72
Bites and Stings
Insects
• The bite of any insect can lead to a local cutaneous reaction whose intensity can vary depending on the individual’s level of sensitivity; the typical presentation is a 2 to 8 mm, erythematous urticarial papule in an exposed area (Fig. 72.1); lesions are often multiple and can be grouped.

Fig. 72.1 Insect bite reactions. In this patient, there are papulovesicles as well as excoriated papules with hemorrhagic crusting. In more darkly pigmented individuals, residual hyperpigmentation is common and can persist for months. Courtesy, Julie V. Schaffer, MD.
• Secondary changes consisting of excoriations may be present; less often, vesicles or bullae develop at the site of bites (Fig. 72.2).


Fig. 72.2 Insect bite reactions. Sometimes patients develop large, erythematous, edematous plaques (A) or frank bullae (B). Courtesy, Julie V. Schaffer, MD.
• Bite reactions typically resolve over 5–10 days; occasionally, patients develop persistent bite reactions that on biopsy may be diagnosed as pseudolymphoma (see Chapter 99).
• Postinflammatory hyperpigmentation is common, especially in patients with darkly pigmented skin.
• Secondary infection is a potential complication, most commonly from staphylococci or streptococci.
• Exaggerated bite reactions can be seen in patients with chronic lymphocytic leukemia; rarely, hypersensitivity reactions to mosquito bites that become necrotic can be associated with EBV infection (see Chapter 67).
• Anaphylaxis with urticaria and angioedema is generally due to stings from hymenopterids (bees, wasps, hornets, and fire ants) (Fig. 72.3).

Fig. 72.3 Fire ant bites presenting as clusters of sterile pustules on the foot. Courtesy, Dirk M. Elston, MD.
• Insects may be vectors of infectious diseases (Table 72.1).
Table 72.1
Major insects of dermatologic significance.
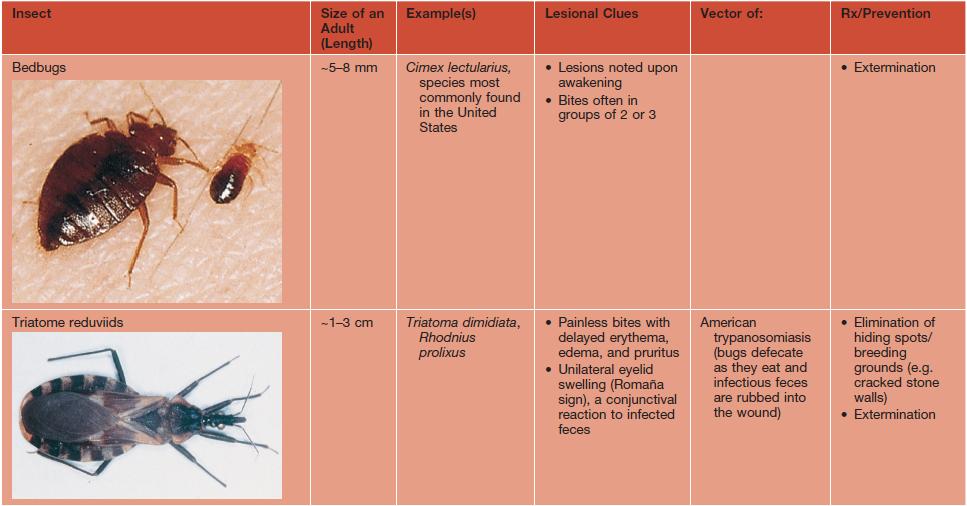
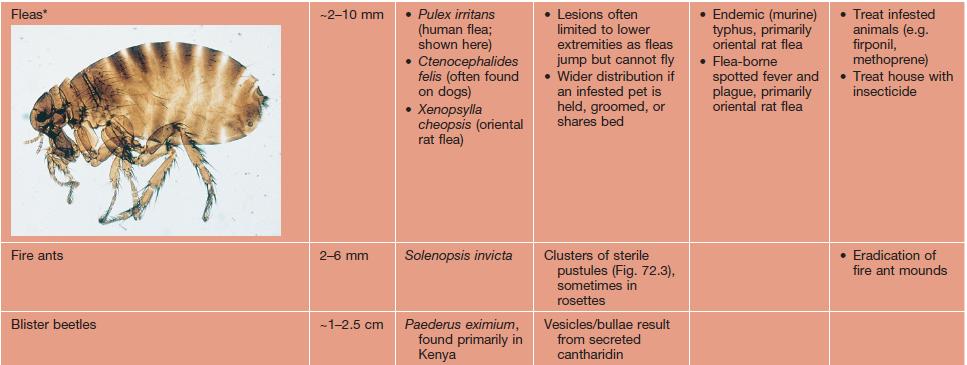
* See Chapter 71 for information on Tunga penetrans, a burrowing flea.
Photographs courtesy, Dirk M. Elston, MD.
Arachnids
Hard Ticks
• Ticks are important disease vectors, especially in the nymphal stage (Table 72.2; see Fig. 63.1); tick control measures are important for public health (see Fig. 63.8 for geographic distribution of vector tick species).
Table 72.2
Major ticks of dermatologic significance.
Dermacentor ticks primarily attach to the head and neck region; Amblyomma ticks prefer the lower legs and buttocks; Ixodes ticks may be found at any site, but the trunk is common.
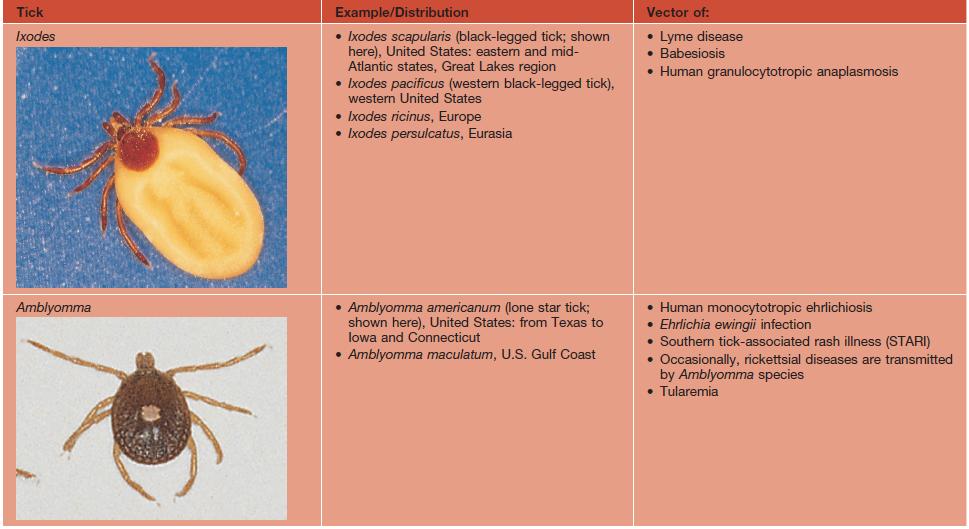
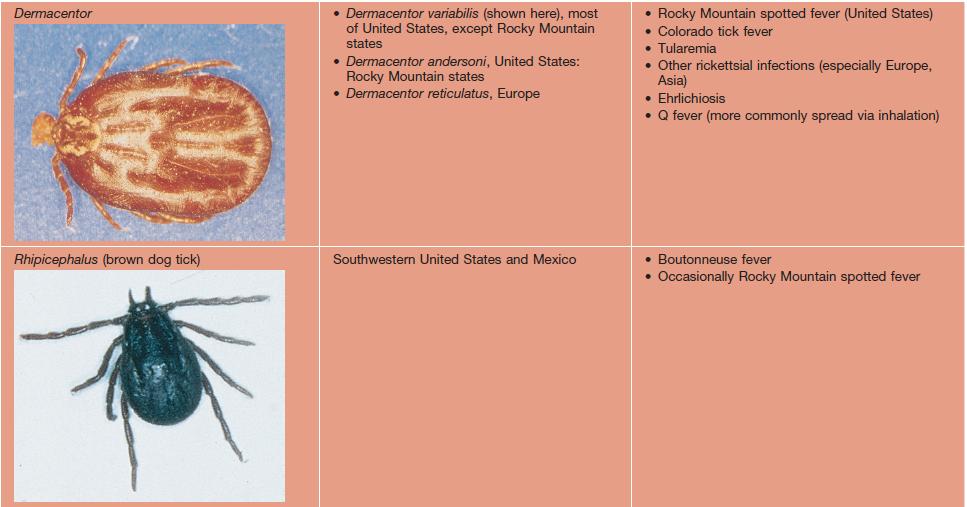
Photographs courtesy, Dirk M. Elston, MD.
• Prevention: permethrin repellent can be sprayed on clothing or other fabrics; protective clothing.
• Rx of persistent tick bite reactions: potent topical CS, intralesional CS, or even excision in severe cases; doxycycline is recommended in suspected cases of Rocky Mountain spotted fever (10-day course; see Chapter 63) or Lyme disease (14- to 21-day course).
Mites
• Thousands of species; parasitize humans as well as animals and plants.
• Human mites include Demodex folliculorum and D. brevis (may lead to folliculitis and exacerbate rosacea) and Sarcoptes scabiei, which causes scabies (see Chapter 71); these mites complete their life cycle on humans.
• Cheyletiella mites (‘walking dandruff’) are found on small mammals (e.g. cats, dogs) and may cause papulovesicular lesions in humans (Fig. 72.4).

Fig. 72.4 Cheyletiella bites. These mites are nonburrowing and are found on cats, rabbits, and dogs. Courtesy, Dirk M. Elston, MD.
Spiders
• Black widow spider (Latrodectus mactans is the primary species in the United States).
– Bites lead to acute pain and edema.
– Systemic symptoms may include an acute abdomen or rhabdomyolysis.
– Rx: if severe reaction, emergency medical treatment.
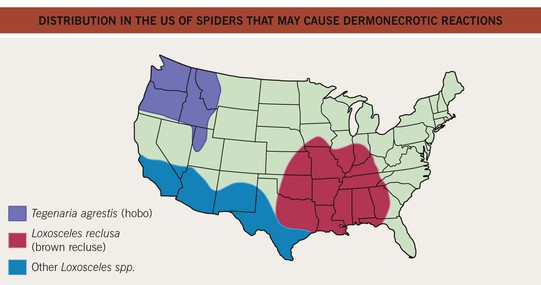
• Brown recluse spider (Loxosceles reclusa is the predominant species in the United States) (Fig. 72.5).
– Bites can cause dermonecrosis (sphingomyelinase D is the major toxin) which begins with erythema and/or vesiculation that becomes dusky, sometimes with bullae formation and eventual necrosis (Fig. 72.6).
– Rx: rest, ice, and elevation are the mainstay of treatment.

Marine Stings/Injuries
• Rx: for acute marine envenomations – soaking in hot water to denature venom proteins; for symptoms of delayed reactions or dermatitis – topical CS; for foreign body reactions – removal of foreign material.
– Pruritic papules, localized to the bathing suit area and intertriginous areas (Fig. 72.7).

For further information see Ch. 85. From Dermatology, Third Edition.






