[level-membership-for-dermatology-category]
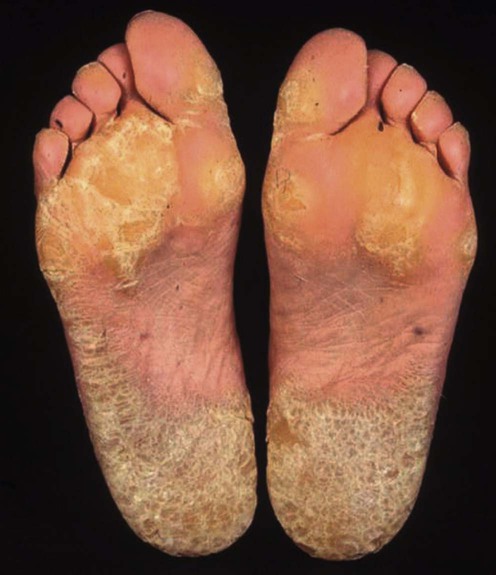
Palmoplantar keratoderma
Specific investigations


First-line therapies
 Topical keratolytics
Topical keratolytics Topical retinoids
Topical retinoidsSecond-line therapies
 Systemic retinoids
Systemic retinoidsThird-line therapies
 Reconstructive surgery with total excision of hyperkeratotic skin followed by grafting
Reconstructive surgery with total excision of hyperkeratotic skin followed by grafting Topical calcipotriol
Topical calcipotriol Oral vitamin D3 analogs
Oral vitamin D3 analogs Topical corticosteroids with or without keratolytics
Topical corticosteroids with or without keratolytics PUVA or re-PUVA
PUVA or re-PUVA Dermabrasion
Dermabrasion CO2 laser
CO2 laser 5-Fluorouracil
5-Fluorouracil Tyrosine-restricted diet in oculocutaneous keratoderma
Tyrosine-restricted diet in oculocutaneous keratoderma[/level-membership-for-dermatology-category][not-level-membership-for-dermatology-category]
Palmoplantar keratoderma
Specific investigations
