[level-membership-for-dermatology-category]
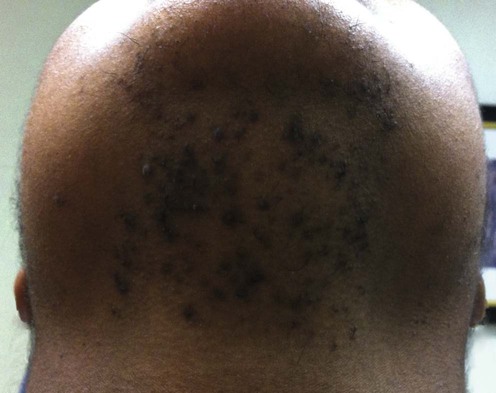
Pseudofolliculitis barbae



Specific investigations


An unusual Ala12Thr polymorphism in the 1A alpha-helical segment of the companion layer-specific keratin K6hf: evidence for a risk factor in the etiology of the common hair disorder pseudofolliculitis barbae.
The authors somehow conclude that this gene represents a significant genetic risk factor for PFB.
First-line therapies
 Beard growth
Beard growth Razor shaving technique
Razor shaving technique Hair clippers
Hair clippers Chemical depilatories
Chemical depilatories Adjunctive hair extraction
Adjunctive hair extractionSecond-line therapies
 Retinoic acid
Retinoic acid Glycolic acid
Glycolic acid Topical clindamycin
Topical clindamycin
Third-line therapies
 Laser depilation
Laser depilation Surgical depilation
Surgical depilation[/level-membership-for-dermatology-category][not-level-membership-for-dermatology-category]
Pseudofolliculitis barbae
Specific investigations
An unusual Ala12Thr polymorphism in the 1A alpha-helical segment of the companion layer-specific keratin K6hf: evidence for a risk factor in the etiology of the common hair disorder pseudofolliculitis barbae.
Buy Membership for Dermatology Category to continue reading. Learn more here
[/not-level-membership-for-dermatology-category]
