[level-membership-for-dermatology-category]30
Rosacea and Periorificial Dermatitis
Epidemiology
Clinical Features
• Highly variable degree of severity, from a few papulopustules to extreme distortion of the nose.
• Table 30.1 lists the four major types of rosacea (Figs. 30.1–30.5) and their characteristics.
Table 30.1
Four major types of rosacea.
An individual patient may have more than one form. Some patients also have seborrheic dermatitis and/or actinic damage.
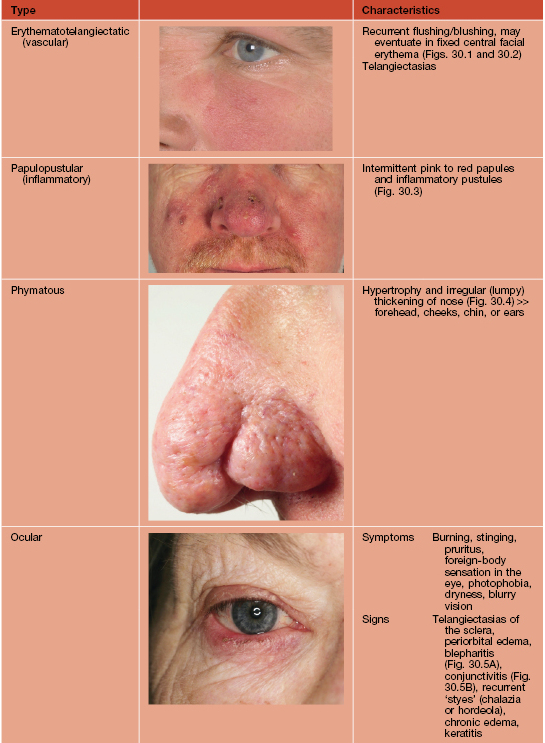

Fig. 30.1 Erythematotelangiectatic rosacea. Persistent erythema of the medial and lateral cheeks is seen. In this patient, there are no telangiectasias, indicating mild disease. Courtesy, Frank C. Powell, MD.

Fig. 30.2 Dermatoheliosis in a skin phototype I patient. Telangiectasias and erythema due to chronic actinic damage are particularly marked on the facial prominences. Features of dermatoheliosis overlap with those of erythematotelangiectatic rosacea. Courtesy, Frank C. Powell, MD.


Fig. 30.3 Rosacea. A Moderate papulopustular rosacea of the forehead. Note the superficial nature of the inflammatory lesions. B Moderate to severe papulopustular rosacea. There is a typical centrofacial distribution of erythema, telangiectasias, papules, and pustules. In addition, the skin has a scaly, crusty surface, and this is often a sign of more severe disease. Courtesy, Frank C. Powell, MD.


Fig. 30.4 Rhinophyma – early versus advanced disease. A Tortuous, telangiectatic vessels on the distal aspect of the nose contribute to its hyperemic appearance; this hyperemia may predispose to the subsequent hypertrophic changes of rhinophyma. Note the early sign of dilated follicles. B Distortion of nasal tissue due to tissue hypertrophy. Electrosurgery or laser therapy can be used to debulk and resculpt this nose. Courtesy, Frank C. Powell, MD.
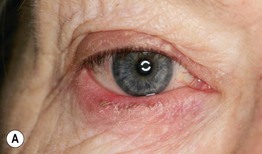

Fig. 30.5 Ocular rosacea. A Tiny concretions of keratin (conical dandruff) are visible at the bases of some of the eyelashes of the lower eyelid. There is also evidence of blepharitis predominantly of the eyelid margin and conjunctival injection. B Marked injection of the conjunctivae, leading to the appearance of red eyes. Ectropion is also present. A, Courtesy, Frank C. Powell, MD.
• Variants include granulomatous rosacea and periorificial dermatitis.
• Red to red-brown papules secondary to granulomatous inflammation (Fig. 30.6).

Fig. 30.6 Granulomatous rosacea. Discrete skin-colored to brown papules scattered on the face. Courtesy, Frank C. Powell, MD.
• Affects children and adults.
• Lesions around the mouth and nose > eyes.
• Monomorphic pink papules and fine pustules (Figs. 30.7 and 30.8) admixed with eczematous patches and thin plaques, sometimes with fine scale.

Fig. 30.7 Periorificial dermatitis. Discrete dull pink-red papules around the mouth and nose. While periorificial dermatitis is often misdiagnosed as eczema, this more granulomatous form may be misdiagnosed as sarcoidosis if a biopsy has been performed. Courtesy, Julie V. Schaffer, MD.


Fig. 30.8 Periorificial dermatitis. A Granulomatous periorificial dermatitis in a child with monomorphous pink papules that have become confluent around the mouth. The eruption, which had previously worsened upon treatment with topical and oral corticosteroids, resolved with a 6-week course of azithromycin. B Periocular dermatitis with multiple fine papules and pustules superimposed on a pink plaque. The lesions can be misdiagnosed as an irritant or allergic contact dermatitis or atopic dermatitis. Although topical CS will initially improve the lesions, ultimately, there is exacerbation. A, Courtesy, Julie V. Schaffer, MD; B, Courtesy, Ronald P. Rapini, MD.
• Lesions recur over weeks to months.
• Erythematous, firm, nonpitting, painless swelling of the mid-face (Fig. 30.9).

Fig. 30.9 Facial edema secondary to rosacea (Morbihan’s disease). Erythematous, firm, nonpitting, nonpainful swelling of the upper face. Areas of greatest involvement have acquired a ‘peau d’orange’ appearance. Courtesy, Frank C. Powell, MD.
• Acute facial plaque studded with pustules.
• DDx: Table 30.2.
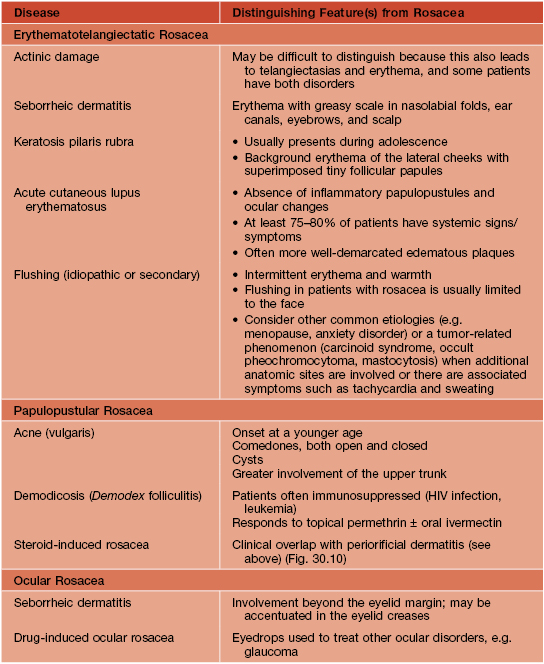

Fig. 30.10 Steroid rosacea. Mild disease in an adult with scattered erythematous papules and papulopustules. Courtesy, Kalman Watsky, MD.
• Rx: Tables 30.3 and 30.4.
Table 30.3
Medical and surgical therapies for rosacea and periorificial dermatitis.
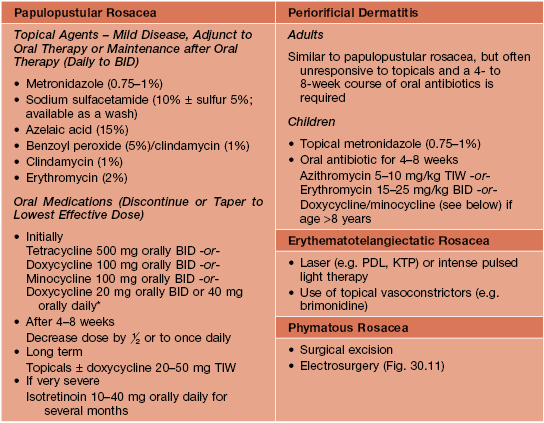
* Sub-antimicrobial dose.
BID, twice a day; KTP, potassium titanyl phosphate laser; PDL, pulsed dye laser; TIW, three times per week.
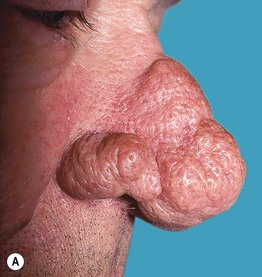
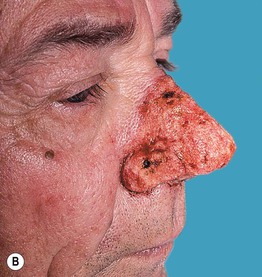
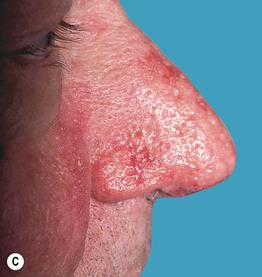
Fig. 30.11 Rhinophyma. A Moderately severe rhinophyma in a middle-aged man. B Immediately after electrosurgical planing of excess sebaceous glands. Care is taken to perform subtotal removal as very aggressive therapy can result in significant scarring and possible deformity caused by scar contracture. C Four weeks later, healing with good cosmetic outcome is noted. During healing, the wound is kept moist with an antibiotic ointment and semi-occlusive dressings. Courtesy, Sheldon V. Pollack, MD.
Table 30.4
General recommendations for facial skin care and education in patients with rosacea.
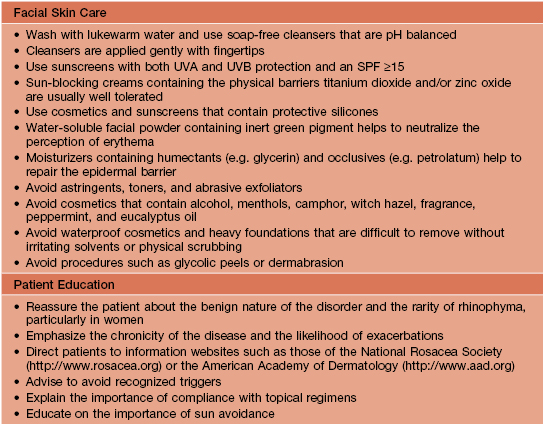
Adapted from Powell FC. Rosacea. N. Engl. J. Med. 2005;352:793–803; Pelle MT, Crawford GH, James WD. Rosacea: II. Therapy. J. Am. Acad. Dermatol. 2004;51:499–512; and Del Rosso JQ, Baum EW. Comprehensive medical management of rosacea: An interim study report and literature review. J. Clin. Aesthet. Dermatol. 2008;1:20–25.
For further information see Ch. 37. From Dermatology, Third Edition.
[/level-membership-for-dermatology-category][not-level-membership-for-dermatology-category]30
Rosacea and Periorificial Dermatitis
Epidemiology
Clinical Features
• Highly variable degree of severity, from a few papulopustules to extreme distortion of the nose.
• Table 30.1 lists the four major types of rosacea (Figs. 30.1–30.5) and their characteristics.
Table 30.1
Four major types of rosacea.
An individual patient may have more than one form. Some patients also have seborrheic dermatitis and/or actinic damage.
Fig. 30.1 Erythematotelangiectatic rosacea. Persistent erythema of the medial and lateral cheeks is seen. In this patient, there are no telangiectasias, indicating mild disease. Courtesy, Frank C. Powell, MD.
Fig. 30.2 Dermatoheliosis in a skin phototype I patient. Telangiectasias and erythema due to chronic actinic damage are particularly marked on the facial prominences. Features of dermatoheliosis overlap with those of erythematotelangiectatic rosacea. Courtesy, Frank C. Powell, MD.
Fig. 30.3 Rosacea. A Moderate papulopustular rosacea of the forehead. Note the superficial nature of the inflammatory lesions. B Moderate to severe papulopustular rosacea. There is a typical centrofacial distribution of erythema, telangiectasias, papules, and pustules. In addition, the skin has a scaly, crusty surface, and this is often a sign of more severe disease. Courtesy, Frank C. Powell, MD.
Fig. 30.4 Rhinophyma – early versus advanced disease. A Tortuous, telangiectatic vessels on the distal aspect of the nose contribute to its hyperemic appearance; this hyperemia may predispose to the subsequent hypertrophic changes of rhinophyma. Note the early sign of dilated follicles. B Distortion of nasal tissue due to tissue hypertrophy. Electrosurgery or laser therapy can be used to debulk and resculpt this nose. Courtesy, Frank C. Powell, MD.
Fig. 30.5 Ocular rosacea. A
[/not-level-membership-for-dermatology-category]
