH joint is so dependent on the innervation, strength, and control of the rotator cuff muscles. It is clinically important to note that, as evidenced by Figure 5-26, the rotator cuff fails to cover two regions of the capsule: inferiorly, and a region between the supraspinatus and subscapularis known as the rotator interval.83 The inherently weakened region of the rotator interval is, however, reinforced by the tendon of the long head of the biceps and the coracohumeral ligament.86 The rotator interval is one common site for anterior dislocation of the GH joint.
The long head of the biceps brachii originates off the supraglenoid tubercle of the scapula and adjacent rim of connective tissue known as the glenoid labrum (see Figure 5-26). From this proximal attachment, this intracapsular tendon crosses over the humeral head as it courses toward the intertubercular groove on the anterior humerus. Cadaver studies strongly suggest that in an active state, the long head of the biceps restricts anterior translation of the humeral head.100,154 In addition, the position of the tendon across the dome of the humeral head also suggests a role in resisting superior migration of the humeral head—an important force needed to control the natural arthrokinematics of abduction.154
Glenoid Labrum: The rim of the glenoid fossa is encircled by a fibrocartilage ring, or lip, known as the glenoid labrum (see Figure 5-26). About 50% of the overall depth of the glenoid fossa has been attributed to the glenoid labrum.79 By deepening the concavity of the fossa, the labrum increases contact area with the humeral head and therefore helps stabilize the joint.29
SPECIAL FOCUS 5-4  Why the Glenoid Labrum Is So Vulnerable to Injury
Why the Glenoid Labrum Is So Vulnerable to Injury
Several structural and functional factors explain why the glenoid labrum is so frequently involved in shoulder pathology. First, the superior part of the glenoid labrum is only loosely attached to the adjacent glenoid rim. Furthermore, approximately 50% of the fibers of the tendon of the long head of the biceps are direct extensions of the superior glenoid labrum; the remaining 50% arise from the supraglenoid tubercle.197 Exceedingly large or repetitive forces within the biceps tendon can partially detach the loosely secured superior labrum from its near–12 o’clock position on the glenoid rim. The relatively high incidence of superior labral tears in throwing athletes, such as baseball pitchers, is likely related to the forces produced within the biceps during this activity.100 The long head of the biceps is stressed (along with the anterior and inferior capsule) during the “cocking” phase of pitching, and again as the muscle rapidly decelerates the arm and forearm during the follow-through phase of the pitch.4,100 This stress is transferred directly to the superior labrum. A weakening of the proximal attachment of the long head of the biceps likely limits the muscle’s ability to restrain anterior translation of the humeral head.42 These pathomechanics may predispose the throwing athlete (or overhead laborer) to anterior instability and further associated stress.156 Several other mechanisms of injury and biomechanical consequences of lesions of the superior labrum have been postulated.144,145,208
Lesions or detachments of the glenoid labrum are also common along the anterior-inferior rim of the glenoid fossa.74,193 Normally this region of the labrum is firmly attached to the anterior band of the inferior capsular ligament.29 As previously described, excessive laxity or tears in this portion of the capsule can lead to recurrent anterior dislocations of the humeral head.170 A rapidly anteriorly translating humeral head can create damaging forces on the adjacent anterior-inferior capsule and glenoid labrum. The resulting frayed or partially torn labrum or adjacent capsule may create a vicious cycle of greater anterior GH joint instability and more frequent episodes of stress in this region. Conservative management of a detached or torn glenoid labrum is often unsuccessful, especially if the shoulder is also mechanically unstable. Surgical repair is often required, followed by a specific postoperative rehabilitation program.156,208
SCAPULOTHORACIC POSTURE AND ITS EFFECT ON STATIC STABILITY
Normally when one stands at complete rest with arms at the sides, the head of the humerus remains stable against the glenoid fossa. This stability is referred to as static because it exists at rest. One passive mechanism for controlling static stability at the GH joint is based on the analogy of a ball compressed against an inclined surface (Figure 5-28, A).9 At rest, the superior capsular structures (SCS) provide the primary ligamentous support for the humeral head. These structures include the superior capsular ligament, the coracohumeral ligament, and the tendon of the supraspinatus. Combining the resultant capsular force vector with the force vector due to gravity yields a compressive locking force, oriented at right angles to the surface of the glenoid fossa. The compression force (CF) stabilizes the GH joint by compressing the humeral head firmly against the glenoid fossa, thereby resisting descent of the humerus.86,87 The inclined plane of the glenoid also acts as a partial shelf that supports part of the weight of the arm.
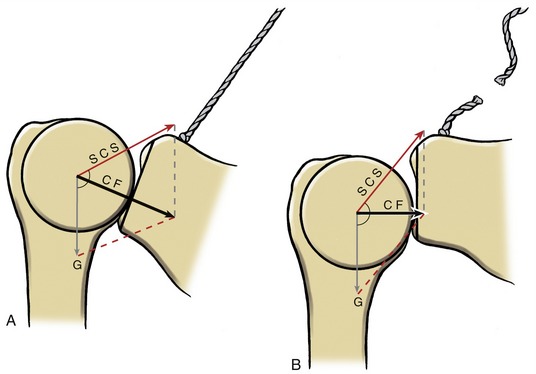
Electromyographic (EMG) data suggest that the supraspinatus, and to a lesser extent the posterior deltoid, provides a secondary source of static stability by generating active forces that are directed nearly parallel to the superior capsular force vector. This secondary support may be required, for example, while supporting a hand-held load by the side at the waist. Of interest, a classic and early study by Basmajian and Bazant9 showed that vertically running muscles, such as the biceps, triceps, and middle deltoid, are generally not actively involved in providing static stability, even when significant downward traction is applied to the arm.
An important component of the static locking mechanism is a scapulothoracic posture that maintains the glenoid fossa slightly upwardly rotated. A chronically downwardly rotated posture may be associated with “poor posture” or may be secondary to paralysis or weakness of certain muscles, such as the upper trapezius. Regardless of cause, loss of the upwardly rotated position increases the angle between the force vectors created by the superior capsular structures and gravity (see Figure 5-28, B). Adding the force vectors produced by the superior capsular structures and gravity now yields a reduced compressive force. Gravity can pull the humerus down the face of the glenoid fossa. Over time, and if not supported by external means, the downward pull can result in plastic deformation of the superior capsular structures. As a consequence, the inadequately supported head of the humerus may eventually sublux or dislocate inferiorly from the glenoid fossa.
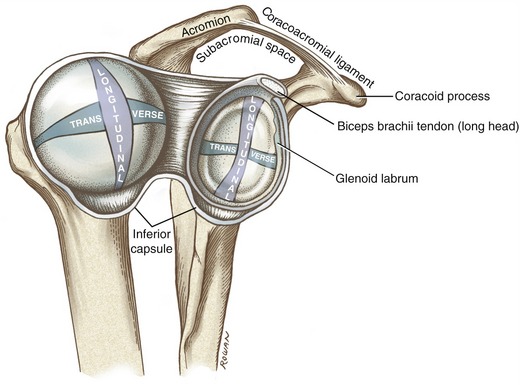
CORACOACROMIAL ARCH AND ASSOCIATED BURSA
The coracoacromial arch is formed by the coracoacromial ligament and the acromion process of the scapula (see Figure 5-26). The coracoacromial ligament attaches between the anterior margin of the acromion and the lateral border of the coracoid process.
The coracoacromial arch forms the functional “roof” of the GH joint. The space between the coracoacromial arch and the underlying humeral head was referred to earlier in the chapter as the subacromial space. In the healthy adult, the subacromial space measures only about 1 cm in height.157,189 The very clinically relevant subacromial space contains the supraspinatus muscle and tendon, the subacromial bursa, the long head of the biceps, and part of the superior capsule.
Multiple separate bursa sacs exist around the shoulder. Some of the sacs are direct extensions of the synovial membrane of the GH joint, such as the subscapular bursa, whereas others are separate structures. All are situated in regions where significant frictional forces develop, such as between tendons, capsule and bone, muscle and ligament, or two adjacent muscles. Two important bursa sacs are located superior to the humeral head (Figure 5-29). The subacromial bursa lies within the subacromial space above the supraspinatus muscle and below the acromion process. This bursa protects the relatively soft and vulnerable supraspinatus muscle and tendon from the rigid undersurface of the acromion. The subdeltoid bursa is a lateral extension of the subacromial bursa, limiting frictional forces between the deltoid and the underlying supraspinatus tendon and humeral head.
KINEMATICS
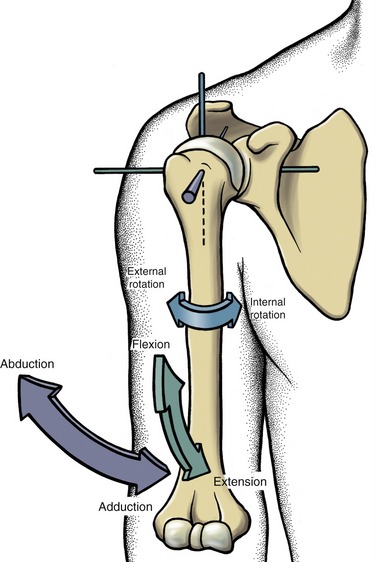
The GH joint is considered a universal joint because movement occurs in all three degrees of freedom. The primary motions at the GH joint are flexion and extension, abduction and adduction, and internal and external rotation (Figure 5-30). Often, a fourth motion is defined at the GH joint: horizontal flexion and extension (also called horizontal adduction and abduction). The motion occurs from a starting position of 90 degrees of abduction. The humerus moves anteriorly during horizontal flexion and posteriorly during horizontal extension.
Abduction and Adduction: Abduction and adduction are traditionally defined as rotation of the humerus in the near frontal plane around an axis oriented in the near anterior-posterior direction (Figure 5-30). Normally, the healthy person has about 120 degrees of abduction at the GH joint, although a range of values has been reported.5,84,115 External rotation of the GH joint naturally accompanies abduction—a point easily verifiable by palpation. This accompanying external rotation allows the greater tubercle of the humerus to pass posterior to the acromion process and therefore avoid jamming against the contents within the subacromial space, most notably the supraspinatus tendon. Full abduction of the shoulder complex requires a simultaneous approximate 60 degrees of upward rotation of the scapula; these kinematics were introduced previously in this chapter.
The arthrokinematics of abduction involve the convex head of the humerus rolling superiorly while simultaneously sliding inferiorly (see Figure 5-31). Roll-and-slide arthrokinematics occur along, or close to, the longitudinal diameter of the glenoid fossa (see Figure 5-24). With regard to arthrokinematics, adduction is similar to abduction but occurs in a reverse direction.
Figure 5-31 shows part of the supraspinatus muscle blending with the superior capsule of the GH joint. In addition to producing abduction, the active muscular contraction pulls the superior capsule taut, thereby protecting it from being pinched between the humeral head and undersurface of the acromion process. The muscular force also adds to the dynamic stability of the joint. (Dynamic stability refers to the stability achieved while the joint is moving.) As abduction proceeds, the prominent humeral head unfolds and stretches the axillary pouch of the inferior capsular ligament. The resulting tension within the inferior capsule acts as a hammock or sling, which supports the head of the humerus.
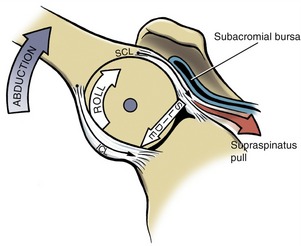
Importance of Roll-and-Slide Arthrokinematics at the Glenohumeral Joint: The roll-and-slide arthrokinematics depicted in Figure 5-31 are essential to the completion of full range abduction. Recall that the longitudinal diameter of the articular surface of the humeral head is almost twice the size of the longitudinal diameter on the glenoid fossa. The arthrokinematics of abduction demonstrate how a simultaneous roll and slide allow a larger convex surface to roll over a much smaller concave surface without running out of articular surface.
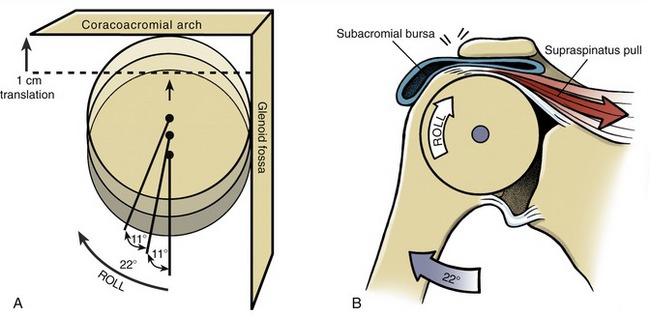
Without a sufficient concurrent inferior slide during abduction, the superior roll of the humeral head would ultimately lead to a jamming of the head against the unyielding coracoacromial arch. An adult-sized humeral head that is rolling up a glenoid fossa without a concurrent inferior slide would translate through the 10-mm subacromial space after only 22 degrees of GH joint abduction (Figure 5-32, A). This situation would create an impingement of the supraspinatus tendon and subacromial bursa between the head of the humerus and the coracoacromial arch.67 Such an impingement can physically block further abduction (see Figure 5-32, B). In vivo measurements of the healthy shoulder show that throughout abduction in the scapular plane, the center of the humeral head remains essentially stationary, or it may translate superiorly only a few millimeters.43,112,135,155,160 The concurrent inferior slide of the contact point of the humeral head offsets most of its inherent tendency to translate superiorly during abduction.
In healthy persons the offsetting effect of the roll-and-slide arthrokinematics in conjunction with a pliable inferior capsule contribute to the maintenance of a normal subacromial space during abduction. In cases of excessive stiffness and reduced volume of the axillary pouch, however, the humeral head is typically forced upward a considerable distance during abduction, and against the delicate tissues within the subacromial space. Such unnatural and repeated compression may damage and inflame the supraspinatus tendon, subacromial bursa, long head of the biceps tendon, and superior parts of the capsule. Over time, this repeated compression may lead to a painful condition known as subacromial impingement syndrome.135,147
SPECIAL FOCUS 5-6  Shoulder Abduction in the Frontal Plane versus the Scapular Plane
Shoulder Abduction in the Frontal Plane versus the Scapular Plane
Shoulder abduction in the frontal plane is often used as a representative motion to evaluate overall shoulder function. Despite its common usage, however, this motion is not very natural. Abducting the shoulder in the scapular plane (about 35 degrees anterior to the frontal plane) is a more natural movement and generally allows greater elevation of the humerus than abducting in the pure frontal plane.3 Furthermore, abducting in the scapular plane appears less mechanically coupled to an obligatory external rotation.181 This can be demonstrated by the following example. Attempt to maximally abduct your shoulder in the pure frontal plane while consciously avoiding any accompanying external rotation. The difficulty or inability to complete the extremes of this motion results in part from the greater tubercle of the humerus compressing the contents of the subacromial space against a low point on the coracoacromial arch (Figure 5-38, A).212 For natural completion of full frontal plane abduction, external rotation of the humerus must be combined with the abduction effort. This ensures that the prominent greater tubercle clears the posterior edge of the undersurface of the acromion.
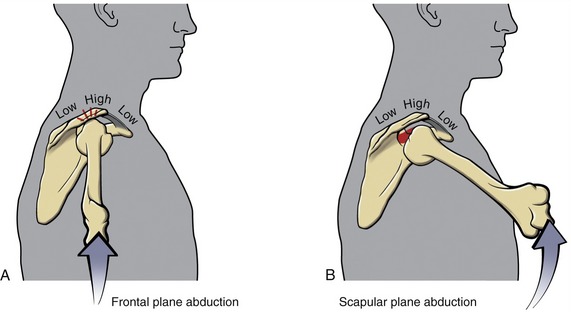
Next, fully abduct your arm in the scapular plane. This abduction movement can usually be performed with greater ease and with less external rotation, at least in the early to mid ranges of shoulder motion. Impingement is avoided because scapular plane abduction places the apex of the greater tubercle under the relatively high point of the coracoacromial arch (see Figure 5-38, B). Abduction in the scapular plane also allows the naturally retroverted humeral head to fit more directly into the glenoid fossa. The proximal and distal attachments of the supraspinatus muscle are placed along a straight line. These mechanical differences between frontal plane and scapular plane abduction should be considered during evaluation and treatment of patients with shoulder dysfunction, particularly if subacromial impingement is suspected.
Flexion and Extension: Flexion and extension at the GH joint are defined as a rotation of the humerus within the near sagittal plane around a near medial-lateral axis of rotation (Figure 5-33). The arthrokinematics involve primarily a spinning motion of the humeral head around the glenoid fossa. As shown in Figure 5-33, the spinning of the humeral head draws most of the surrounding capsular structures taut. Tension within the stretched posterior capsule may cause a slight anterior translation of the humerus at the extremes of flexion.75 At least 120 degrees of flexion are available to the GH joint. Flexing the shoulder to nearly 180 degrees includes an accompanying upward rotation of the scapulothoracic joint.115

Full extension of the shoulder occurs to a position of about 65 degrees actively (and 80 degrees passively) behind the frontal plane.8 The extremes of this passive motion likely stretch the capsular ligaments, causing a slight anterior tilting of the scapula. This forward tilt may enhance the extent of a backward reach.
Internal and External Rotation: From the anatomic position, internal and external rotation at the GH joint is defined as an axial rotation of the humerus in the horizontal plane (see Figure 5-30). This rotation occurs around a vertical or longitudinal axis that runs through the shaft of the humerus. The arthrokinematics of external rotation take place over the transverse diameters of the humeral head and the glenoid fossa (see Figure 5-24). The humeral head simultaneously rolls posteriorly and slides anteriorly on the glenoid fossa (Figure 5-34). The arthrokinematics for internal rotation are similar, except that the direction of the roll and slide is reversed.
The simultaneous roll and slide of internal and external rotation allows the much larger transverse diameter of the humeral head to roll over a much smaller surface area of the glenoid fossa. The importance of these anterior and posterior slides is evidenced by returning to the model of the humeral head shown in Figure 5-32, A, but envisioning the humeral head rolling over the glenoid fossa’s transverse diameter. If, for example, 75 degrees of external rotation occur by a posterior roll without a concurrent anterior slide, the head displaces posteriorly, roughly 38 mm. This amount of translation completely disarticulates the joint because the entire transverse diameter of the glenoid fossa is only about 25 mm (about 1 inch). Normally, however, full external rotation results in only 1 to 2 mm of posterior translation of the center of the humeral head, demonstrating that an “offsetting” anterior slide accompanies the posterior roll.75
As with all motions of the GH joint, the specific arthrokinematics depend on the exact plane of the osteokinematics. As previously described, from the anatomic position, internal and external rotation is associated with roll-and-slide arthrokinematics. Rotation of the GH joint from a position of about 90 degrees of abduction, however, requires primarily a spinning motion between a point on the humeral head and the glenoid fossa. Being able to visualize the relationship between the osteokinematics and arthrokinematics at a joint provides a useful mental construct for the treatment and evaluation of patients. These relationships are summarized in Table 5-2.
TABLE 5-2.
Summary of the Kinematic Relationships at the Glenohumeral Joint
| Osteokinematics | Plane of Motion/Axis of Rotation | Arthrokinematics |
| Abduction and adduction | Near frontal plane/near anterior-posterior axis of rotation | Roll and slide along joint’s longitudinal diameter |
| Internal and external rotation | Horizontal plane/vertical axis of rotation | Roll and slide along joint’s transverse diameter |
| Flexion and extension, internal and external rotation (in 90 degrees of abduction) | Near sagittal plane/near medial-lateral axis of rotation | Primarily a spin between humeral head and glenoid fossa |
SPECIAL FOCUS 5-5  “Dynamic Centralization” of the Humeral Head: an Important Interaction between the Capsule and the Rotator Cuff Muscles
“Dynamic Centralization” of the Humeral Head: an Important Interaction between the Capsule and the Rotator Cuff Muscles
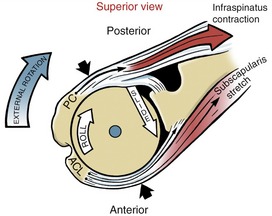
During all volitional motions at the glenohumeral (GH) joint, forces from activated rotator cuff muscles play a very important role in providing dynamic stability of the GH joint. Activated muscle forces combine with the passive forces from stretched capsular ligaments to maintain the humeral head in proper position on the glenoid fossa. Dynamic stability at the GH joint relies heavily on the interaction of these active and passive forces, particularly because of the natural incongruity and lack of bony containment of the joint. Figure 5-34 highlights an example of a dynamic stabilizing mechanism during active external rotation. The infraspinatus (one of the four rotator cuff muscles) is shown contracting to produce active external rotation torque at the GH joint. Because the infraspinatus attaches partially to the posterior capsule, its active contraction limits the amount of slack produced in this structure.88 Maintenance of even relatively low-level tension in the posterior capsule, combined with the natural rigidity from the activated muscle, helps stabilize the posterior side of the joint during active external rotation. In the healthy shoulder, the anterior side of the joint is also stabilized during active external rotation. Passive tension in the stretched subscapularis muscle, middle glenohumeral capsular ligament, and coracohumeral ligament all add rigidity to the anterior capsule. Forces therefore are generated on both sides of the joint during active external rotation, serving to stabilize and centralize the humeral head against the glenoid fossa.41
An excessively tight GH joint capsule may interfere with the effectiveness of the centralization process just described. For instance, during active external rotation (as shown in Figure 5-34), an overly tight anterior capsule could create a large, passive force that positions the humeral head too far posteriorly. This mechanism could decentralize the humeral head relative to the glenoid, creating abnormal contact areas within the joint. Alternatively (and likely more commonly), during active internal rotation an overly tight posterior capsule can displace the humeral head too far anteriorly. This situation is a possible factor associated with GH joint instability and subacromial impingement syndrome.111,122,192
Overall Kinematics of Shoulder Abduction: Establishing the Six Kinematic Principles of the Shoulder Complex
To this point, the study of shoulder arthrology has focused primarily on the isolated kinematics of the various joints, or links, within the shoulder complex. The next and final discussion summarizes the kinematics across the entire region, with a focus on how the bones or joints contribute to full active abduction. This discussion will highlight six kinematic principles related to full active shoulder abduction, shown in a highly mechanical fashion in Figure 5-35. When performed in a pain-free and natural manner, full abduction usually indicates optimal kinematic sequencing across the shoulder complex. Understanding how the joints of the complex work together allows the clinician to appreciate how impairments in one part of the complex affect another. This understanding serves as an important foundation for effective evaluation and treatment of the shoulder.
SCAPULOHUMERAL RHYTHM
The most widely cited study on the kinematics of shoulder abduction was published by Inman and colleagues in 1944.84 This classic work focused on shoulder abduction in the frontal plane. Data from this study were collected using two-dimensional radiographs and, most interesting, recording the movement of pins inserted directly into the bones of the shoulder in a live subject. This early study set the background for most subsequent studies on the kinematics of the shoulder.
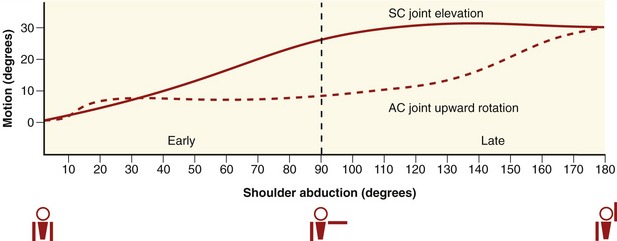
In the healthy shoulder a natural kinematic rhythm or timing exists between glenohumeral abduction and scapulothoracic upward rotation. Inman popularized the term “scapulohumeral rhythm” to explain this kinematic relationship. He reported that after about 30 degrees of abduction this rhythm remained remarkably constant, occurring at a ratio of 2 : 1: for every 3 degrees of shoulder abduction, 2 degrees occurs by GH joint abduction and 1 degree occurs by scapulothoracic joint upward rotation. The first kinematic principle of shoulder abduction states that based on a generalized 2 : 1 scapulohumeral rhythm, a full arc of nearly 180 degrees of abduction is the result of a simultaneous 120 degrees of GH joint abduction and 60 degrees of scapulothoracic upward rotation (see two purple arcs in main illustration of Figure 5-35).
A significant amount of research on scapulohumeral rhythm has been published since Inman’s classic in vivo work. Most of these studies used less invasive methods, including radiography, goniometry, photography, cinematography, and, more recently, fluoroscopy, magnetic resonance imaging, and electromechanical or electromagnetic tracking devices.* Published scapulohumeral rhythms vary across studies, ranging from 1.25 : 1 to 2.9 : 1, which are relatively close to Inman’s reported 2 : 1 ratio.† Variations in scapulohumeral rhythms reflect differences in measurement technique, population sampled, speed and arc of measured motion, number of dimensions recorded, and amount of external load. Regardless of the differing ratios reported in the literature, Inman’s classic 2 : 1 ratio remains a valuable axiom for evaluating shoulder abduction. It is simple to remember and helps to conceptualize the overall relationship between humeral and scapular movement considering the full 180 degrees of shoulder abduction.
STERNOCLAVICULAR AND ACROMIOCLAVICULAR JOINTS DURING FULL ABDUCTION
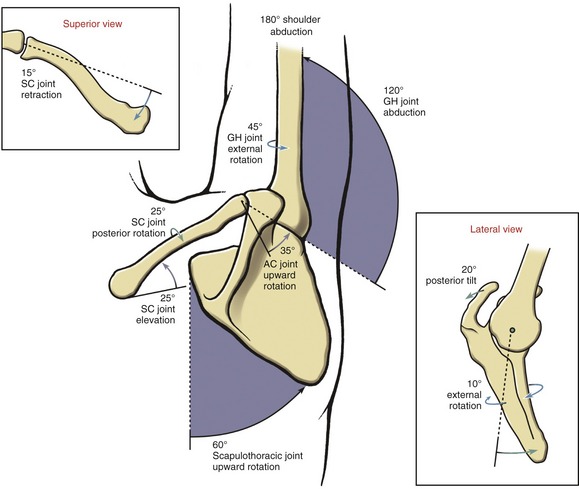
Upward rotation of the scapula during full abduction is one of the essential components of shoulder kinematics. What dictates the overall path of the scapula, however, are the combined kinematics at the SC and AC joints.84,115 These kinematics are plotted in Figure 5-36, based on data collected as a subject actively performed 180 degrees of frontal plane shoulder abduction. Although the preceding graph represents only one of many possible kinematic expressions at the SC and AC joints during abduction, it nicely introduces the next kinematic principle. The second kinematic principle of abduction states that the approximate 60 degrees of upward rotation of the scapula during full shoulder abduction are a result of a simultaneous elevation of the clavicle at the SC joint combined with upward rotation of the scapula at the AC joint. The precise angular motions that each joint contributes to scapular upward rotation are difficult to document with certainty. For mostly technical reasons, the kinematics at the SC joint have been more extensively studied in this regard. Inman reported that the SC joint elevates 30 degrees during 180 degrees of frontal plane abduction.84 In contrast, Ludewig and co-workers reported an average of only 6 to 10 degrees of clavicular elevation; however, their data were collected throughout a more limited arc of abduction.110,115 More definitive data are needed on the relative contributions of the SC and AC joints to upward rotation of the scapula, throughout a full range of shoulder abduction. It is clear, however, that each joint contributes significantly to the scapular motion, as depicted in the main illustration in Figure 5-35.
The third kinematic principle of abduction states that the clavicle retracts at the SC joint during full shoulder abduction. Recall that in the anatomic position the clavicle lies approximately horizontal, about 20 degrees posterior to the frontal plane (see Figure 5-4, A). During shoulder abduction the clavicle retracts about another 15 degrees (see Figure 5-35, top left inset). Of interest, these kinematics have been reported during active and passive abduction.62,123,125,194 The retracting clavicle assists the AC joint with optimal positioning of the scapula within the horizontal plane.110,115,174
The fourth kinematic principle of abduction states that during full abduction, the scapula posteriorly tilts and externally rotates (Figure 5-35, lower right inset). (Although these kinematic terms were described previously in Figure 5-19, A for the AC joint, they are frequently used in the literature to describe the overall motion of the scapula relative to the thorax.) The magnitude of the posterior tilting and external rotation of the scapula vary widely and are determined by the combined kinematics at the SC and AC joints.115,169,199 At rest in the anatomic position, the scapula is anteriorly tilted about 10 degrees and internally rotated approximately 35 degrees (i.e., in the scapular plane; see Figure 5-4, B). As shoulder abduction proceeds, the scapula posteriorly tilts primarily by motion at the AC joint. The external rotation of the scapula during full abduction, although relatively slight and variable, occurs as a net rotation based on movements at the SC and AC joints. According to Ludewig and colleagues, the AC joint actually internally rotates during shoulder abduction.115 Any potential internal rotation of the scapula is normally offset, however, by a greater magnitude of retraction at the SC joint. As a result, the scapula usually undergoes a slight net external rotation, although the bone is still biased anteriorly in the scapular plane. It is important to realize that the magnitude and pattern of these scapular motions vary considerably among studies.* Nevertheless, these motions are important and function to move the coracoacromial arch away from the advancing humeral head. Most studies suggest that the posterior tilting and net external rotation of the scapula help preserve the volume of the subacromial space during abduction.† These motions may limit the likelihood of impingement of structures in the subacromial space and thereby reduce mechanical stress on the shoulder capsule and rotator cuff muscles.116
The fifth kinematic principle of abduction states the clavicle rotates posteriorly around it own long axis. This motion was described earlier in this chapter as one of the primary SC joint motions (see Figure 5-13). Although actual measurements are scarce, the literature reports 20 to 35 degrees of clavicular rotation, depending on the plane and amount of shoulder abduction (see Figure 5-35, main illustration).84,110,115,194 Data consistently show that most of the rotation occurs relatively late in the range of abduction.
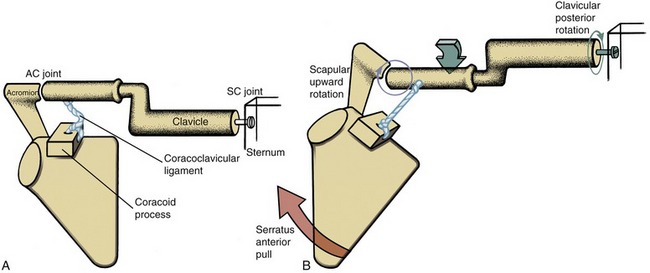
The mechanism that drives the posterior rotation of the clavicle is based on a combination of interesting multi-joint kinematics and forces transferred from muscle to ligaments. Figure 5-37, A shows in a very highly diagrammatic fashion the relatively slackened coracoclavicular ligament while at rest in the anatomic position. At the early phases of shoulder abduction, the scapula begins to upwardly rotate at the AC joint, stretching the relatively stiff coracoclavicular ligament (see Figure 5-37, B). The inability of this ligament to significantly elongate restricts further upward rotation at this joint. Tension within the stretched ligament is transferred to the conoid tubercle region of the clavicle, a point posterior to the bone’s longitudinal axis. The application of this force rotates the crank-shaped clavicle posteriorly. This rotation places the clavicular attachment of the coracoclavicular ligament closer to the coracoid process, unloading the ligament slightly and permitting the scapula to continue its final degrees of upward rotation. Inman84 describes this mechanism as “a fundamental feature of shoulder motion,” and without this motion complete shoulder abduction is not possible. Ludewig and colleagues report that posterior rotation of the clavicle is mechanically coupled with posterior tilting of the AC joint—motions that are essential to full-range shoulder abduction.110
The sixth kinematic principle of abduction states the humerus naturally externally rotates during shoulder abduction (see Figure 5-35, main illustration).115 As stated earlier, external rotation allows the greater tubercle to pass posterior to the acromion, avoiding a potential impingement of the contents in the subacromial space. Stokdijk and colleagues have shown differing ratios of external rotation to humeral elevation based on the specific plane of elevation.181 Pure frontal plane abduction had a higher ratio (i.e., greater external rotation per degree of abduction) than abduction in the scapular plane. The amount of external rotation that accompanies full active shoulder abduction is not known for certain but likely falls within the 25- to 55-degree range.
The six kinematic principles associated with the fully abducting shoulder are summarized in Box 5-1. These principles should provide a generalized guideline for organizing and highlighting the kinematics across the multiple joints of the shoulder. The actual magnitudes and pattern of motion associated with each principle will certainly vary for any individual person or study. This variability reflects the natural variability associated with human motion, and that caused by different methods of studying the topic.187
[/level-membership-for-rheumatology-category][not-level-membership-for-rheumatology-category]Chapter 5
Shoulder Complex
Periarticular Connective Tissue and Other Supporting Structures
Scapulothoracic Posture and its Effect on Static Stability
Overall Kinematics of Shoulder Abduction: Establishing the Six Kinematic Principles of the Shoulder Complex
Innervation of the Muscles and Joints of the Shoulder Complex
Action of the Shoulder Muscles
Muscles of the Scapulothoracic Joint
Muscles That Elevate the Arm at the Glenohumeral Joint
Upward Rotators at the Scapulothoracic Joint
Function of the Rotator Cuff Muscles during Elevation of the Arm
The study of the upper extremity begins with the shoulder complex, a set of four articulations involving the sternum, clavicle, ribs, scapula, and humerus (Figure 5-1). This series of joints provides extensive range of motion to the upper extremity, thereby increasing the ability to reach and manipulate objects. Trauma or disease often limits shoulder motion, causing a significant reduction in the effectiveness of the entire upper limb.
FIGURE 5-1. The joints of the right shoulder complex.
OSTEOLOGY
The sternum consists of the manubrium, body, and xiphoid process (Figure 5-2). The manubrium possesses a pair of oval-shaped clavicular facets, which articulate with the clavicles. The costal facets, located on the lateral edge of the manubrium, provide bilateral attachment sites for the first two ribs. The jugular notch is located at the superior aspect of the manubrium, between the clavicular facets.
Clavicle
When one looks from above, it is evident that the shaft of the clavicle is curved, with its anterior surface being generally convex medially and concave laterally (Figure 5-3). With the arm in the anatomic position, the long axis of the clavicle is oriented slightly above the horizontal plane and about 20 degrees posterior to the frontal plane (Figure 5-4; angle A). The rounded and prominent medial or sternal end of the clavicle articulates with the sternum (see Figure 5-3). The costal facet of the clavicle (see Figure 5-3; inferior surface) rests against the first rib. Lateral and slightly posterior to the costal facet is the distinct costal tuberosity, an attachment for the costoclavicular ligament.
The lateral or acromial end of the clavicle articulates with the scapula at the oval-shaped acromial facet (see Figure 5-3; inferior surface). The inferior surface of the lateral end of the clavicle is well marked by the conoid tubercle and the trapezoid line.
Scapula
The triangular-shaped scapula has three angles: inferior, superior, and lateral (Figure 5-5). Palpation of the inferior angle provides a convenient method for following the movement of the scapula during arm motion. The scapula also has three borders. With the arm resting by the side, the medial or vertebral border runs almost parallel to the spinal column. The lateral or axillary border runs from the inferior angle to the lateral angle of the scapula. The superior border extends from the superior angle laterally toward the coracoid process.
The posterior surface of the scapula is separated into a supraspinatous fossa and an infraspinatous fossa by the prominent spine. The depth of the supraspinatous fossa is filled by the supraspinatus muscle. The medial end of the spine diminishes in height at the root of the spine. In contrast, the lateral end of the spine gains considerable height and flattens into the broad and prominent acromion (from the Greek akros, meaning topmost, highest). The acromion extends in a lateral and anterior direction, forming a horizontal shelf over the glenoid fossa. The clavicular facet on the acromion forms part of the acromioclavicular joint (see Figure 5-16, B).
The scapula articulates with the head of the humerus at the slightly concave glenoid fossa (from the Greek root glene, socket of joint, + eidos, resembling) (see Figure 5-5, B). The slope of the glenoid fossa is inclined upward about 4 degrees relative to a horizontal axis through the body of the scapula.26 This inclination is highly variable, ranging from a downward inclination of 7 degrees to an upward inclination of nearly 16 degrees. At rest the scapula is normally positioned against the posterior-lateral surface of the thorax, with the glenoid fossa facing about 35 degrees anterior to the frontal plane (see Figure 5-4; angle B). This orientation of the scapula is referred to as the scapular plane. The scapula and humerus tend to follow this plane when the arm is naturally raised overhead.
Located at the superior and inferior rim of the glenoid fossa are the supraglenoid and infraglenoid tubercles. These tubercles serve as the proximal attachment for the long head of the biceps and triceps brachii, respectively (see Figure 5-5, B). Near the superior rim of the glenoid fossa is the prominent coracoid process, meaning “the shape of a crow’s beak.” The coracoid process projects sharply from the scapula, providing multiple attachments for ligaments and muscles (Figure 5-6). The subscapular fossa is located on the anterior surface of the scapula (see Figure 5-5, B). The concavity within the fossa is filled with the thick subscapularis muscle.
Proximal-to-Mid Humerus
The head of the humerus, nearly one half of a full sphere, forms the convex component of the glenohumeral joint (Figure 5-7). The head faces medially and superiorly, forming an approximate 135-degree angle of inclination with the long axis of the humeral shaft (Figure 5-8, A). Relative to a medial-lateral axis through the elbow, the humeral head is rotated posteriorly about 30 degrees within the horizontal plane (see Figure 5-8, B). This rotation, known as retroversion (from the Latin retro, backward, + verto, to turn) aligns the humeral head within the scapular plane for articulation with the glenoid fossa (see Figure 5-4; angle C). Interestingly, researchers have shown that the dominant shoulder in elite baseball pitchers possesses greater humeral retroversion than the nondominant limb.24 This difference (which was not present in a control group of nonpitchers) was theorized to occur as an osseous adaptation to the large torsional stress generated during pitching.
The anatomic neck of the humerus separates the smooth articular surface of the head from the proximal shaft (see Figure 5-7, A). The prominent lesser and greater tubercles surround the anterior and lateral circumference of the extreme proximal end of the humerus (see Figure 5-7, B). The lesser tubercle projects rather sharply and anteriorly for attachment of the subscapularis. The large and rounded greater tubercle has an upper, middle, and lower facet, marking the distal attachment of the supraspinatus, infraspinatus, and teres minor, respectively (see Figure 5-7, B and Figure 5-9).
Sharp crests extend distally from the anterior side of the greater and lesser tubercles. These crests receive the distal attachments of the pectoralis major and teres major (see Figure 5-7, A). Between these crests is the intertubercular (bicipital) groove, which houses the tendon of the long head of the biceps brachii. The latissimus dorsi muscle attaches to the floor of the intertubercular groove, medial to the biceps tendon. Distal and lateral to the termination of the intertubercular groove is the deltoid tuberosity.
The radial (spiral) groove runs obliquely across the posterior surface of the humerus. The groove separates the proximal attachments of the lateral and medial head of the triceps (see Figure 5-9). Traveling distally, the radial nerve spirals around the posterior side of the humerus in the radial groove, heading toward the distal-lateral side of the humerus.
ARTHROLOGY
The most proximal articulation within the shoulder complex is the sternoclavicular joint (see Figure 5-1). The clavicle, through its attachment to the sternum, functions as a mechanical strut, or prop, holding the scapula at a relatively constant distance from the trunk. Located at the lateral end of the clavicle is the acromioclavicular joint. This joint, and associated ligaments, firmly attaches the scapula to the clavicle. The anterior surface of the scapula rests against the posterior-lateral surface of the thorax, forming the scapulothoracic joint. This articulation is not a true anatomic joint; rather, it is an interface between bones. Movements at the scapulothoracic joint are mechanically linked to the movements at both the sternoclavicular and acromioclavicular joints. The position of the scapula on the thorax provides a base of operation for the glenohumeral joint, the most distal and mobile link of the complex. The term “shoulder movement” describes the combined motions at both the glenohumeral and the scapulothoracic joints.
Before the kinematics of the sternoclavicular and acromioclavicular joints are described, the movements at the scapulothoracic joint must be defined (Figure 5-10). Primary movements at the scapulothoracic joint are traditionally described as elevation and depression, protraction and retraction, and upward and downward rotation. Additional movements of the scapula will be defined as the chapter unfolds.
Sternoclavicular Joint
The sternoclavicular (SC) joint is a complex articulation, involving the medial end of the clavicle, the clavicular facet on the sternum, and the superior border of the cartilage of the first rib (Figure 5-11). The SC joint functions as the basilar joint of the entire upper extremity, linking the appendicular skeleton with the axial skeleton. The joint therefore must be firmly attached while simultaneously allowing considerable range of movement. These seemingly paradoxic functions are accomplished through extensive periarticular connective tissues, and an irregular saddle-shaped articular surface (Figure 5-12). Although highly variable, the medial end of the clavicle is usually convex along its longitudinal diameter and concave along its transverse diameter.178 The clavicular facet on the sternum typically is reciprocally shaped, with a slightly concave longitudinal diameter and a slightly convex transverse diameter.
PERIARTICULAR CONNECTIVE TISSUE
The SC joint is enclosed by a capsule reinforced by anterior and posterior sternoclavicular ligaments (see Figure 5-11).177 When active, muscles add further stability to the joint: anteriorly by the sternocleidomastoid, posteriorly by the sternothyroid and sternohyoid, and inferiorly by the subclavius. The interclavicular ligament spans the jugular notch, connecting the medial end of the right and left clavicles.
The costoclavicular ligament is a strong structure extending from the cartilage of the first rib to the costal tuberosity on the inferior surface of the clavicle. The ligament has two distinct fiber bundles running perpendicular to each other.178 The anterior bundle runs obliquely in a superior and lateral direction, and the posterior bundle runs obliquely in a superior and medial direction (see Figure 5-11). The crisscrossing of fibers assists with stabilizing the joint through all motions, except for a downward movement of the clavicle (i.e., depression).
The articular disc at the SC joint separates the joint into distinct medial and lateral joint cavities (see Figure 5-11).178 The disc is a flattened piece of fibrocartilage that attaches inferiorly near the lateral edge of the clavicular facet and superiorly at the sternal end of the clavicle and interclavicular ligament. The remaining outer edge of the disc attaches to the internal surface of the capsule. The disc not only strengthens the articulation but functions as a shock absorber by increasing the surface area of joint contact. This absorption mechanism apparently works well because significant age-related degenerative arthritis is relatively rare at this joint.35
The tremendous stability at the SC joint is due to the arrangement of the periarticular connective tissues and, to a lesser extent, the interlocking of the articular surfaces. Large forces through the clavicle often cause fracture of the bone before the SC joint dislocates. Clavicular fractures are most common in males under 30 years old—most often as the result of contact-sport or road-traffic accidents.164
KINEMATICS
The osteokinematics of the clavicle involve a rotation in all three degrees of freedom. Each degree of freedom is associated with one of the three cardinal planes of motion: sagittal, frontal, and horizontal. The clavicle elevates and depresses, protracts and retracts, and rotates around the bone’s longitudinal axis (Figure 5-13). The primary purpose of these movements is to place the scapula in an optimal position to accept the head of the humerus. Essentially all functional movements of the glenohumeral joint involve some movement of the clavicle around the SC joint. As described later in this chapter, the clavicle rotates in all three degrees of freedom as the arm is raised overhead.110,115,125,169
Elevation and Depression: Elevation and depression of the clavicle occur approximately parallel to the frontal plane, around a near anterior-posterior axis of rotation (see Figure 5-13). Maximums of approximately 45 degrees of elevation and 10 degrees of depression have been reported.27,140 Elevation and depression of the clavicle produce a similar path of movement of the scapula.73
The arthrokinematics for elevation and depression of the clavicle occur along the SC joint’s longitudinal diameter (see Figure 5-12). Elevation of the clavicle occurs as its convex articular surface rolls superiorly and simultaneously slides inferiorly on the concavity of the sternum (Figure 5-14, A). The stretched costoclavicular ligament helps limit as well as stabilize the elevated position of the clavicle. Depression of the clavicle occurs by action of its convex surface rolling inferiorly and sliding superiorly (see Figure 5-14, B). A fully depressed clavicle elongates and stretches the interclavicular ligament and the superior portion of the capsular ligaments.
Protraction and Retraction: Protraction and retraction of the clavicle occur nearly parallel to the horizontal plane, around a vertical axis of rotation (see Figure 5-13). (The axis of rotation is shown in Figure 5-13 as intersecting the sternum because, by convention, the axis of rotation for a given motion intersects the convex member of the joint.) A maximum of 15 to 30 degrees of motion have been reported in each direction.27,140,179 The horizontal plane motions of the clavicle are strongly associated with protraction and retraction motions of the scapula.
The arthrokinematics for protraction and retraction of the clavicle occur along the SC joint’s transverse diameter (see Figure 5-12). Retraction occurs as the concave articular surface of the clavicle rolls and slides posteriorly on the convex surface of the sternum (Figure 5-15). The end ranges of retraction elongate the anterior bundles of the costoclavicular ligament and the anterior capsular ligaments.
Axial (Longitudinal) Rotation of the Clavicle: The third degree of freedom at the SC joint is a rotation of the clavicle around the bone’s longitudinal axis (see Figure 5-13). During shoulder abduction or flexion, a point on the superior aspect of the clavicle rotates posteriorly 20 to 35 degrees.62,84,115,194 As the arm is returned to the side, the clavicle rotates back to its original position. The arthrokinematics of clavicular rotation involve a spin of its sternal end relative to the lateral surface of the articular disc.
Acromioclavicular Joint
The acromioclavicular (AC) joint is the articulation between the lateral end of the clavicle and the acromion of the scapula (Figure 5-16, A). The clavicular facet on the acromion faces medially and slightly superiorly, providing a point of attachment with the corresponding acromial facet on the clavicle. An articular disc of varying form is present in most AC joints.
The AC joint is a gliding or plane joint, reflecting the predominantly flat contour of the joint surfaces. Joint surfaces vary, however, from flat to slightly convex or concave (see Figure 5-16, B). Because of the predominantly flat joint surfaces, roll-and-slide arthrokinematics are not described.
PERIARTICULAR CONNECTIVE TISSUE
The AC joint is surrounded by a capsule that is directly reinforced by superior and inferior ligaments (Figure 5-17).36,105 The superior capsular ligament is reinforced through attachments from the deltoid and trapezius.
FIGURE 5-17. An anterior view of the right acromioclavicular joint including many surrounding ligaments.
The coracoclavicular ligament provides an important extrinsic source of stability to the AC joint (see Figure 5-17). This extensive ligament consists of two parts: the trapezoid and conoid ligaments. The trapezoid ligament extends in a superior-lateral direction from the superior surface of the coracoid process to the trapezoid line on the clavicle. The conoid ligament extends almost vertically from the proximal base of the coracoid process to the conoid tubercle on the clavicle.
Both parts of the coracoclavicular ligament are of similar length, cross-sectional area, stiffness, and tensile strength.31 As a whole, the entire ligament is stronger and absorbs more energy at the point of rupture than most other ligaments of the shoulder. These structural features, in conjunction with the coracoclavicular ligament’s near-vertical orientation, suggest an important role in suspending the scapula (and upper extremity) from the clavicle.
The articular surfaces at the AC joint are lined with a layer of fibrocartilage and often separated by a complete or incomplete articular disc. An extensive dissection of 223 sets of AC joints revealed complete discs in only about 10% of the joints.35 The majority of joints possessed incomplete discs, which appeared fragmented and worn. According to DePalma,35 the incomplete discs are not structural anomalies but rather indications of the degeneration that often affects this joint.
