Published on 19/03/2015 by admin
Filed under Dermatology
Last modified 22/04/2025
This article have been viewed 3881 times
Antonios Kanelleas and John Berth-Jones
Evidence Levels: A Double-blind study B Clinical trial ≥ 20 subjects C Clinical trial < 20 subjects D Series ≥ 5 subjects E Anecdotal case reports
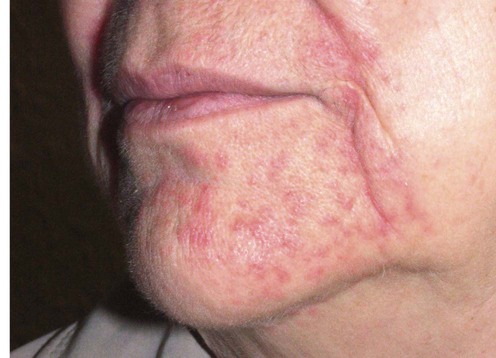
Perioral dermatitis is a persistent erythematous eruption of inflammatory papules (and sometimes pustules) on the chin, perioral areas, and nasolabial folds, characteristically sparing the skin immediately adjacent to the vermilion border. The main symptoms include pruritus, burning sensation and soreness. It is usually seen in young women, but also occurs in childhood. The etiology is unknown, however the development of perioral dermatitis is frequently preceded by intentional or inadvertent application of potent topical corticosteroids to the facial skin. The use of steroid inhalers may also induce perioral dermatitis. A similar eruption involving the eyelids and periorbital skin has been termed periocular dermatitis. The granulomatous subset of perioral dermatitis, which is seen in prepubertal children, presents with small flesh-colored or yellow-brown papules.
The suggested relationship of perioral dermatitis with infectious agents and infestations such as Candida spp, Demodex folliculorum and fusiform bacteria has not been confirmed. However, a high prevalence of atopy has been found amongst patients with perioral dermatitis.
Although sometimes described as a variant of rosacea, perioral dermatitis is distinguished from this disease by its distribution, by the relatively monomorphic appearance of the lesions, by the absence of flushing and telangiectasia, and by its tendency to occur in younger patients. Differential diagnoses also include contact dermatitis, which does not usually spare the lip margins.
Many cases are associated with the use of potent topical corticosteroids, and withdrawal of this medication is the most important measure in this group. Any cosmetic products applied on the area should also be discontinued. Patients must be warned that the condition may initially flare after this maneuvre. If the flare proves intolerable, initial use of a less potent topical corticoid can often be helpful. Systemic tetracyclines are also frequently employed, and a range of other modalities are used less frequently. In most cases there will be a permanent remission, but relapses may rarely occur. In case of treatment failure, contact dermatitis should be excluded by patch testing.
No investigation is routinely required
Guin JD. J Am Acad Dermatol 1981; 4: 417–22.
Perioral dermatitis developed following the use of topical hydrocortisone.
Although usually associated with the use of potent topical corticosteroids, this case suggests that even hydrocortisone may induce perioral dermatitis.
Macdonald A, Feiwel M. Br J Dermatol 1972; 87: 351–9.
Tetracycline 250 mg given three times daily for a week, then twice daily for 2 to 3 months, proved highly effective in this series of 29 cases.
Adams SJ, Davison AM, Cunliffe WJ, Giles GR. Br J Dermatol 1982; 106: 589–92.
A report of five cases where perioral dermatitis developed in patients on oral corticosteroids that could not be discontinued. A 2-month course of doxycycline was effective.
There are also a few recent reports that low-dose doxycycline (40 mg daily) has been useful in perioral dermatitis.
Oppel T, Pavicic T, Kamann S, Bräutigam M, Wollenberg A. J Eur Acad Dermatol Venereol 2007; 21: 1175–80.
Twenty patients were treated with topical pimecrolimus cream 1% twice a day for 4 weeks. The comparison group consisted of 20 patients treated with the vehicle compound. The Perioral Dermatitis Severity Index (PODSI) score was found to be significantly lower in the pimecrolimus group at the end of the treatment period, whereas no differences between the two groups were observed after a 4-week follow-up period.
Schwarz T, Kreiselmaier I, Bieber T, Thaci D, Simon JC, Meurer M, et al. J Am Acad Dermatol 2008; 59: 34–40.
This multicentre, double-blind trial confirmed the findings of the above-mentioned study. Patients treated with pimecrolimus also reported greater improvement in quality of life.
There are reports linking the use of topical calcineurin inhibitors with the induction of perioral dermatitis and rosacea-like eruptions after treatment for facial inflammatory dermatoses.
Wilson RG. Arch Dermatol 1979; 115: 637.
Topical tetracycline, applied twice daily, proved highly effective in this series of 30 patients. Twenty-four cleared completely after five to 28 days.
Weber K, Thurmayr R, Meisinger A. J Dermatol Treat 1993; 4: 57–9.
A comparison of the response to topical erythromycin (33 patients), oral tetracycline (35 patients), and placebo (31 patients). Oral tetracycline and topical erythromycin were comparable in efficacy and both were superior to placebo.
Bikowski JB. Cutis 1983; 31: 678–82.
Six cases cleared with topical erythromycin.
Weston WL, Morelli JG. Pediatr Dermatol 1998; 15: 144.
Two cases responded to oral erythromycin.
Veien NK, Munkvad JM, Nielsen AO, Niordson AM, Stahl D, Thormann J. J Am Acad Dermatol 1991; 24: 258–69.
A prospective, randomized, double-blind trial with 109 patients. Both groups improved, but 1% metronidazole cream applied twice daily was less effective than oxytetracycline 250 mg twice daily over 8 weeks.
Miller SR, Shalita AR. J Am Acad Dermatol 1994; 31: 847–8.
Three children with perioral or periocular eruptions were treated with topical metronidazole gel (0.75%) twice daily. Significant improvement was observed after 2 months. Complete resolution occurred after 14 weeks.
Jansen T. Br J Dermatol 2004; 151: 933–4.
Ten cases were treated with topical 20% azelaic acid cream applied twice daily. Complete clearing was reported in all cases after 2 to 6 weeks. The cream was well tolerated.
Smith KW. Cutis 1990; 46: 413–15.
Isotretinoin was used successfully in a resistant case.
Jansen T. J Eur Acad Dermatol Venereol 2002; 16: 175–7.
Successful treatment of one case of perioral dermatitis with topical adapalene gel once daily for 4 weeks. The patient had had no history of steroid use, and previous topical therapy with erythromycin had failed.
Richey DF, Hopson B. J Drugs Dermatol 2006; 5: 12–16.
Twenty-one patients participated in this prospective split-face study. One half of the face was treated with ALA-PDT once weekly for approximately 4 weeks, and the other half was treated with topical clindamycin once daily. Out of 14 patients who completed the study, the sides treated with PDT had a mean clearance of 92.1%, compared to 80.9% for the clindamycin sides (p=0.0227). The mean patient satisfaction level for PDT was also higher.
Treatment of Skin Disease Comprehensive Therapeutic Strategies 4e
WhatsApp us

 Withdrawal of topical corticoids
Withdrawal of topical corticoids Oral tetracyclines
Oral tetracyclines Topical pimecrolimus
Topical pimecrolimus Topical tetracycline
Topical tetracycline Topical erythromycin
Topical erythromycin Oral erythromycin
Oral erythromycin Topical metronidazole
Topical metronidazole Topical azelaic acid
Topical azelaic acid Oral isotretinoin
Oral isotretinoin Topical adapalene
Topical adapalene Photodynamic therapy
Photodynamic therapy
