Chapter 58 Radiation Retinopathy
Introduction
Radiation retinopathy (RR) is a slowly progressive, delayed-onset occlusive microangiopathy of the retinal vasculature that occurs with variable latency after exposure of the retina to ionizing radiation. First described by Stallard in 1933,1 the term encompasses all retinal vascular changes, including ischemic and proliferative RR (PRR) and radiation maculopathy. It is a potentially devastating sequela of exposure of the eye to any source of radiation, including local plaque radiation treatment (brachytherapy), external-beam radiation treatment (ERBT), proton beam radiation, helium ion radiotherapy and gamma knife radiotherapy of the eye, ocular adnexa, orbit, and head and neck structures.2–6 Radiotherapy offers an alternative to enucleation for patients with retinoblastoma, choroidal melanoma, and ocular metastases,7–9 as well as life-saving treatment of orbital, sinus, and intracranial tumors. Since the Collaborative Ocular Melanoma Study showed similar survival rates after radiotherapy and enucleation, the shift towards globe-salvaging therapeutic strategies has increased the use of radiation and consequently increased its complications, with reports of the incidence of RR ranging from 3% to over 20%.10,11 The current interest in use of radiation in the treatment of neovascular age-related macular degeneration (AMD) might further increase the risk of this complication.12
The risk of RR is related to characteristics of the radiation treatment itself, the presence of systemic disease, and exposure to radiation sensitizers such as chemotherapy. Fundoscopic findings can be highly variable, ranging from scattered retinal hemorrhages, microaneurysms, and cotton-wool spots to macular edema, large-vessel occlusion, extensive ischemic retinopathy and maculopathy and consequent retinal and ocular neovascularization. Within the retina, the posterior pole is particularly sensitive to this pathology,13 with grave implications for visual prognosis. Further, RR has a long latency and may not be clinically detectable for 8 years or more.14
Etiology, pathogenesis, and histopathology
RR can be described as a progressive obliterative arteritis that initiates a characteristic pattern of degenerative and proliferative vascular changes and microvascular dysfunction. Radiotherapy is the most frequent cause. Radiotherapy generates its effective tumoricidal effects both directly, via injury to the DNA of rapidly dividing cells, and indirectly, via the production of free radicals. However, these processes damage vascular and interstitial support structures of both pathological and healthy tissue. Histopathologically, ionizing radiation of the retina induces an acute transudative as well as a slowly progressive occlusive vasculopathy.15 The initial pathologic change, and the fundamental abnormality, is retinal vascular endothelial cell injury and loss15–18 and associated inflammation,19 which occurs primarily in capillaries, followed by capillary closure, clearly visible with fluorescein angiography (FA),14,20–22 retinal ischemia, nerve tissue necrosis, and fibrovascular proliferation.13,18,21,23,24
The loss of capillary cellularity leads to the development of microaneurysms, and hemodynamic alterations produce fenestrated telangiectatic retinal vessels. Larger retinal vessels become involved later in the course of the retinopathy, with diameter reduction of up to 75% in major retinal arteries and veins demonstrated in animal models.19 Closure of blood vessels is the single most characteristic finding on FA. Ghost vessels are later visible ophthalmoscopically. Central retinal artery occlusion has also been described as a consequence of high-dose irradiation,25 as has interruption of the choroidal circulation.26,27 The choriocapillaris also suffers, and hypoperfusion is detectable several months after treatment,27 leading to choroidopathy and chorioretinal atrophy. The widespread vascular occlusion induces the production of vascular endothelial growth factor (VEGF),18 leading to neovascularization and an increase in vascular permeability, both of which result in vascular leakage and tissue edema.28 Uveal effusion can also be present.
The disappearance of choriocapillaris, retinal pigment epithelium (RPE), photoreceptors and retinal nerve fibers, along with leukocyte invasion, has been demonstrated histologically.29 Areas devoid of photoreceptor cells correspond with areas of pigment dispersion with reduced numbers of melanocytes. There is a thickening of arteriolar and capillary walls and endothelial cell loss. In contrast to diabetic retinopathy, in which pericytes are initially affected, RR exhibits an early loss of endothelial cells. However, pericytes can be affected in severely damaged capillaries.
On optical coherence tomography (OCT) images, significant thinning of the inner plexiform, inner nuclear, and outer plexiform layers is visible, suggesting that radiation-induced damage is confined to the inner layers of the retina.30 However, secondary functional changes may occur in the outer retina.31
Natural history and clinical features
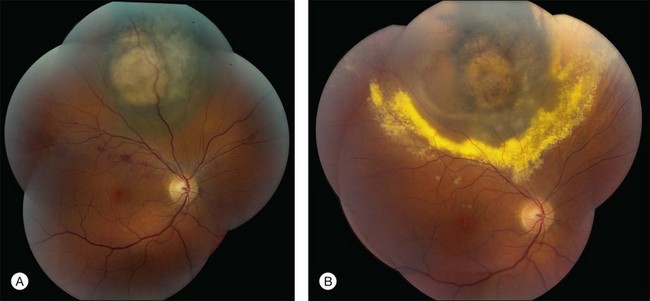
RR displays clinical and angiographic features that are virtually identical to those seen in diabetic retinopathy.32 This is to be expected, since both radiation and diabetes primarily damage the retinal capillaries. Ophthalmoscopically, microaneurysms are the first to appear and are near-universally present,33 closely followed by intraretinal hemorrhages, macular capillary dilation and nonperfusion, and nerve fiber layer infarcts (cotton-wool spots; Fig. 58.1).14 Retinal edema, hard exudates, telangiectasia, and perivascular sheathing may follow in variable sequence and latency. Hard exudates have been found to be more prevalent after brachytherapy (Fig. 58.2), whereas retinal hemorrhages and microaneurysms are more commonly found after EBRT.13 The telangiectatic-like vessels are a feature of established retinopathy and are likely to represent collateral vasculature at the edges of capillary occlusion.14 Confluent areas of capillary closure lead to the development of large areas of retinal capillary nonperfusion.
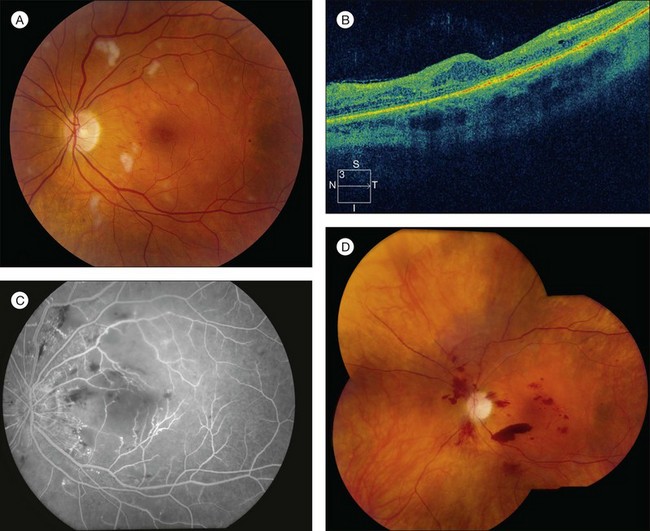
The fluorescein angiographic hallmarks of the condition are the presence of severe retinal capillary nonperfusion, capillary dilation, and microaneurysms, frequently in combination with macular edema or ischemia.13 Central macular chorioretinal anastomosis has also been described.34 Neovascularization may develop later (Fig. 58.1), and does so in approximately 32% of eyes with RR.35 This development is referred to as PRR, and its presence is ominous. Analogous to proliferative diabetic retinopathy, it suggests profound ischemia and carries a worse prognosis for long-term visual acuity. If left untreated, it can lead to neovascular glaucoma, vitreous hemorrhage, and tractional retinal detachment caused by fibrovascular proliferation similar to that seen in diabetic retinopathy. However, in contrast to diabetic retinopathy and other retinal vasculopathies, neovascularization does not typically extend through the internal limiting membrane into the vitreous.18 Nevertheless, vitreous hemorrhage can occur and its presence is associated with a poor prognosis for both vision and globe salvage, as well as for ghost cell or neovascular glaucoma. It also impedes the clinician’s ability to monitor the retinopathy and to employ laser photocoagulation to treat progression (Table 58.1).
| Complication | Incidence |
|---|---|
| Nonproliferative radiation retinopathy | 68% |
| Proliferative radiation retinopathy | 32% |
| Clinically significant macular edema | 76% |
| Macular ischemia | 76% |
| Radiation optic neuropathy | 55% |
| Cataract | 52% |
| Vitreous hemorrhage | 24% |
| Glaucoma | 12% |
| Radiation keratopathy | 10% |
| Tractional retinal detachment | 5% |
(Adapted from Kinyoun JL. Long-term visual acuity results of treated and untreated radiation retinopathy (an AOS thesis). Trans Am Ophthalmol Soc 2008;106:325–35.)
Classification
There is currently no standard method of classification for RR, although several methods have been developed. These can be categorized as clinical or ophthalmoscopic, fluorescein angiographic and OCT. Finger and Kurli proposed a four-stage, prognosis-related classification that uses ophthalmoscopic and fluorescein angiographic findings to classify macular and extramacular changes.36 In this system, stage 1 includes extramacular ischemic changes, stage 2 includes macular ischemic changes, stage 3 includes additional macular edema and retinal neovascularization, and stage 4 encompasses vitreous hemorrhage and at least 5 disc areas of retinal ischemia, whether macular or extramacular. The Early Treatment Diabetic Retinopathy Study (ETDRS) definition of clinically significant macular edema has been applied to macular edema associated with radiation damage. In these cases, it is referred to as clinically significant radiation macular edema, which follows the ETDRS definitions: retinal thickening within 500 mm of the fovea; edema-associated hard exudates within 500 mm of the fovea; and one or more zones of retinal thickening ≥1 disc area, any part of which is within 1 disc diameter of the fovea.37 FA allows the clinician to determine the condition of the macula, allowing maculopathy to be subdivided into ischemic and nonischemic variants, which has a significant impact on the visual outcome. FA also allows for the classification of macular edema, which is useful if grid or focal laser photocoagulation is to be administered. OCT is increasingly used to guide diagnosis and treatment decisions for macular edema in various retinal disorders.38 Horgan et al. proposed a five-point OCT-based grading scale based on standard reference OCT images: grade 1, extrafoveolar, noncystoid edema; grade 2, extrafoveolar cystoid edema; grade 3, foveolar noncystoid edema; grade 4, mild-to-moderate foveolar cystoid edema; and grade 5, severe foveolar cystoid edema.39 This study demonstrated OCT evidence of macular edema as early as 4 months after plaque radiotherapy for uveal melanoma, with a peak incidence at 12–18 months, and that it is associated with significant vision loss. The use of OCT is important, because macular edema is visible on OCT approximately 5 months earlier than clinically detectable radiation maculopathy.39 The classification of RR into PRR and nonproliferative (NPRR) subtypes is also of great prognostic importance. A recent retrospective study reported an incidence of PRR of 5.8% at 5 years and 7% at 10 and 15 years in 3841 eyes treated with plaque radiotherapy for uveal melanoma.40
Risk factors
Risk factors for the development of RR can be divided into internal (inherent/patient) and external (iatrogenic) factors. The primary patient factor is concomitant vascular disease such as diabetes mellitus.41 Since both diabetes and radiation primarily damage the retinal capillaries, this synergistic effect is to be expected, as the capillaries experience an early loss of pericytes due to diabetes and endothelial cell loss due to radiation. Destruction of these two cell types leaves little cellular structural support for capillaries and thus results in capillary closure, aneurysms, vessel leakage, and hemorrhage. Indeed, it has been suggested that concomitant diabetes mellitus is also a poor prognostic indicator for visual acuity, increasing the risk of visual loss by nearly 300%.42 This is in part due to the fact that diabetes mellitus is associated with an increased incidence and severity of neovascular complications, including neovascular glaucoma43 and radiation papillopathy44 following radiotherapy.45 Other vascular disorders predisposing to RR are arterial hypertension and coronary artery disease.46 Tumor characteristics likely to lead to a worse prognosis include large tumors and close proximity to the macula and optic disc.47
Chemotherapy, whether or not concurrent/concomitant with the radiation therapy, also increases the risk,13,48 as may pregnancy.49 Chemotherapy increases the vulnerability of the retinal vasculature to radiation damage, possibly via an increase in oxygen-derived free radicals.23 It also increases the risk of proliferative (or neovascular) RR, which carries a worse prognosis than the nonproliferative type.50 The concomitant administration of chemotherapy increases the risk of visual complications,13,23,48,51–53 potentiates the development of RR at lower radiation doses,13 and may shorten the latent period between exposure and retinopathy.48,52,54
Incidence and dosimetry
The most important external or iatrogenic risk factors relate to the radiation itself. These are radiation type, treatment modality (external beam versus brachytherapy or plaque), total radiation dose and the fractionation schedule of that dosage, the total elapsed time in the course of irradiation treatment, and errors in treatment technique and/or dosage calculations.53,55
Radiation type
If a large enough dose is applied, any type of radiation can result in retinopathy and its associated complications. RR is found in 87% of patients after plaque radiotherapy for juxtapapillary melanomas, and radiation maculopathy in 89% after proton beam irradiation. However, neither of these radiation types is as highly associated with severe sight-limiting complications (such as rubeosis and neovascular glaucoma) as gamma knife treatment, which may lead to complete loss of vision in nearly 50%.5






