11
Other Eczematous Eruptions
The major forms of dermatitis include atopic (see Chapter 10), contact (see Chapter 12), seborrheic, asteatotic (xerotic), stasis, and nummular. Dermatitis of special sites – i.e. hands, feet, lips, diaper area, and major body folds – is reviewed in Chapter 13, and pityriasis alba is reviewed in Chapters 10 and 54.
Seborrheic Dermatitis
• Common disorder with both an infantile and an adult form (Figs. 11.1 and 11.2); unusual in children.

Fig. 11.1 Infantile seborrheic dermatitis. Glistening red plaques of the neck, axillary and inguinal folds as well as the penis and umbilicus. Note disseminated lesions on the trunk and extremities. Courtesy, Robert Hartman, MD.



Fig. 11.2 Adult seborrheic dermatitis of the scalp, ear, and face. A Fairly sharply demarcated pink plaque with white and greasy scale. Note the fissure in the retroauricular fold. B Thin pink-orange plaques with yellow, greasy scale, especially of the melolabial fold and eyebrows. C Symmetric red-brown to violet plaques of the central forehead, nasal bridge, and medial cheeks with an associated hypopigmented figurate rim. A, Courtesy, Norbert Reider, MD, and Peter O Fritsch, MD; C, Courtesy, Jeffrey Callen, MD.
• Possibly related to components of sebum and Malassezia spp.
• DDx: psoriasis, contact dermatitis, other causes of diaper dermatitis (see Fig. 13.4), intertrigo (see Fig. 13.2) or blepharitis, tinea versicolor (presternal), tinea capitis (especially in children), atopic dermatitis, pityriasis amiantacea and dermatomyositis (scalp); may coexist with rosacea.
Asteatotic Eczema (Xerotic Eczema, Eczema Craquelé)
• Arises in areas of dry skin, especially during winter months, in dry climates and in older adults.
• The areas of dermatitis resemble a ‘dried riverbed’ or ‘crazy-paving’ with superficial cracking of the skin (Fig. 11.3).

Stasis Dermatitis
• Pruritic dermatitis with scale-crust and sometimes oozing that favors the shins and calves; historically often begins near the medial malleolus.
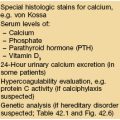
• Often accompanied by other signs of chronic venous hypertension (Table 11.1).
Table 11.1
Cutaneous signs of chronic venous hypertension.
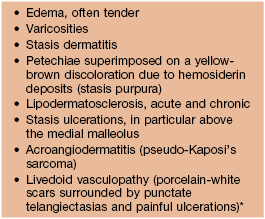
* Need to exclude causes of hypercoagulability.
• One of the more common causes of autosensitization (Fig. 11.4).

Fig. 11.4 Autosensitization dermatitis. There is dermatitis of the extensor surfaces of the upper extremities in this patient with allergic contact dermatitis to neomycin as well as stasis dermatitis and venous ulceration. Courtesy, Jean Bolognia, MD.
• DDx: allergic contact dermatitis, irritant contact dermatitis, asteatotic eczema, nummular dermatitis; may accompany other causes of the red leg, especially cellulitis and acute or chronic lipodermatosclerosis (Fig. 11.5), but the latter lack the clinical and histologic findings of dermatitis.
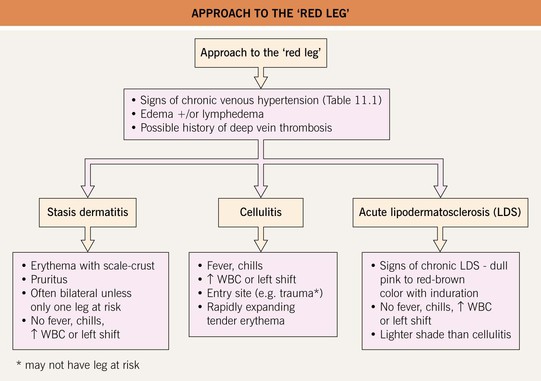
Fig. 11.5 Approach to the ‘red leg.’
Autosensitization Dermatitis (Id Reaction)
• Favored sites of involvement (in addition to primary site): extensor aspects of extremities (see Fig. 11.4), palms and soles, usually in a symmetric pattern.
• In children with tinea capitis, the id reaction often involves the head and neck region.
• Areas of dermatitis, often ill-defined, can be accompanied by excoriated papules (Fig. 11.6).

Fig. 11.6 Id reaction in a child due to allergic contact dermatitis (ACD) to nickel. Square-shaped area of ACD due to nickel in a buckle surrounded by multiple crusted edematous papules. Courtesy, Julie V. Schaffer, MD.
• DDx: atopic dermatitis, widespread contact dermatitis (e.g. textiles), Gianotti–Crosti syndrome, drug eruption to systemic anti-fungal medication (tinea capitis id), eczematous drug eruptions (e.g. calcium channel blockers [unusual]).
Infectious Eczematous (Eczematoid) Dermatitis
Nummular Eczema (Nummular Dermatitis)
• Markedly pruritic, coin-shaped lesions of dermatitis, usually measuring 2 or 3 cm in diameter (Fig. 11.7).

Fig. 11.7 Nummular eczema. Coin-shaped lesions of acute and subacute dermatitis that are fairly well demarcated. There is often marked pruritus. Courtesy, Kalman Watsky, MD.
• Occurs primarily on the extremities, classically the legs in men and the arms in women.
• DDx: atopic dermatitis, autosensitization dermatitis, impetigo, stasis dermatitis, allergic contact dermatitis, tinea corporis, vesicular pityriasis rosea, mycosis fungoides.
• Rx: in addition to topical CS and calcineurin inhibitors, often requires phototherapy to clear.
Dyshidrotic Eczema (Acute and Recurrent Vesicular Hand Dermatitis)
• Firm, pruritic vesicles of the palms > soles as well as the lateral and medial aspects of the digits (Fig. 11.8); chronic and recurrent.

Fig. 11.8 Dyshidrotic eczema. Clusters of firm vesicles along the lateral aspect of the thumb and hypothenar eminence. Courtesy Louis A. Fragola, MD.
• When larger vesicles develop, the term pompholyx is sometimes used.
Juvenile Plantar Dermatosis
• The skin is dry and scaly with mild inflammation and a characteristic glazed appearance (Fig. 11.9).

Fig. 11.9 Juvenile plantar dermatosis in a child. Erythema and scaling of the plantar surface of the forefoot, especially the ball of the foot and the great and fifth toes. Note the glazed appearance of the skin of the left foot. Courtesy, Kalman Watsky, MD.
• Thought to be related to hydration of the stratum corneum from wearing shoes made of impermeable materials and subsequent shearing of skin due to friction.
• DDx: other causes of foot dermatitis (see Table 13.1), especially psoriasis, allergic contact dermatitis (e.g. rubber, chromates in leather), tinea pedis (interdigital toe webs involved), atopic dermatitis.
• Rx: permeable socks and shoes, emollients, CS ointments, removal of wet socks along with wet shoes.