7 Psychiatric assessment
History taking
The psychiatric history
Interviewing technique
As with any patient, aim for an open, empathic and non-judgemental approach and maintain non-threatening eye contact as much as possible. Start with open questions, avoid loaded questions, encourage the patient to tell his story in his own words and follow the approaches for general history taking detailed in Chapter 1. Another way of questioning is to use a normalizing statement. This is employed when you are asking about symptoms or behaviours which the patient may find embarrassing or difficult to acknowledge. For example, you might say something like ‘Sometimes when people have been feeling very depressed or have been under great stress, they may have odd experiences which they cannot explain, for example they may hear or see things which are unusual – has anything like this happened to you?’ Further examples of these are provided in the appropriate sections. Finish with a summary of what you have understood and check with the patient if you have missed anything that he feels is important.
Order of sections
The order in which the sections of the history are covered is suggested in Box 7.1 and followed in the text. Conventionally, past medical and psychiatric history goes at the end. However, if it is impossible to complete the interview on a single occasion, it is more useful to have found out about previous psychiatric illness, current contact with mental health services, medication and important medical conditions than it is to know the patient’s father’s occupation or what jobs he has done.
Box 7.1 Suggested order for psychiatric history







History of presenting complaint
Patients may volunteer symptoms which may be associated with the presentation. If none are volunteered, a systematic enquiry is essential. For example, in a patient presenting with depression, enquire about other symptoms in the depressive syndrome (Box 7.2) such as concentration, memory, enjoyment and social withdrawal. Anxiety and depression frequently coexist and so either presentation should lead to systematic enquiry about symptoms of the other. Somatic and psychic symptoms of anxiety are outlined in Boxes 7.3 and 7.4.
Box 7.2 Features supporting a diagnosis of depression
 Persistent/pervasive low mood, often tearfulness
Persistent/pervasive low mood, often tearfulness
 Diurnal variation of mood, typically worse in the morning
Diurnal variation of mood, typically worse in the morning

 Anhedonia, i.e. inability to experience pleasure in things
Anhedonia, i.e. inability to experience pleasure in things
 Irritability and/or poor concentration
Irritability and/or poor concentration
 Lethargy, fatigue and lack of energy
Lethargy, fatigue and lack of energy
 Sleep disturbance, usually early-morning waking
Sleep disturbance, usually early-morning waking
 Appetite and weight loss (increased in atypical depression)
Appetite and weight loss (increased in atypical depression)
 Constipation and/or loss of libido
Constipation and/or loss of libido
 Ideas of hopelessness, worthlessness, guilt, persecution, nihilism
Ideas of hopelessness, worthlessness, guilt, persecution, nihilism
 Loss of confidence and social withdrawal
Loss of confidence and social withdrawal
 Self-deprecation and/or self neglect
Self-deprecation and/or self neglect
 Motor retardation, leading to depressive stupor
Motor retardation, leading to depressive stupor




Box 7.3 Somatic symptoms of anxiety






















Personal history
Birth and early developmental milestones
This begins with enquiry about the patient’s birth. Was it a normal delivery or were there any medical interventions or birth complications requiring specialist care? This is relevant to assess the possibility of any early brain injury. It can also be relevant if there were problems in early maternal bonding. Were developmental milestones reached within the normal range (see Ch. 5)? Patients may not have any knowledge about their birth and milestones. If they tell you about some problem surrounding their birth and early milestones, this may be significant and is worth recording. If no problems are identified, it is possible that the patient just does not know. Clearly an informant, such as the patient’s mother, may have more accurate information.
Family milieu, childhood health and early relationships with caregivers






Psychosexual history, including marital/relationship history and children
The psychosexual history can be a source of embarrassment for students and patients, but this is unnecessary if handled in a straightforward way. If there is a problem, the patient may be relieved to be asked about this, as he may have found it difficult to mention. Many psychotropic drugs have psychosexual side effects (e.g. erectile dysfunction with some antidepressants), but patients may not mention these side-effects unless asked. How much detail is needed will vary depending on the presenting complaint. Obviously, if the patient is complaining of marital or psychosexual difficulties, a full history of this area is relevant. The level of detail outlined in Box 7.5 is usually not necessary, but you should routinely gather basic details of the psychosexual history. In the relationship history, do not make an assumption about sexual orientation. Ask about sexual orientation in an open non-judgemental way. Look for patterns which may be indicative of relationship problems (lots of brief relationships, a repeated pattern in intimate relationships, repeatedly entering into abusive relationships). Be aware of domestic violence and the need to ask about this if there is a very difficult or aggressive relationship. Basic details about children (also in Box 7.5) can be important later if child-protection issues are raised.








Current social situation – see Box 7.6




Use of alcohol and non-prescribed recreational drugs
Alcohol
Ascertain quantity and frequency of alcohol intake. If the level of alcohol use is above safe drinking limits (Box 7.7), or if there are other indicators of a problem with alcohol (Box 7.8), a full drinking history should be taken and symptoms of alcohol dependence should be sought (Box 7.9). A very brief and commonly used screen for alcohol dependence is a questionnaire called the CAGE (Box 7.10). Alcohol misuse is drinking which causes physical, social or psychological harm to the drinker. Alcohol dependence is when the criteria for a dependence syndrome are met (Box 7.9).
Box 7.7 Units of alcohol and safe drinking limits
1 unit contains 10 g of pure alcohol and is equal to half a pint of beer, one small glass of table wine or one bar measure of spirits (for more detail, see Box 1.12):


Box 7.8 Features suggesting alcohol misuse

 Secret drinking and drinking alone
Secret drinking and drinking alone

 Amnesia for events during episode of drinking
Amnesia for events during episode of drinking
 Drink driving convictions or other alcohol-related crime
Drink driving convictions or other alcohol-related crime
 Violent behaviour related to consumption
Violent behaviour related to consumption
 Marital problems related to consumption
Marital problems related to consumption
 Employment problems related to consumption
Employment problems related to consumption

 Patient is evasive or vague when questioned about intake
Patient is evasive or vague when questioned about intake



Box 7.9 Features of alcohol dependence










Taking a full drinking history
You need to obtain as accurately as possible an estimate of quantity, type and pattern of alcohol consumption as well as effects of alcohol on life. Patients are frequently in denial and will underestimate their intake. The most efficient way to take the history is to ask about a typical drinking day or week. Go through the day ascertaining type, quantity and context of alcohol intake. Cover the features listed in Boxes 7.8 and 7.9 to establish if there is alcohol misuse or dependence.
Personality assessment
Do not rely too heavily on a patient’s self-assessment of personality, though it is important to hear how he views himself. The depressed patient may paint a picture of himself as incompetent and lacking in confidence, which may be far from his premorbid personality. To avoid such misrepresentations, try to rely on objective information in the history and, where possible, talk to an informant who knows the patient well about what he is usually like. The important areas to cover in assessing personality are shown in Box 7.11.





The mental state examination
Observations and interpretations should be recorded separately. A mental state examination consisting solely of the doctor’s interpretations is of little use. For example, a patient may say that the police are in a conspiracy against him and are monitoring his flat with listening devices in the walls. It is inadequate just to record that the patient has paranoid delusions. It may not be a delusion. It could be true, or he could be intentionally creating fantasy stories. The record should include what the patient actually says and then state ‘This belief seems to be a delusion’. A basic comprehensive structure is outlined in Box 7.12 with a detailed outline of what should be recorded under each heading.







Appearance and behaviour
Behaviour
Reduced motor activity
In bradykinesia, voluntary movements are reduced and abnormally slow. The face and arms tend to be particularly affected. Bradykinesia is most commonly caused by parkinsonism due to Parkinson’s disease or medication, particularly antipsychotics. Slowness and paucity of movement may also occur in psychomotor retardation, which is a feature of depression and indicates quite severe depression. In stupor, there is severe paucity of movement and mutism. This occurs in severe depression, catatonia and organic brain disease. Catatonia is characterized by a stuporose state with additional features (see Boxes 7.13 and 7.14).
Box 7.13 Movement changes in the mental state examination
 Dystonia: due to older major antipsychotic drugs
Dystonia: due to older major antipsychotic drugs
 Choreiform: Huntington’s chorea – common with l-dopa therapy (for Parkinson’s disease)
Choreiform: Huntington’s chorea – common with l-dopa therapy (for Parkinson’s disease)
 Tics: quite frequent in childhood and during periods of emotional stress
Tics: quite frequent in childhood and during periods of emotional stress



 Catatonia: (see also Box 7.14) striking condition characterized by stupor, sometimes alternating with excited motor and behavioural features. Motor excitation can be extreme and lead to injury or exhaustion, which can be lethal
Catatonia: (see also Box 7.14) striking condition characterized by stupor, sometimes alternating with excited motor and behavioural features. Motor excitation can be extreme and lead to injury or exhaustion, which can be lethal
Box 7.14 Variable features of catatonia
 Waxy flexibility: the patient maintains a posture in which he has been placed by the examiner
Waxy flexibility: the patient maintains a posture in which he has been placed by the examiner
 Negativism: the patient seems to behave in the opposite way to that requested by the examiner
Negativism: the patient seems to behave in the opposite way to that requested by the examiner
 Aversion: the patient turns away when addressed
Aversion: the patient turns away when addressed



 Posturing: the patient adopts an unusual posture for a prolonged period, e.g. symbolic like a cross
Posturing: the patient adopts an unusual posture for a prolonged period, e.g. symbolic like a cross
 Automatic obedience: the patient shows excessive compliance (opposite of negativism)
Automatic obedience: the patient shows excessive compliance (opposite of negativism)
 Echopraxia: the patient exactly imitates the interviewer
Echopraxia: the patient exactly imitates the interviewer
 Advertance: the patient frequently turns to the interviewer in an exaggerated way
Advertance: the patient frequently turns to the interviewer in an exaggerated way
 Mitgehen: the interviewer can move the patient’s limbs with fingertip pressure
Mitgehen: the interviewer can move the patient’s limbs with fingertip pressure

Increased motor activity
Note any excessive activity and whether it is purposeful or not. Manic patients may just be overactive and distractable. Agitation has a different quality, being driven by an unpleasant inner sense of tension. It is a general restlessness in which there may be apparently purposeful activity but it is not carried through properly. There may be repetitive purposeless behaviour such as hand-wringing, scratching, rubbing hands on knees and pacing up and down. See Box 7.13.
Speech
This is divided into two components: rate and structure of speech.
Structure
This can be disrupted in a variety of ways and due to a range of disorders (Box 7.15).
Box 7.15 Disorders of structure of speech
 Circumstantial: frequent digressions, taking a long time to get to the point, e.g. in obsessive compulsive disorder, epilepsy and organic brain disorders
Circumstantial: frequent digressions, taking a long time to get to the point, e.g. in obsessive compulsive disorder, epilepsy and organic brain disorders


Thought
The exploration of depressive thoughts is described in Box 7.16. It is important always to establish whether or not a patient experiences suicidal thoughts, and this is part of risk assessment. It is negligent to perform a psychiatric assessment without a basic risk assessment. Medical students and doctors may feel uncomfortable asking about suicidal ideas or may fear that asking about suicidal thoughts increases the likelihood that the patient will act upon them. Research has shown that the opposite is the case. Patients are often relieved to share these feelings, and welcome this opportunity.










It is important to pursue a risk assessment to determine the likelihood of patients acting on thoughts of suicide or self-harm. Ask what he has thought of doing and whether he has done anything to prepare (e.g. saving up tablets). Look for protective factors by asking what it is that stops him acting on his suicidal thoughts and how he copes with the thoughts. Box 7.17 summarizes important risk factors for completed suicide which the student should know about and explore in assessing risk.
Box 7.17 Features suggesting increased risk of suicidal behaviour








Exploring thoughts in elevated mood
Patients with elevated mood states (mania or hypomania) will often mention all kinds of grandiose ideas while you are taking a history and may have disinhibited behaviour. Specific questions to ask if they have not already come up are listed in Box 7.18.

Abnormal beliefs
The main types of abnormal belief are primary and secondary delusions, overvalued ideas and sensitive ideas of reference (Box 7.19).
Primary delusions (also called true delusions) are delusions which are not secondary to other abnormal mental processes such as abnormal mood or hallucinations. A particular example of a primary delusion is a delusional perception in which a patient has a normal perception to which he attaches delusional significance. For example, a patient may see a waiter pick up a glass (a normal perception) and the patient realizes immediately that the waiter is an envoy of the devil (delusional significance). Primary delusions are generally associated with schizophrenia provided they occur in clear consciousness (i.e. they are not occurring in an organic confusional state). Indeed they are one of the Schneiderian first-rank symptoms of schizophrenia (see Boxes 7.20 and 7.21).
Box 7.20 Diagnosis of schizophrenia
1 Audible thoughts: auditory hallucination of hearing thoughts while thinking them (Gedankenlautwerden) or as an echo immediately after thinking them (echo de la pensée)
2 Argumentative voices: two or more voices referring to the patient in the third person in an argumentative manner, e.g. ‘He’s an odd sort of fellow’, ‘No, he is evil’
3 Auditory hallucinations of running commentary on behaviour referring to the patient in the third person, e.g. ‘Now he is opening the door’
4 Thought insertion or thought withdrawal
6 Passivity ‘made’ experiences (experiences arising without the patient’s volition and outside his control)
Box 7.21 Distinction between positive and negative symptoms of schizophrenia
Positive symptoms





Negative symptoms
 Tend to be chronic and accumulate as the illness progresses
Tend to be chronic and accumulate as the illness progresses
 Poverty of speech – the patient has little to say and very little spontaneous speech
Poverty of speech – the patient has little to say and very little spontaneous speech

 Blunting of affect – absence of normal modulation of mood and lack of emotional response
Blunting of affect – absence of normal modulation of mood and lack of emotional response
 Lack of volition – loss of motivation; can be extreme when patient neglects basic self-care
Lack of volition – loss of motivation; can be extreme when patient neglects basic self-care

When eliciting delusional beliefs, and because psychotic symptoms are often very bizarre, it is wise to put patients at ease by making some kind of normalizing statement and asking a very open general question first. For example, you might say ‘Some people find that when they are feeling very stressed or having difficulties with how they are feeling, they have some rather odd experiences. Has anything very odd or unusual happened to you recently?’ Follow up on any positive responses with open questions, asking the patient to describe his experiences in detail. If there are no positives, you can screen for certain sorts of delusions. Some of these, and suggested screening questions, are given in Box 7.22.
Perception
There is a wide range of abnormal perceptual experiences, some of which can be part of normal experience and others which are indicative of mental illness or organic disease of the brain. It may be obvious from his behaviour that a patient is seeing things or attending to auditory hallucinations. Gentle enquiry about what the patient sees or hears will often elicit a description of the experience. Record as much detail as possible. Patients may be embarrassed to mention having had abnormal experiences, so specific enquiry is needed. For patients who have not had these experiences, being asked about them can be quite threatening as they may feel the doctor is suggesting they are ‘mad’. To deal with this, it may be appropriate to make a normalizing statement first, and then ask a screening question for abnormal perceptual experiences: ‘It is quite common for people to have unusual experiences which may puzzle them. For example, some people may hear noises, music or voices when there is no one there, or people may see things which others are not able to see. Have you ever had any experiences like these?’ If the patient has had such experiences, they can then be explored in more detail (Box 7.23).









Abnormal perception
Hallucinations are perceptions that are not based on any real external stimulus. They can occur in any sensory modality but the commonest are auditory, for example a voice being heard by the patient but no one else hears it. Auditory hallucinations occur in many disorders including schizophrenia, organic brain disease and manic depressive illness. Voices can be heard speaking in the second or third person. In severe depression, voices are often second person and the content may be mood congruent, for example ‘Look at you, you are useless, do away with yourself’. The manic patient may hear God’s voice telling him he has special powers. Third-person hallucinations in the absence of organic disease suggest schizophrenia (see Box 7.20 for first-rank symptoms).
Tactile hallucinations are difficult to distinguish from illusions. In cocaine psychosis, patients may complain that insects are crawling over them (formication). Patients with schizophrenia can describe tactile hallucinations which may be incorporated into their delusional beliefs, for example a patient may feel sensations on their skin and believe this is due to aliens taking specimens from them. In the absence of organic brain disease, tactile hallucinosis is a first-rank symptom of schizophrenia (see Box 7.20).
Abnormal experiences of self and environment are listed in Box 7.24.
Cognition
 What is the patient’s level of consciousness?
What is the patient’s level of consciousness?

 Is he fully alert and behaving appropriately for the context?
Is he fully alert and behaving appropriately for the context?

Basic assessment of cognitive function
A useful and commonly used semi-quantitative measure is the Mini-Mental State Examination (MMSE) (Box 7.25). Scores are to some extent dependent on educational level. The test has subcategories related to orientation, registration, attention, recall and language. The maximum score is 30, and scores lower than 21 are associated with cognitive impairment. The MMSE cannot differentiate multifocal from diffuse organic brain disease, but it provides a useful baseline assessment of a patient’s cognitive performance.
Box 7.25 Mini-Mental State Examination
Registration
Award 1, 2 or 3 points according to how many the patient can repeat.
Resubmit list until patient is word perfect in order to use this for a later test of recall.
Language
1 point each for two objects correctly named (e.g. pencil and watch) (2 points).
1 point for correct repetition of ‘No ifs, ands and buts’ (1 point).
1 point for correct response to a written command, such as ‘close your eyes’ (1 point).
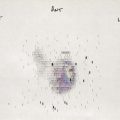
Test the patient’s ability to copy a complex diagram of two intersecting pentagons (1 point).
Level of consciousness
The patient’s level of alertness or, if he is unconscious, the level of unconsciousness may be assessed. Some patients have fluctuating levels of consciousness; the mental state may then fluctuate between lucidity and gross abnormality. This is a manifestation of an acute organic confusional state. For a fuller account of the examination of the unconscious patient, see Chapters 8 and 14.