[level-membership-for-dermatology-category]41
Porphyrias
The porphyrias represent a group of metabolic disorders in which there is dysfunction of the enzymes involved in heme synthesis (Fig. 41.1). With the exception of acquired porphyria cutanea tarda (PCT), the underlying etiology is monogenetic mutations. Porphyrins absorb light energy (400–410 nm) and their accumulation within the skin can lead to photosensitization, with water-soluble porphyrins producing blisters and lipophilic porphyrins leading to acute burning and erythema. This chapter focuses on those porphyrias with cutaneous manifestations.
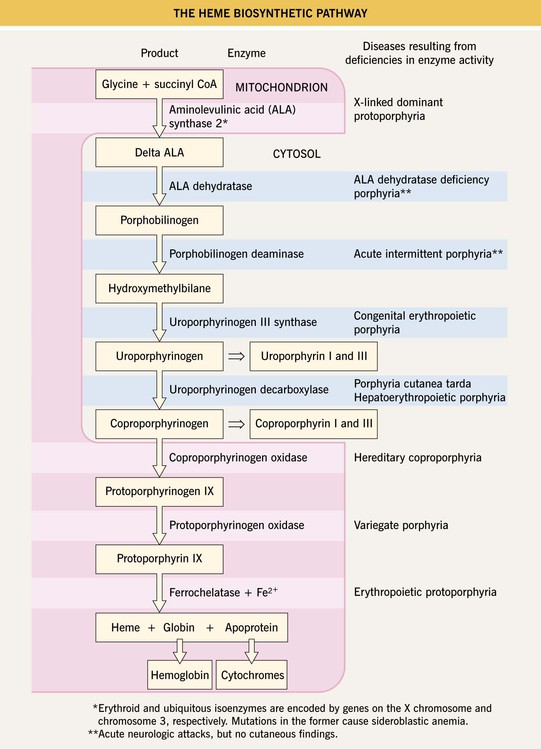
Fig. 41.1 The heme biosynthetic pathway. Courtesy, Jorge Frank, MD, and Pamela Poblete-Gutiérrez, MD.
Porphyria Cutanea Tarda (PCT)
• In addition to photosensitivity, characteristic skin findings include fragility, erosions, vesicobullae, milia, and scars in sun-exposed areas, especially on the dorsal aspects of the hand (Fig. 41.2); hypertrichosis (malar region) and hyperpigmentation can develop on the face (Fig. 41.3); morpheaform plaques are seen less often (Fig. 41.4).


Fig. 41.2 Porphyria cutanea tarda. A Marked fragility with multiple hemorrhagic crusts, erosions, and milia as well as scars. B Flaccid bulla and tense vesicle with clear fluid on the forefinger, accompanied by crusts and scars. B, Courtesy, Jorge Frank, MD, and Pamela Poblete-Gutiérrez, MD.
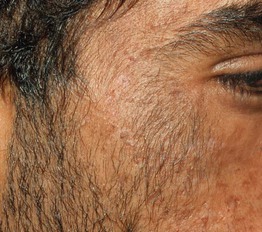
Fig. 41.3 Porphyria cutanea tarda. Hypertrichosis of the malar region of the cheek. Courtesy, Judit Stenn, MD.

Fig. 41.4 Porphyria cutanea tarda presenting as yellow-brown morpheaform plaques. The plaques were in sun-exposed areas in this patient with a history of alcohol abuse.
• DDx: pseudoporphyria due to medications (Table 41.1) or in patients with chronic kidney disease and those undergoing dialysis; phototoxic drug eruption; epidermolysis bullosa acquisita (sites of trauma but not limited to sun-exposed sites); rare forms of porphyria with similar cutaneous findings plus neurologic manifestations similar to acute intermittent porphyria (AIP) – variegate porphyria (see below) and hereditary coproporphyria (elevated coproporphyrins in feces consistently and in urine when symptomatic) – and mild forms of congenital erythropoietic porphyria.
Table 41.1
Drug-induced pseudoporphyria: most commonly incriminated medications.
The most commonly incriminated medications are in bold. For a more complete list, see Table 49.5 in Dermatology, Third Edition.
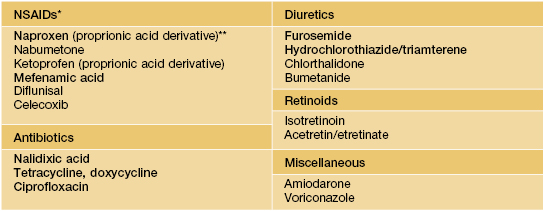
* When caused by NSAIDs, consider prescribing diclofenac, indomethacin, or sulindac.
** Most frequently implicated NSAID.
NSAID, nonsteroidal anti-inflammatory drug.
Courtesy, Misty Sharp, MD.
Erythropoietic Protoporphyria (EPP)
• Complaints of erythema, edema, and a painful burning sensation of the skin following sun exposure usually begin during early childhood; purpura and crusts may also be seen and over time, a waxy texture and scarring develop in areas of greatest cumulative UV exposure, i.e. on the nose and dorsal hands (Fig. 41.5).


Fig. 41.5 Erythropoietic protoporphyria (EPP). A Erythema, edema, and hemorrhagic crusts on the nose as well as the fingers in a young girl. B Subtle scarring on the nose and linear scars on the upper cutaneous lip in a 6-year-old child. B, Courtesy, Gillian Murphy, MD.
• DDx: solar urticaria, phototoxic or photoallergic contact dermatitis and drug reactions, hydroa vacciniforme, cutaneous LE, other causes of early onset photosensitivity (e.g. xeroderma pigmentosum, Rothmund–Thomson syndrome), and a very rare form of porphyria with similar cutaneous and hepatic findings – X-linked dominant protoporphyria.
Variegate Porphyria (VP)
Congenital Erythropoietic Porphyria (CEP)
• Over time, the degree of scarring can become marked, leading to mutilation, e.g. mitten deformities of the hand (Fig. 41.6); additional manifestations include hemolytic anemia, hepatosplenomegaly, and pink-red urine stains and pink-red teeth (erythrodontia).

Fig. 41.6 Congenital erythropoietic porphyria. Severe mutilation of the hands due to scarring. Courtesy, José Mascaro, MD.
• DDx: hepatoerythropoietic porphyria, which represents the rare autosomal recessive variant of PCT (Fig. 41.7); other causes of early onset photosensitivity (see EPP above).

Pseudoporphyria (Pseudo-PCT, Bullous Dermatosis of Dialysis)
• Seen in patients with chronic kidney disease and those undergoing dialysis, usually hemodialysis (Fig. 41.8); it is also associated with certain medications (Table 41.1).

Fig. 41.8 Dialysis-associated pseudoporphyria. Vesicles filled with clear fluid formed on the dorsal aspects of the hand in this patient with chronic kidney disease. Courtesy, Kalman Watsky, MD.
For further information see Ch. 49. From Dermatology, Third Edition.
[/level-membership-for-dermatology-category][not-level-membership-for-dermatology-category]41
Porphyrias
The porphyrias represent a group of metabolic disorders in which there is dysfunction of the enzymes involved in heme synthesis (Fig. 41.1). With the exception of acquired porphyria cutanea tarda (PCT), the underlying etiology is monogenetic mutations. Porphyrins absorb light energy (400–410 nm) and their accumulation within the skin can lead to photosensitization, with water-soluble porphyrins producing blisters and lipophilic porphyrins leading to acute burning and erythema. This chapter focuses on those porphyrias with cutaneous manifestations.
Fig. 41.1 The heme biosynthetic pathway. Courtesy, Jorge Frank, MD, and Pamela Poblete-Gutiérrez, MD.
Porphyria Cutanea Tarda (PCT)
• In addition to photosensitivity, characteristic skin findings include fragility, erosions, vesicobullae, milia, and scars in sun-exposed areas, especially on the dorsal aspects of the hand (Fig. 41.2); hypertrichosis (malar region) and hyperpigmentation can develop on the face (Fig. 41.3); morpheaform plaques are seen less often (Fig. 41.4).
Fig. 41.2 Porphyria cutanea tarda. A Marked fragility with multiple hemorrhagic crusts, erosions, and milia as well as scars. B Flaccid bulla and tense vesicle with clear fluid on the forefinger, accompanied by crusts and scars. B, Courtesy, Jorge Frank, MD, and Pamela Poblete-Gutiérrez, MD.
Fig. 41.3 Porphyria cutanea tarda. Hypertrichosis of the malar region of the cheek. Courtesy, Judit Stenn, MD.
Fig. 41.4 Porphyria cutanea tarda presenting as yellow-brown morpheaform plaques. The plaques were in sun-exposed areas in this patient with a history of alcohol abuse.
• DDx: pseudoporphyria due to medications (Table 41.1
[/not-level-membership-for-dermatology-category]
